(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session A: Prostate Cancer. Dr. Rana R. McKay presented Poster 158: ctDNA dynamics in bone-dominant mCRPC treated with radium-223 with or without olaparib: Biomarker analyses from the multicenter, randomized, phase 2, investigator-initiated COMRADE trial.
Dr. McKay began by reminding the audience that the COMRADE study previously demonstrated a significant improvement in radiographic progression-free survival (rPFS) with the addition of olaparib to radium-223. Given the growing interest in biomarkers to guide treatment selection in mCRPC, this analysis focused on early ctDNA dynamics and PSA responses and their association with clinical outcomes.1
The COMRADE trial (NCT03317392), a multicenter, randomized, open-label phase II study conducted through the NCI Experimental Therapeutics Clinical Trials Network. Patients with metastatic castration-resistant prostate cancer were randomized 1:1 to receive radium-223 (55 kBq/kg IV every 4 weeks for up to 6 cycles) plus olaparib (200 mg orally twice daily) or radium-223 alone. Randomization was stratified by prior docetaxel exposure and extent of bone disease (≤20 vs >20 bone lesions), and crossover to olaparib was permitted at progression.
Eligible patients had mCRPC with at least two bone metastases, no visceral metastases, lymph nodes <4 cm, ECOG performance status 0–1, and no prior PARP inhibitor or radium-223 exposure. Correlative circulating tumor DNA analyses were performed using banked plasma samples sequenced with FoundationOne Monitor (research-use assay). Circulating DNA tumor fraction was measured at cycle 1 day 1 and cycle 2 day 1. A molecular response was defined as a ≥50% decrease in tumor fraction from baseline, and patients with undetectable circulating tumor DNA at both time points were categorized as persistent negatives. Radiographic progression-free survival and overall survival were analyzed using Kaplan-Meier methods and Cox proportional hazards models, landmarked from the date of sample collection. PSA response (PSA50) was defined as a ≥50% decline from baseline.
Of 133 enrolled patients, 113 were eligible for inclusion after excluding those who did not initiate treatment, were not randomized, or lacked required baseline samples. Nineteen additional patients were excluded due to missing cycle 2 samples or progression prior to the landmark analysis, leaving 94 patients for the cycle 2 day 1 ctDNA analysis (49 in the radium-223 plus olaparib arm and 45 in the radium-223 alone arm). For the change-from-baseline analysis, further exclusions due to missing cycle 1 samples or unquantifiable ctDNA changes resulted in 36 evaluable patients in the combination arm and 41 in the radium-223 alone arm.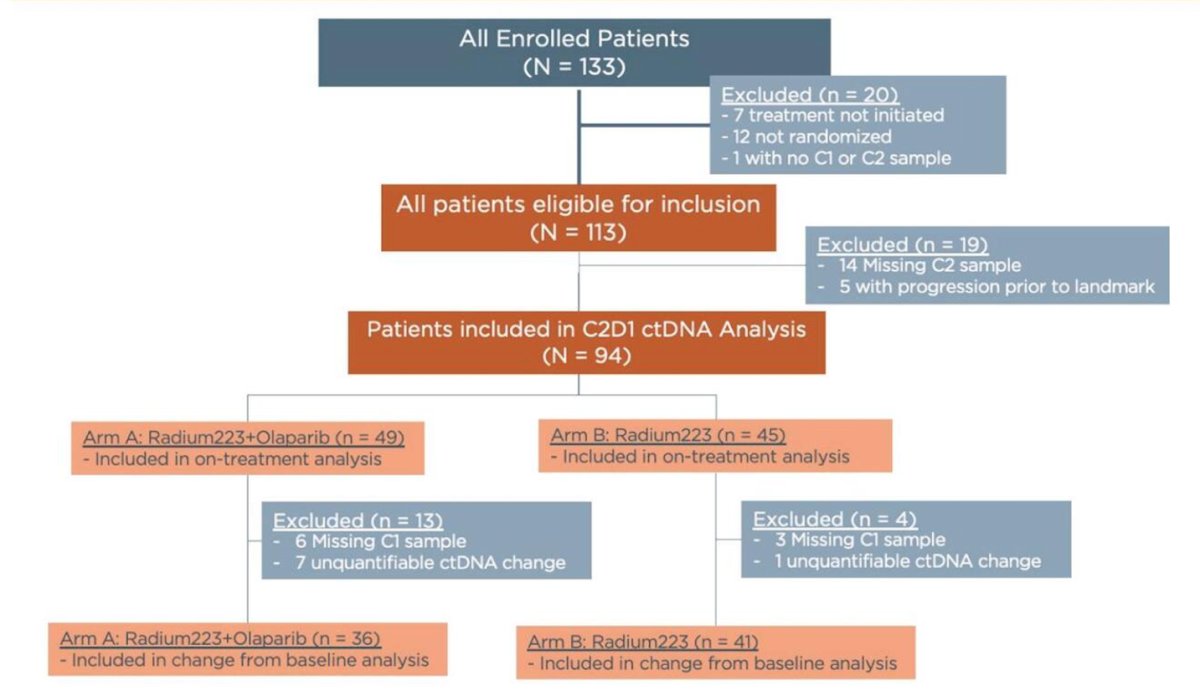
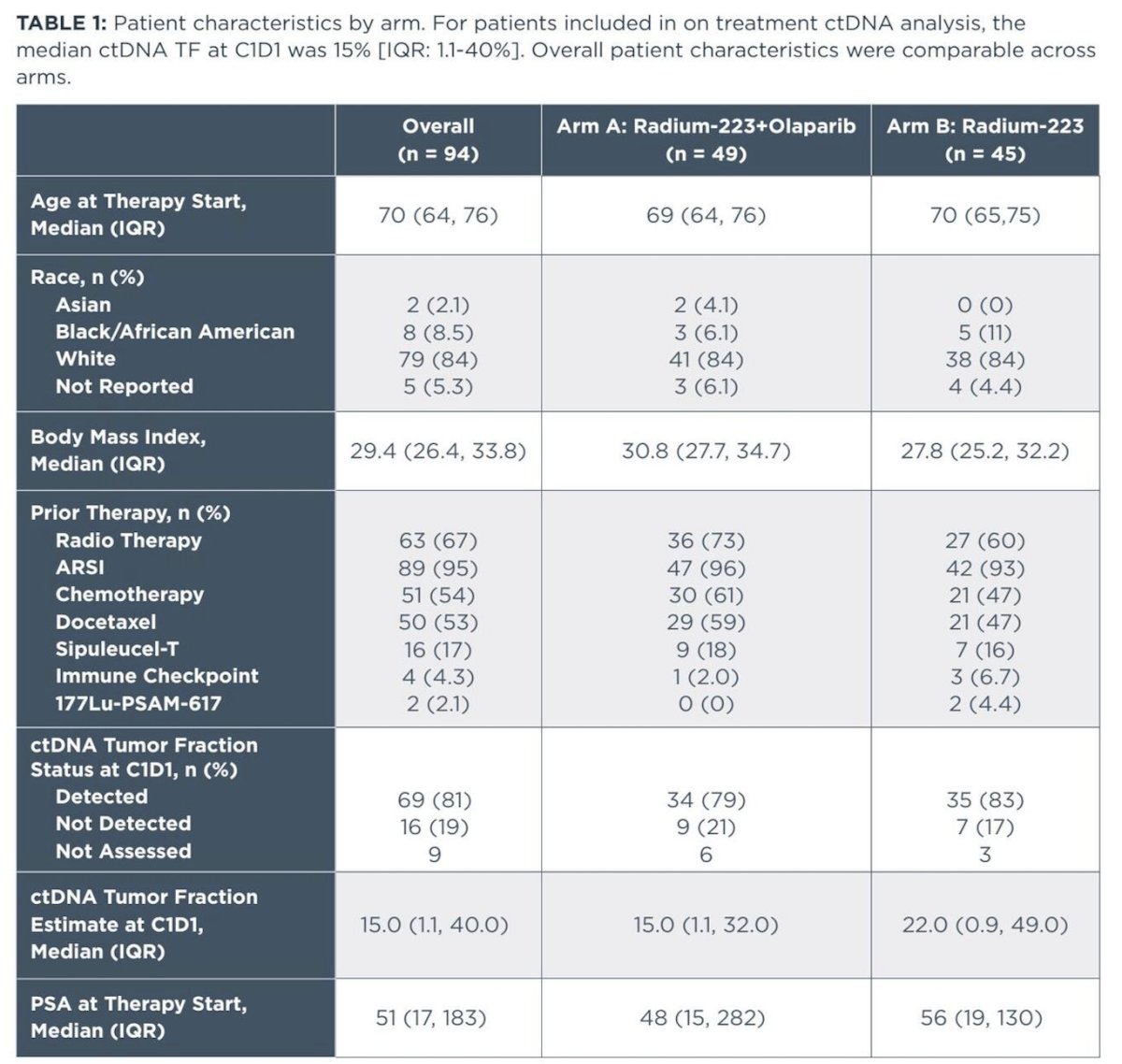
Among the 94 patients included in the on-treatment ctDNA analysis, baseline characteristics were well balanced between the radium-223 plus olaparib arm (n=49) and the radium-223 alone arm (n=45). Median age was 70 years overall, and most patients were White (84%). Median body mass index was 29.4 kg/m². Prior therapies were common, including prior ARSI in 95%, chemotherapy in 54%, docetaxel in 53%, and prior radiotherapy in 67%, with similar distributions across arms. At cycle 1 day 1, ctDNA tumor fraction was detectable in 81% of patients overall, with a median tumor fraction of 15% (IQR 1.1–40.0), and comparable values between treatment groups. Median baseline PSA was 51 ng/mL overall, again similar across arms as illustrated in the table below.
Radiographic progression-free survival was strongly associated with ctDNA tumor fraction status at cycle 2 day 1. In the overall cohort, patients with detectable ctDNA had a median rPFS of 2.7 months (95% CI 1.8–5.1), whereas those with undetectable ctDNA had a median rPFS of 9.9 months (95% CI 7.7–14.3), corresponding to a hazard ratio of 0.47 (95% CI 0.28–0.79). This pattern was consistent across treatment arms. In the radium-223 plus olaparib arm, median rPFS was 5.4 months (95% CI 2.0–12.5) in ctDNA-positive patients versus 12.4 months (95% CI 10.2–not reached) in ctDNA-negative patients (HR 0.38; 95% CI 0.15–0.91). In the radium-223 alone arm, median rPFS was 2.0 months (95% CI 1.8–4.3) in ctDNA-positive patients compared with 7.5 months (95% CI 4.6–not reached) in ctDNA-negative patients (HR 0.35; 95% CI 0.17–0.71), supporting ctDNA clearance as a strong on-treatment prognostic marker.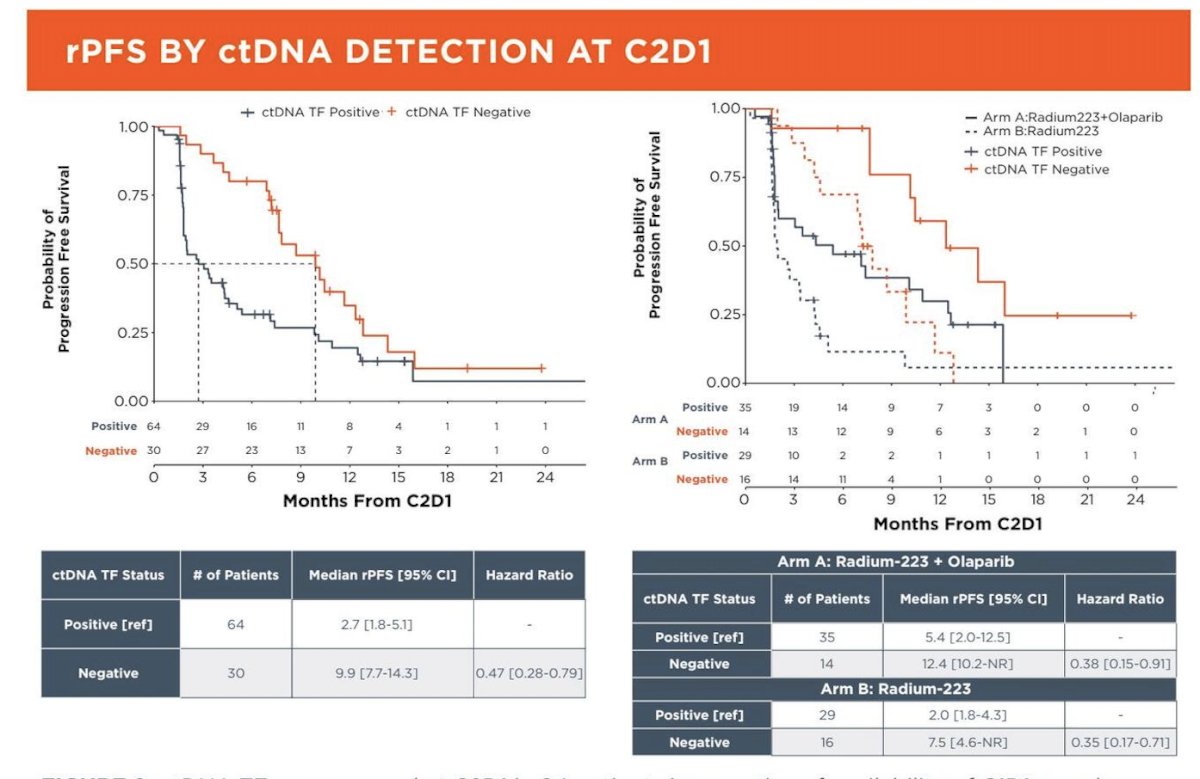
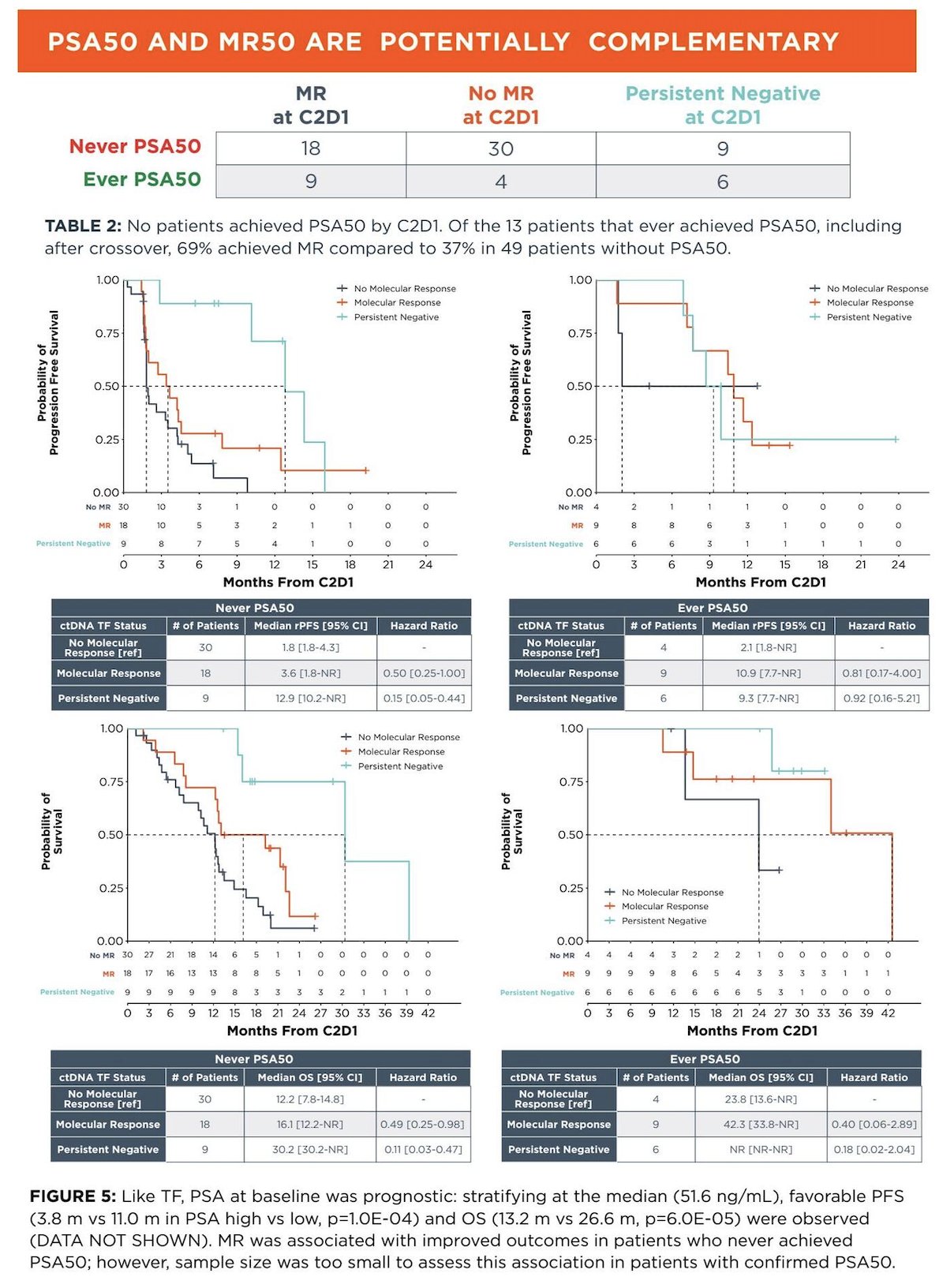
Baseline PSA was also prognostic. When stratified at the median baseline PSA of 51.6 ng/mL, patients with lower PSA had significantly improved radiographic progression-free survival (11.0 vs 3.8 months, p=1.0×10⁻⁴) and overall survival (26.6 vs 13.2 months, p=6.0×10⁻⁵) compared with those with higher PSA.
In addition, PSA50 and molecular response (MR50) appeared potentially complementary. No patients achieved PSA50 by cycle 2, day 1. Among the 13 patients who eventually achieved PSA50 (including after crossover), 69% achieved a molecular response compared with 37% among patients who never achieved PSA50.
In patients who never achieved PSA50, ctDNA dynamics were strongly prognostic. Median rPFS was 1.8 months in those without molecular response, 3.6 months in those with molecular response (HR 0.50), and 12.9 months in patients with persistent negative ctDNA (HR 0.15). Similarly, median OS was 12.2 months without molecular response, 16.1 months with molecular response (HR 0.49), and 30.2 months in those with persistent negative ctDNA (HR 0.11).
Among patients who achieved PSA50, outcomes were numerically improved but limited by a small sample size. Median rPFS was 2.1 months without molecular response, versus 10.9 months with molecular response and 9.3 months in persistent negative patients. Median OS was 23.8 months without molecular response, 42.3 months with molecular response (HR 0.40), and not reached in those with persistent negative ctDNA.
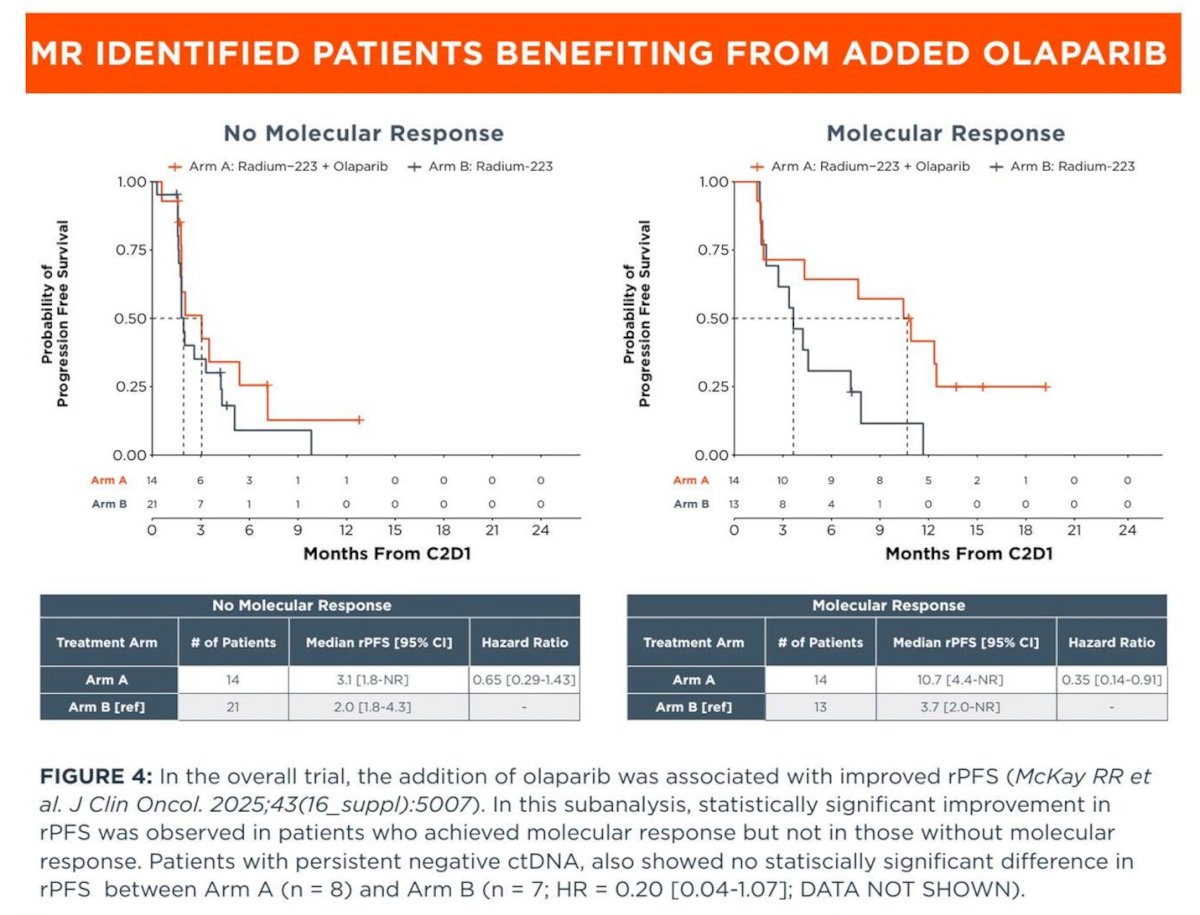
Lastly, molecular response identified patients most likely to benefit from the addition of olaparib. Among patients without molecular response at C2D1, median rPFS was similar between arms (3.1 months with radium-223 + olaparib vs 2.0 months with radium-223 alone; HR 0.65), indicating limited incremental benefit. In contrast, among patients who achieved molecular response, the addition of olaparib was associated with a marked improvement in rPFS (10.7 vs 3.7 months; HR 0.35), supporting ctDNA dynamics as a predictive biomarker of PARP inhibitor benefit. Patients with persistently negative ctDNA also demonstrated favorable outcomes, with no statistically significant difference between treatment arms, suggesting this subgroup may derive less additional benefit from treatment intensification.
Dr. McKay concluded her presentation with the following key takeaways:
- Early ctDNA dynamics at C2D1 were strongly prognostic, with molecular response and persistent ctDNA negativity correlating closely with improved rPFS and OS, whereas no PSA50 responses were observed by C2D1, highlighting the limited utility of early PSA kinetics in this setting.
- Achievement of PSA50 at any time point was associated with improved clinical outcomes, although this may partially reflect survival bias; molecular response was more frequent among patients who ultimately achieved PSA50, suggesting complementary but temporally distinct biomarker value.
- The addition of olaparib to radium-223 appeared to confer greater rPFS benefit among patients who achieved a molecular response.
- Early on-treatment ctDNA dynamics may represent a valuable biomarker to guide treatment decisions in patients with bone-dominant mCRPC receiving radium-223-based therapy.
Presented by: Rana McKay, MD, Medical Oncologist, Clinical Professor of Medicine, UC San Diego School of Medicine, San Diego, CA
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Reference: