(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session A: Prostate Cancer. Dr. Rahul A. Parikh presented Poster 161: A phase 1/2 study of MRT-2359, a highly selective oral GSPT1 molecular glue degrader, in combination with enzalutamide in mCRPC harboring AR ligand binding domain mutations.
Dr. Parikh began by emphasizing that progression to mCRPC is driven by multiple resistance mechanisms, including the emergence of AR LBD mutations that reactivate AR signaling and reduce responsiveness to novel hormonal agents (NHAs). MRT-2359 is an orally bioavailable, highly selective degrader of the translation termination factor GSPT1. Preclinical studies have demonstrated that degradation of GSPT1 reduces the cellular abundance of oncogenic proteins, including AR, MYC, and Cyclin D1, leading to robust anti-tumor activity in mCRPC models, both as monotherapy and in combination with enzalutamide.
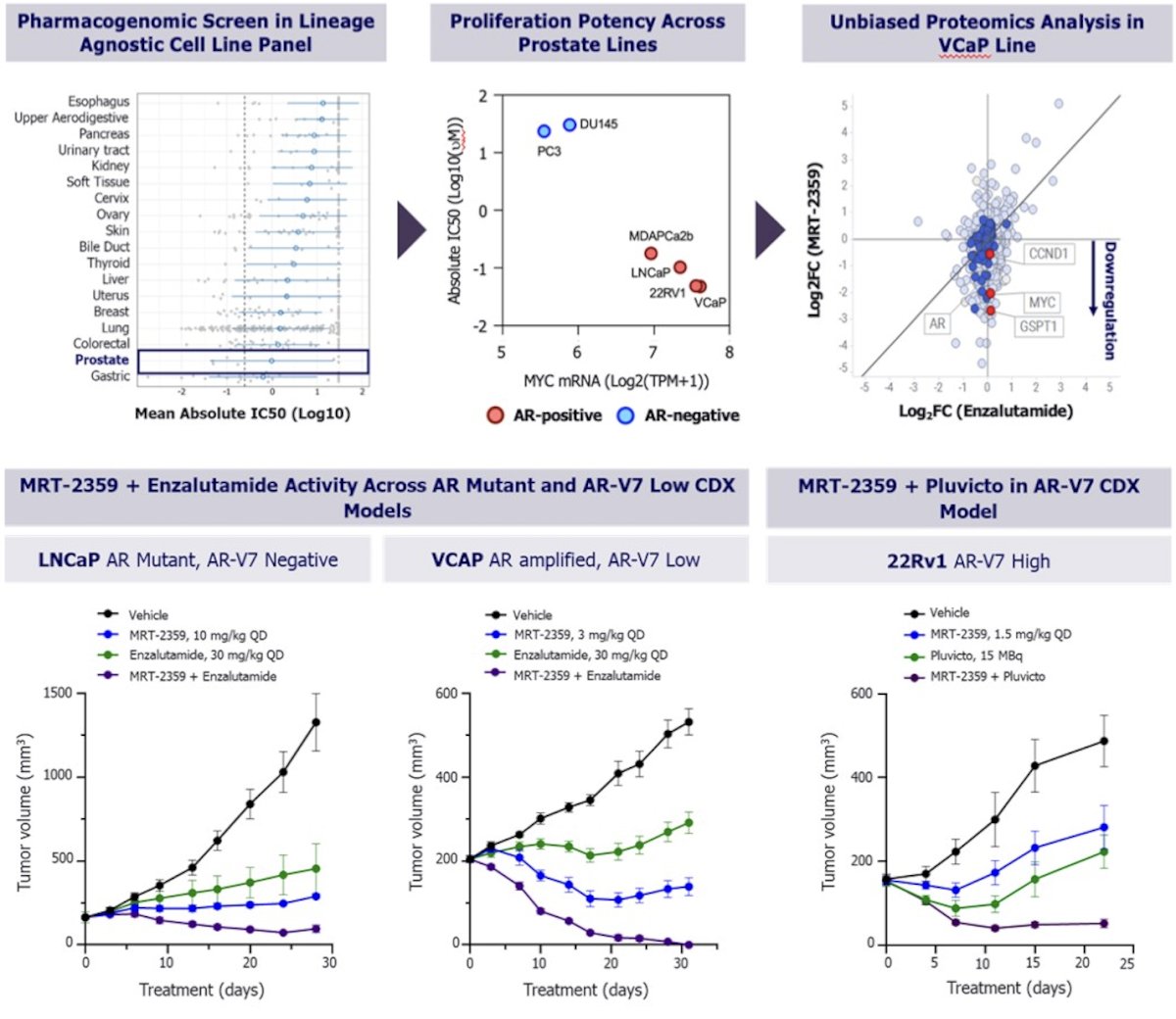
Dr. Parikh presented preclinical data evaluating MRT-2359, a novel MYC-targeting agent, across prostate cancer models. In a lineage-agnostic pharmacogenomic screen, prostate cancer cell lines emerged among the most sensitive tumor types. Across prostate models, anti-proliferative potency correlated with MYC mRNA expression, with greater activity observed in MYC-high, AR-positive lines. Unbiased proteomic analysis in VCaP cells demonstrated downregulation of key oncogenic drivers following MRT-2359 exposure, including AR, CCND1, MYC, and GSPT1, supporting broad suppression of AR-dependent and AR-independent signaling pathways.
In vivo, MRT-2359 demonstrated significant antitumor activity both as monotherapy and in combination strategies. In LNCaP (AR mutant, AR-V7 negative) and VCaP (AR amplified, AR-V7 low) xenograft models, the combination of MRT-2359 with enzalutamide resulted in enhanced tumor growth inhibition compared with either agent alone. In the 22Rv1 AR-V7–high model, combining MRT-2359 with Pluvicto further suppressed tumor growth relative to monotherapy arms. Collectively, these data support MRT-2359 as a promising therapeutic strategy in MYC-driven and AR-dependent prostate cancer, with potential synergy across hormonal and radioligand treatment modalities.
MRT-2359 was first evaluated in an open-label dose-escalation study assessing safety, dose-limiting toxicities (DLTs), pharmacokinetics, pharmacodynamics, and preliminary efficacy across multiple tumor types. In the monotherapy dose-escalation portion, 59 patients received MRT-2359 at doses ranging from 0.5 mg to 2 mg daily on either a 5 days on/9 days off (5/9) or 21 days on/7 days off (21/7) schedule. The recommended phase II dose was established at 0.5 mg on the 21/7 schedule. The clinical study design is shown below.
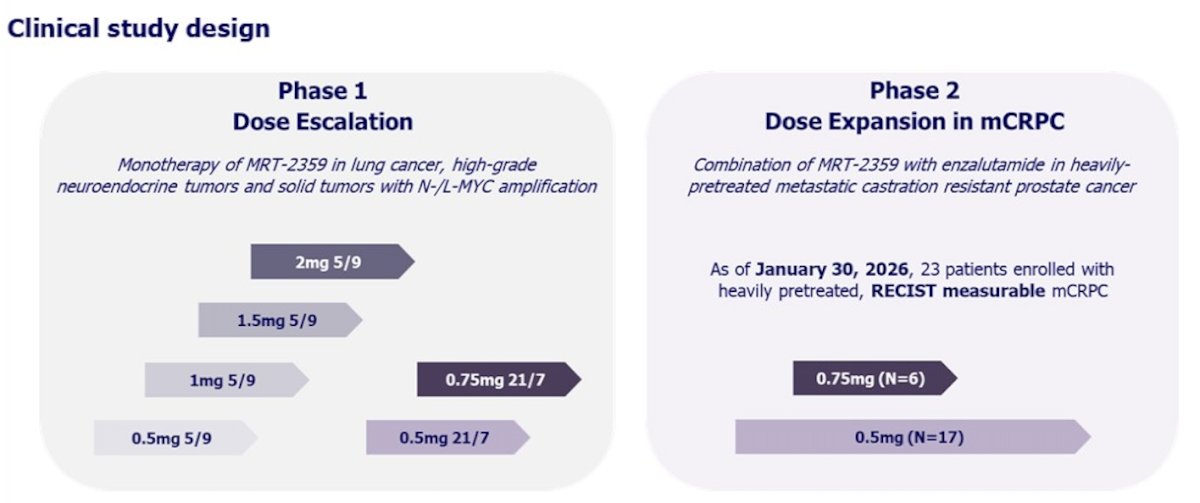
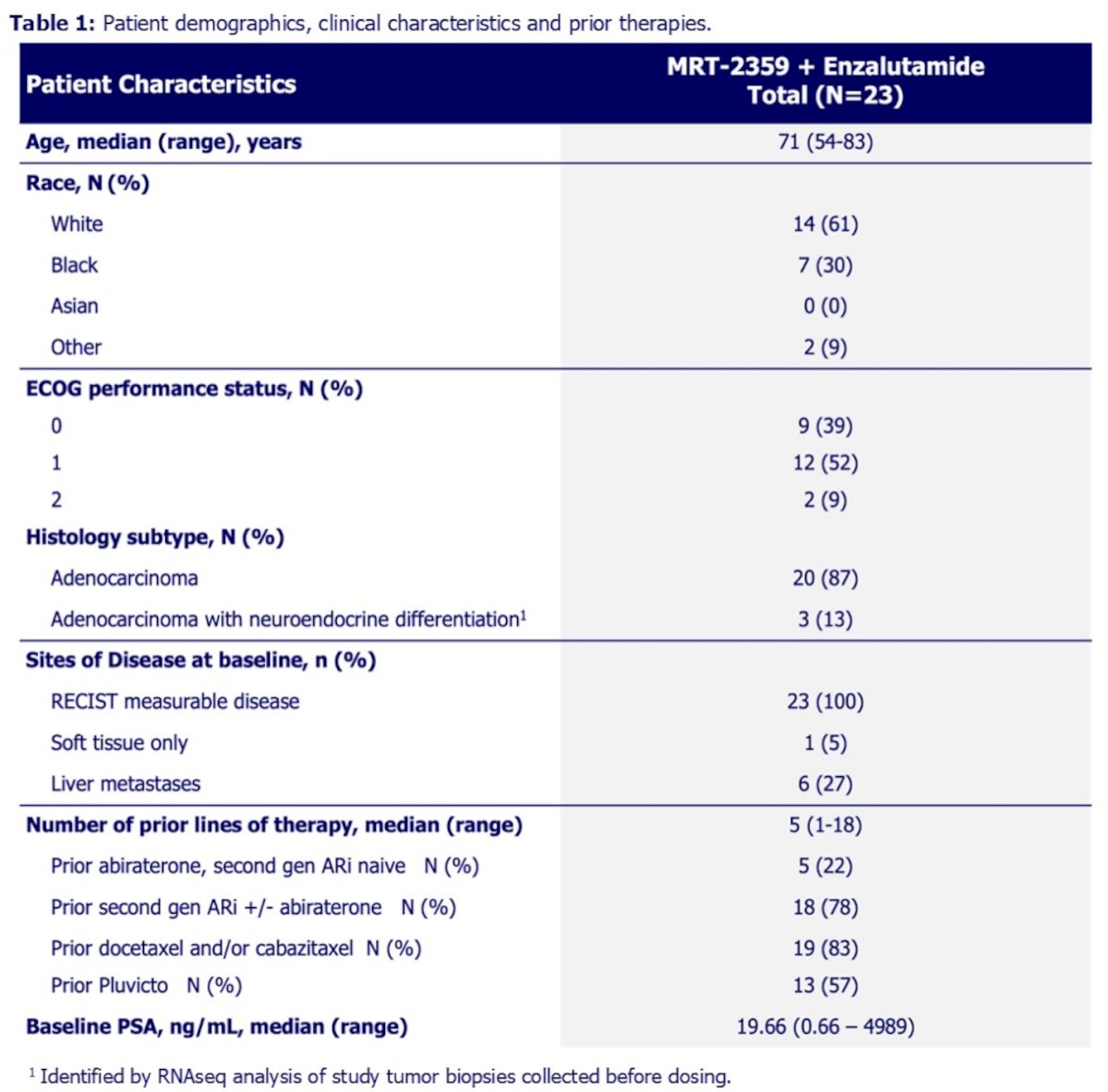
As of January 30, 2026, 23 heavily pretreated patients had received MRT-2359 in combination with enzalutamide, and 4 patients (17%) remained on therapy at data cutoff. No treatment discontinuations occurred due to adverse events, supporting the tolerability of the regimen in this advanced population.
Treatment discontinuations were primarily driven by disease progression, with 13 patients (68%) stopping therapy due to radiologic or clinical progression. Other reasons included withdrawal of consent in 3 patients (16%), development of an intercurrent medical condition in 1 patient (5%), investigator decision in 1 patient (5%), and death in 1 patient (5%).
One patient (4%) experienced a dose-limiting toxicity consisting of grade 3 stomatitis associated with pain. Adverse events suspected to be drug-related and occurring in ≥20% of patients are summarized in Table 2. The most common treatment-related adverse events were fatigue (n=12, 52%), diarrhea (n=11, 48%), and nausea (n=8, 35%). These events were predominantly grade 1–2, manageable, and not treatment-limiting.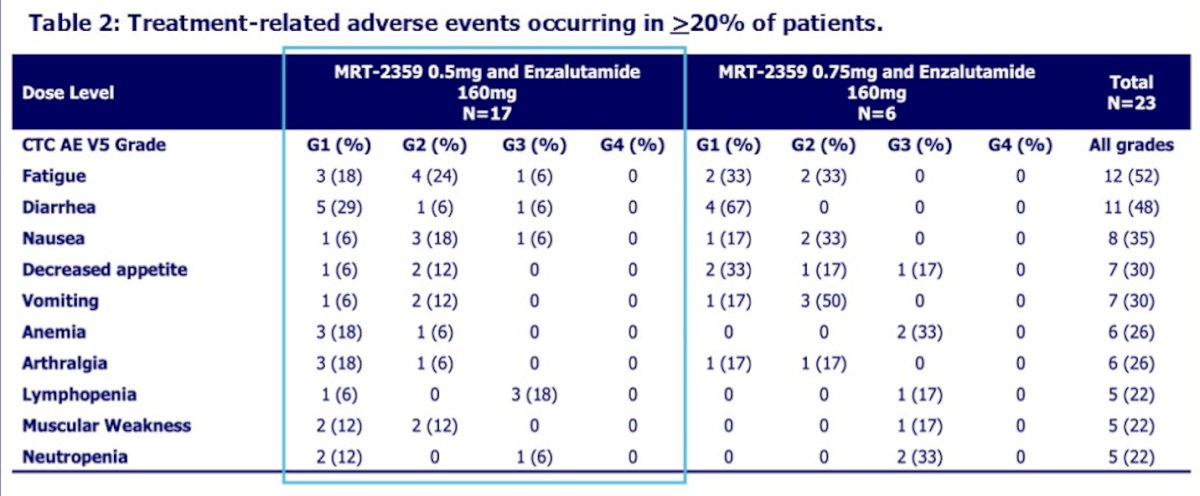
Dr. Parikh noted that, based on the favorable safety profile and encouraging clinical activity observed, the 0.5 mg 21/7 dosing schedule was prioritized for the remainder of the phase 2 expansion.
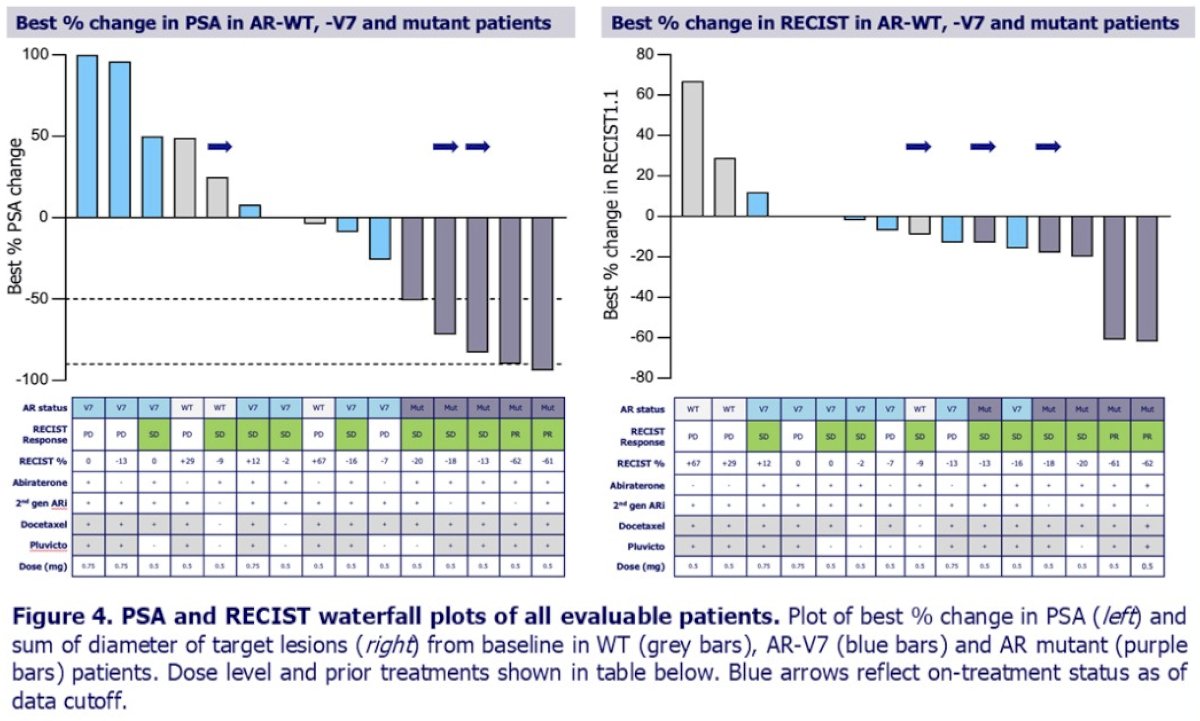
As of the January 30, 2026, data cutoff, 33% of patients (5/15) achieved a PSA response, 13% (2/15) achieved a RECIST partial response, and the overall disease control rate was 67% (10/15). Tumor shrinkage of target lesions was observed in 10 patients, supporting meaningful antitumor activity in this heavily pretreated population.
In a predefined subset of 5 heavily pretreated patients with AR mutations, responses were particularly notable. All 5 patients (100%) achieved a PSA response, including 2 PSA90 and 3 PSA50 responses. Two of five patients demonstrated RECIST partial responses (1 confirmed, 1 unconfirmed), while the remaining 3 had stable disease, resulting in a 100% disease control rate. Two patients remained on therapy for 10 cycles or longer, and 2 of 5 patients continued treatment at the time of data cutoff, further supporting the durability of benefit in this molecularly defined subgroup.
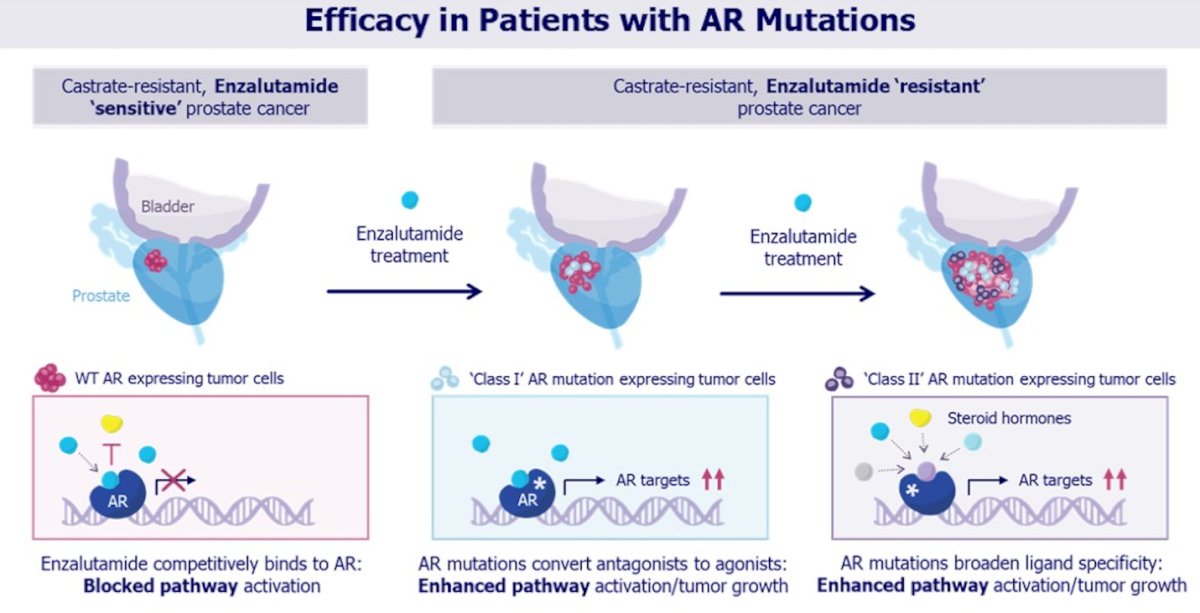
Dr. Parikh further highlighted the biological rationale for targeting AR-mutant disease, outlining two functional classes of therapy-resistant AR mutations that emerge with prolonged AR antagonist exposure. Class I mutations convert AR antagonists into agonists, enhancing AR pathway activation despite enzalutamide. Class II mutations broaden ligand specificity, allowing AR activation by alternative steroid hormones and serving as potential surrogates of heightened AR pathway signaling. These resistance mechanisms provide a strong rationale for evaluating MRT-2359 in AR-mutant prostate cancer.
Clinically, all five patients with AR mutations demonstrated meaningful activity across multiple efficacy endpoints. Each patient achieved a PSA response, with substantial PSA declines observed. Two of five patients achieved RECIST partial responses, and three had stable disease. Tumor shrinkage was mirrored by significant reductions in mutant allele frequency in ctDNA and declines in circulating tumor cell counts in 4 of 5 evaluable patients. Notably, two patients remained on therapy at data cutoff, supporting the durability of response in this molecularly defined subgroup.
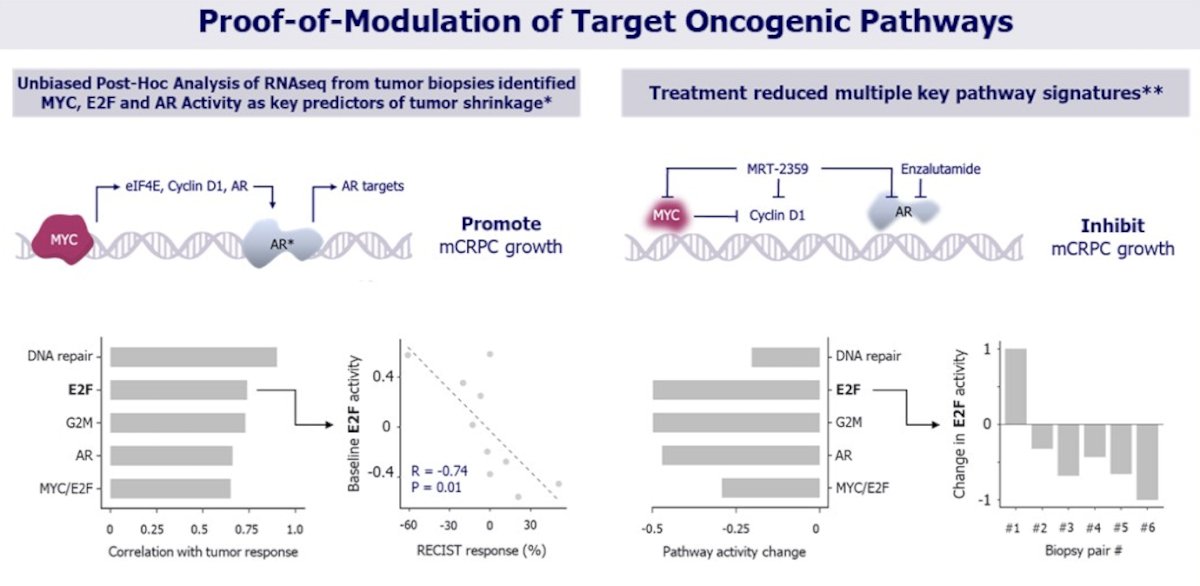
Dr. Parikh presented translational evidence of target modulation demonstrating that baseline activation of MYC, E2F, AR, DNA repair, and G2M pathways in pre-treatment biopsies correlated with tumor response, with higher baseline E2F activity significantly associated with greater RECIST tumor shrinkage (R = −0.74, p = 0.01). Importantly, paired on-treatment biopsies showed coordinated downregulation of these same oncogenic signatures, including MYC/E2F and AR signaling, confirming pharmacodynamic suppression of key proliferative and AR-driven pathways. Together, these data provide molecular proof-of-mechanism supporting the clinical activity observed with MRT-2359 in combination with enzalutamide.
Dr. Parikh concluded his presentation with the following key takeaways:
- MRT-2359 plus enzalutamide was well tolerated in patients with mCRPC, with adverse events manageable; the most common drug-related events were fatigue, diarrhea, nausea, and decreased appetite.
- Among evaluable patients, the overall RECIST disease control rate was 67% (10/15), with 10 of 15 patients demonstrating reductions in target lesion size.
- In the AR-mutant subset (n=5), compelling activity was observed, including 100% PSA50/90 response, 40% RECIST partial response, and 100% RECIST disease control rate.
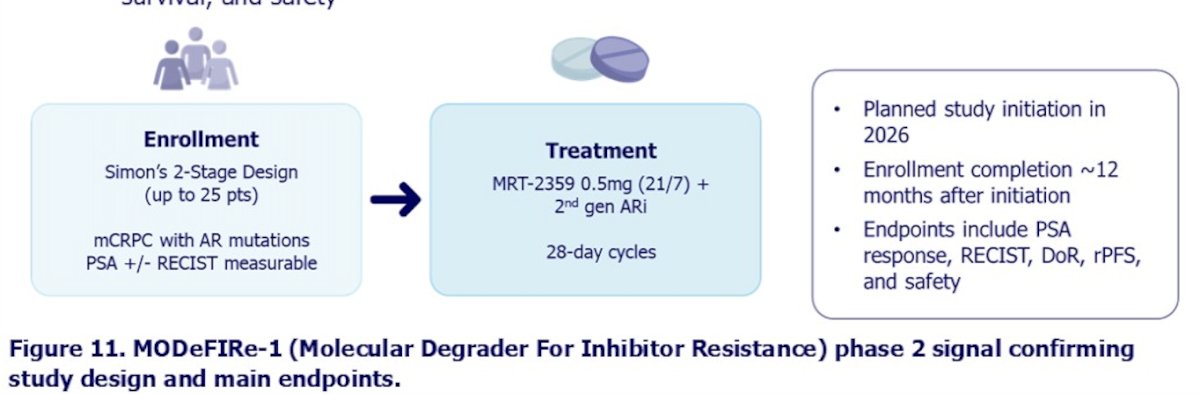
- Based on the efficacy signal in AR-mutant patients, a signal-confirming phase 2 study of MRT-2359 in combination with a second-generation AR inhibitor will be pursued in this molecularly defined population.
- Planned enrollment is up to 25 patients with mCRPC harboring AR mutations.
- Future expansion may include additional patient subsets, such as those naïve to second-generation AR inhibitors and/or combination strategies with other agents.
- Key phase 2 endpoints will include PSA response, RECIST response, duration of response, radiographic progression-free survival, and safety (Study design below)
Presented by: Rahul A. Parikh, MD, PhD, Professor of Medicine, University of Kansas, Kansas City, KS
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.