(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session A: Prostate Cancer. Dr. Manish R. Patel presented Poster 171: Safety and efficacy of pasritamig + docetaxel in participants with metastatic castration resistant prostate cancer (mCRPC): Initial results of a phase 1b study.
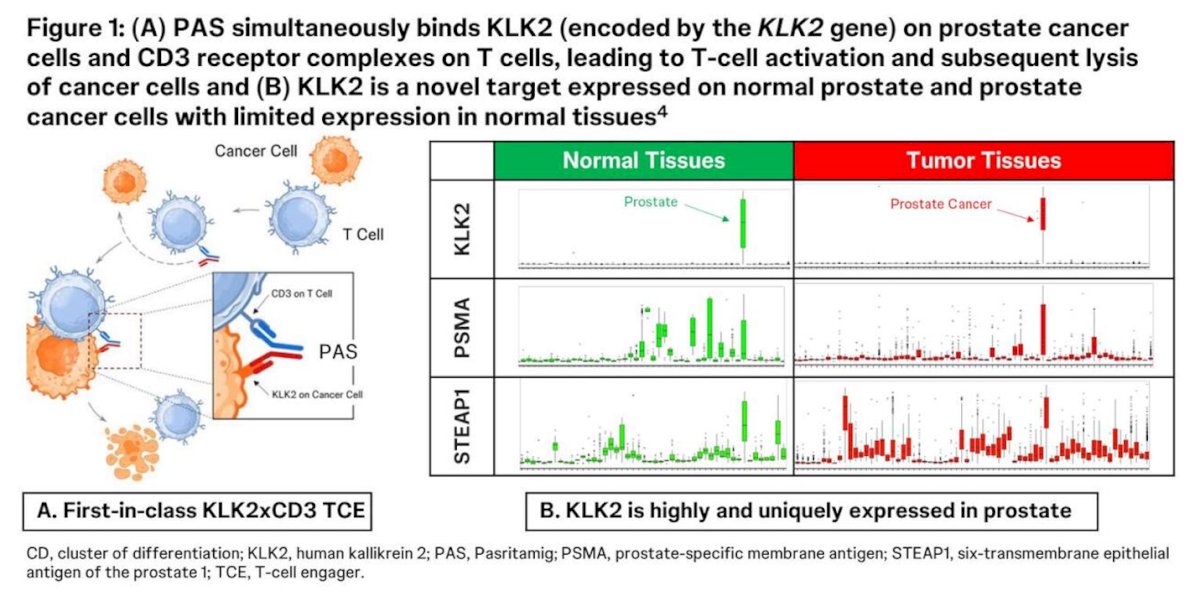
Dr. Patel began by noting that docetaxel remains a standard of care for patients with mCRPC following androgen receptor pathway inhibitor (ARPI) failure. However, improved therapeutic strategies are needed. Pasritamig is a first-in-class bispecific T-cell engager that binds CD3 on T cells and human kallikrein 2 (KLK2), a protein highly and specifically expressed in prostate tissue and prostate cancer cells (As shown in the figure below.
In a prior first-in-human Phase 1 study, PAS demonstrated manageable toxicity with less than 10% Grade 1 cytokine release syndrome (CRS), outpatient dosing every six weeks, and encouraging single-agent activity in heavily pretreated mCRPC.1
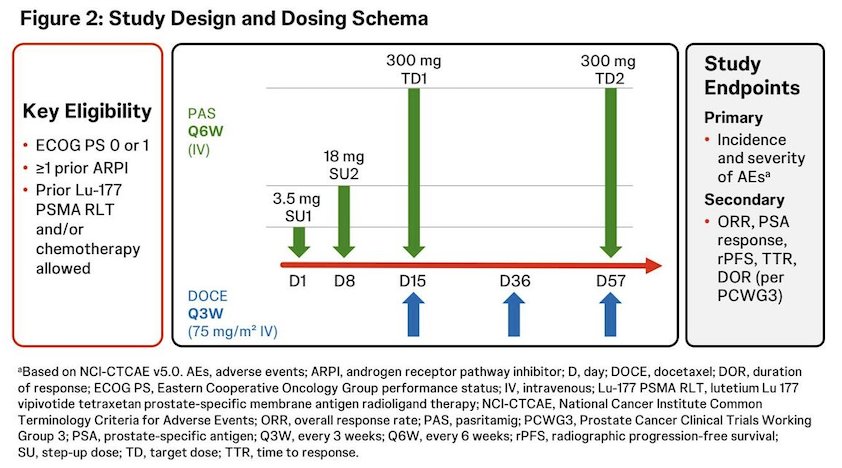
This open-label Phase 1b study (NCT05818683) aimed to determine the recommended Phase 2 regimen of PAS combined with docetaxel based on safety. PAS was administered at the recommended Phase 2 regimen of 300 mg IV every six weeks, with step-up dosing (3.5 mg on Day 1 and 18 mg on Day 8). Docetaxel was given at 75 mg/m² IV every three weeks starting on Day 15. Treatment was delivered in the outpatient setting. Corticosteroids were not routinely administered except as docetaxel premedication, and hematopoietic growth factor support was permitted. The study design is shown below.
As of December 9, 2025, 51 patients had received at least one dose of PAS plus docetaxel. The median age was 70 years, and 33% had visceral metastases. Patients were heavily pretreated, with a median of three prior lines of therapy, including prior ARPI (100%), docetaxel (43%), cabazitaxel (22%), and lutetium-177 vipivotide tetraxetan (20%). The median duration of combination therapy was 3.5 months, and 31 of 51 patients remained on treatment at the time of analysis.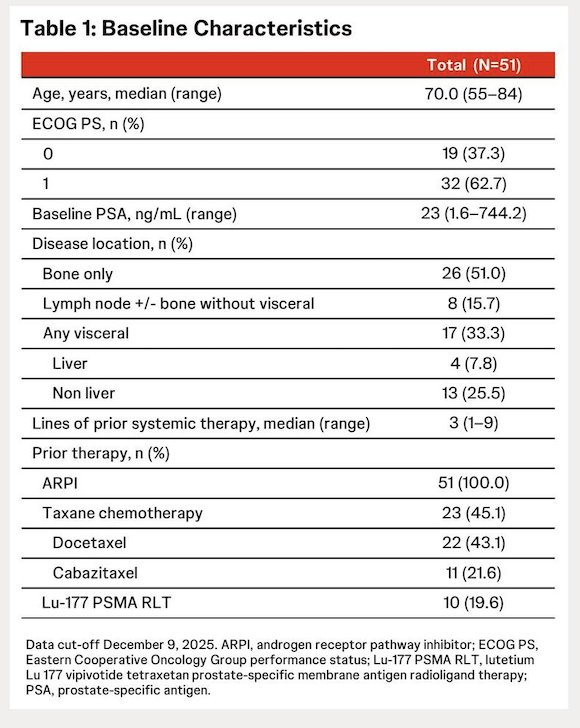
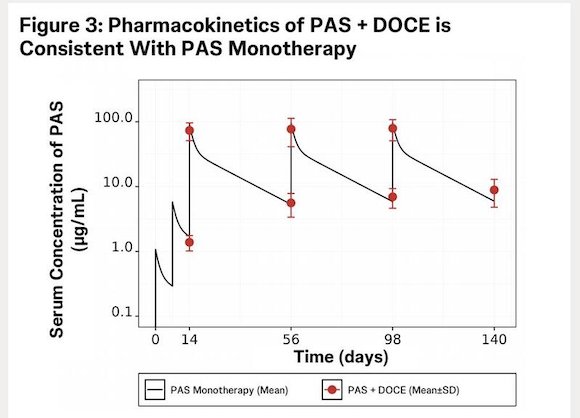
Dr. Patel highlighted that pharmacokinetic analyses demonstrated PAS serum concentrations measured at pre-dose and end-of-infusion—approximating trough and Cmax levels (N=50) following the 300 mg every-6-week dosing schedule in combination with docetaxel were comparable to those observed with PAS monotherapy, indicating no clinically meaningful drug–drug interaction.
PAS and docetaxel were readily combinable at their full monotherapy doses without observed dose-limiting toxicities. Treatment-related adverse events were consistent with the known safety profile of docetaxel in mCRPC. The most frequent adverse events occurring in more than 20% of patients included fatigue (60.8%), alopecia (41.2%), diarrhea (31.4%), nausea (31.4%), peripheral edema (27.5%), peripheral sensory neuropathy (25.5%), and dysgeusia (23.5%). PAS-related adverse events occurred in 60.8% of patients, most commonly fatigue (33.3%) and non-chronic diarrhea (11.8%). Importantly, no patients experienced CRS of any grade.
Grade 3 or higher treatment-related adverse events occurred in 29.4% of patients. Treatment-related serious adverse events were reported in 13.7%, and treatment discontinuation due to adverse events occurred in 13.7%, with only one case attributed to PAS. There were no fatal treatment-related adverse events.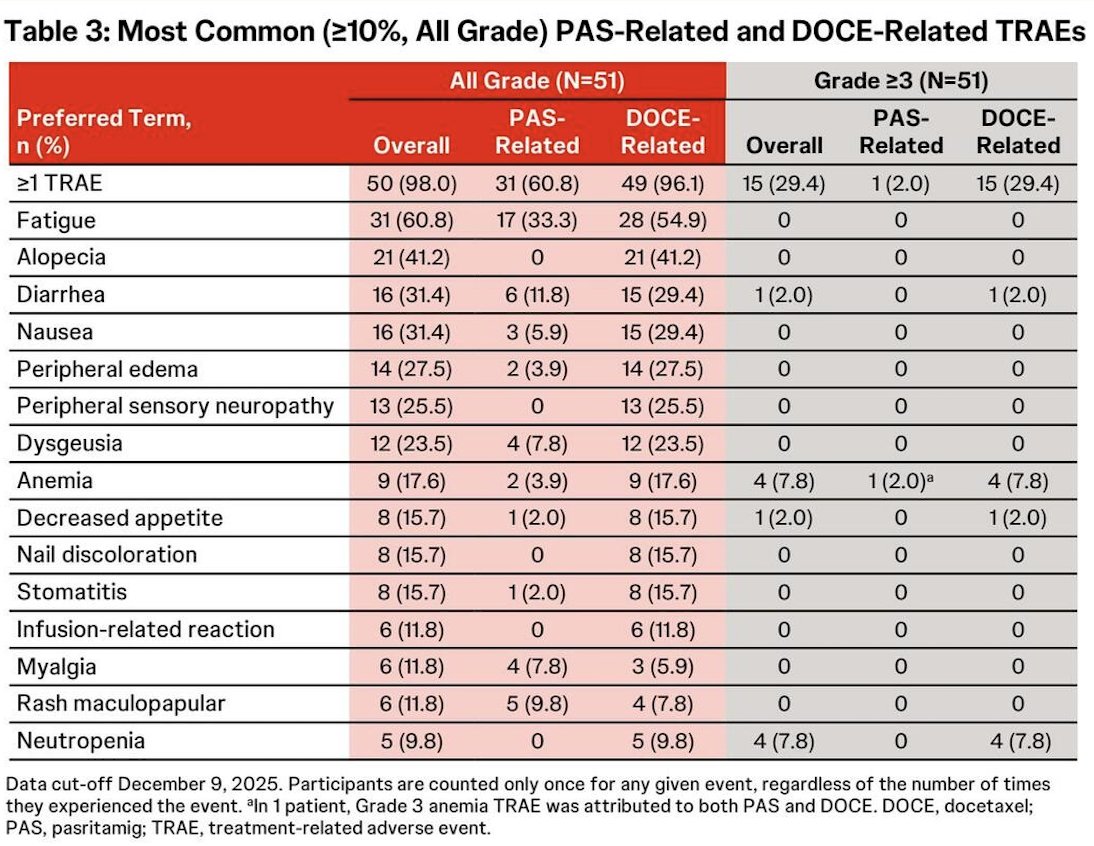
Overall, confirmed PSA responses were robust, with PSA50 and PSA90 response rates of 64.7% (33/51) and 39.2% (20/51), respectively. When stratified by disease extent, the taxane-naïve, bone-only subgroup demonstrated the highest activity, with confirmed PSA50 responses in 88.2% (15/17) and PSA90 responses in 76.5% (13/17) of patients.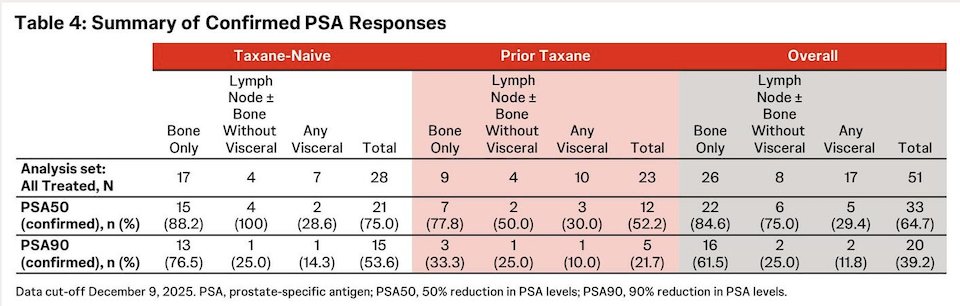
Importantly, PSA50 and PSA90 responses, along with disease control, were observed even among patients with prior taxane exposure. Among those with RECIST-measurable disease, the overall response rate was 28.6% (2/7) in the non-visceral subgroup and 6.7% (1/15) in patients with any visceral metastases, as detailed in the figures below.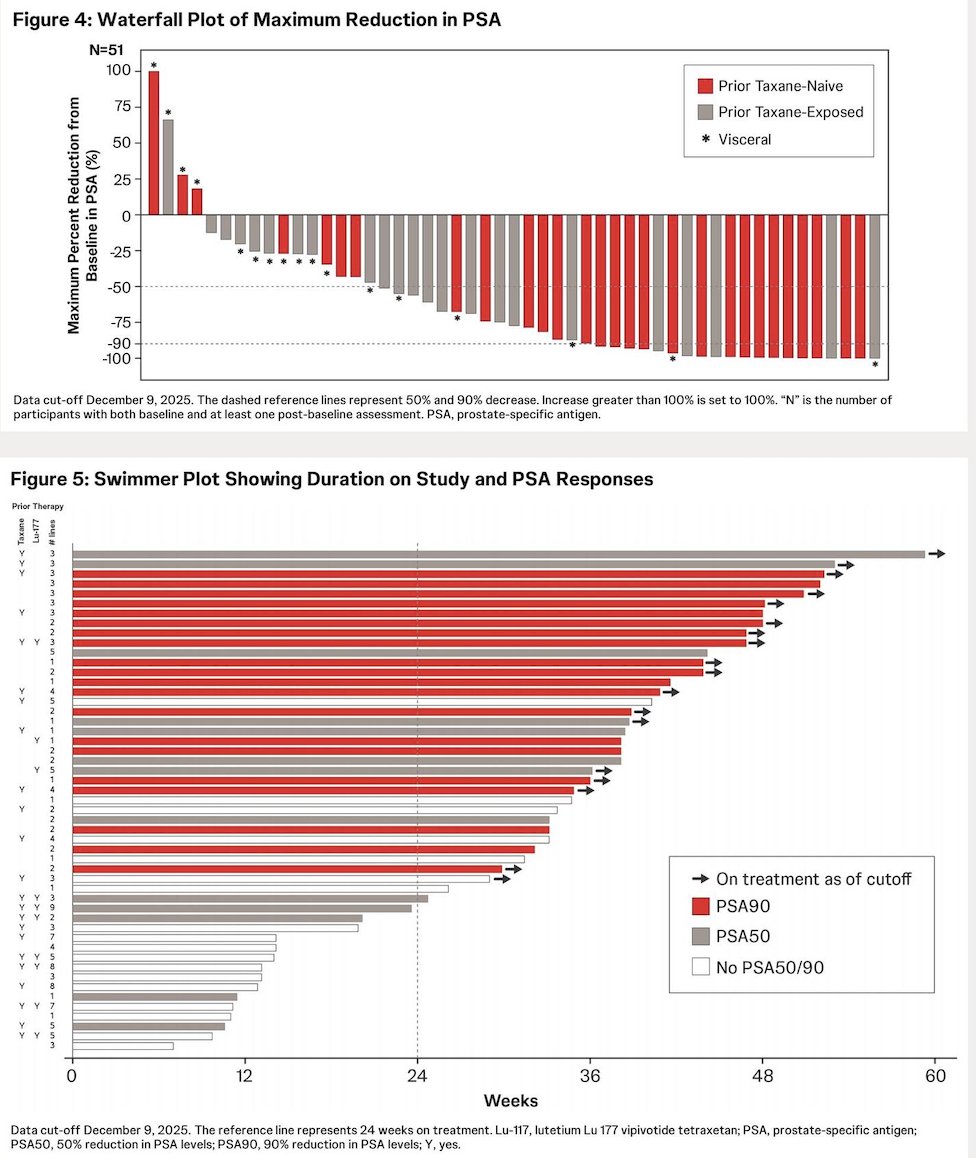
Dr. Patel concluded his presentation with the following key takeaways:
- Pasritamig was readily combinable with full-dose docetaxel without dose-limiting toxicities.
- The safety profile was consistent with docetaxel alone, and notably, no cytokine release syndrome was observed.
- Encouraging PSA responses were observed, particularly among taxane-naïve patients.
- A Phase 3 trial, KLK2-PASenger, evaluating PAS + Docetaxel is now enrolling (NCT07225946).
- Additional combinations with PAS are being explored in Phase 1 trials
Presented by: Manish R. Patel, MD, Medical Oncologist/Hematologist, Director of Drug Development, Florida Cancer Specialists & Research Institute, Associate Director of Drug Development, Sarah Cannon Research Institute, Sarasota, FL
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Reference:- Farha NG, Kasi A. Docetaxel. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Updated June 8, 2024. https://www.ncbi.nlm.nih.gov/books/NBK537242/.2