(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session A: Prostate Cancer. Dr. Neal D. Shore presented Poster 189: Are long-term remissions possible with hormonal therapy only? Post hoc analysis of EMBARK examining sustained PSA <0.2 ng/mL despite testosterone recovery after treatment suspension.
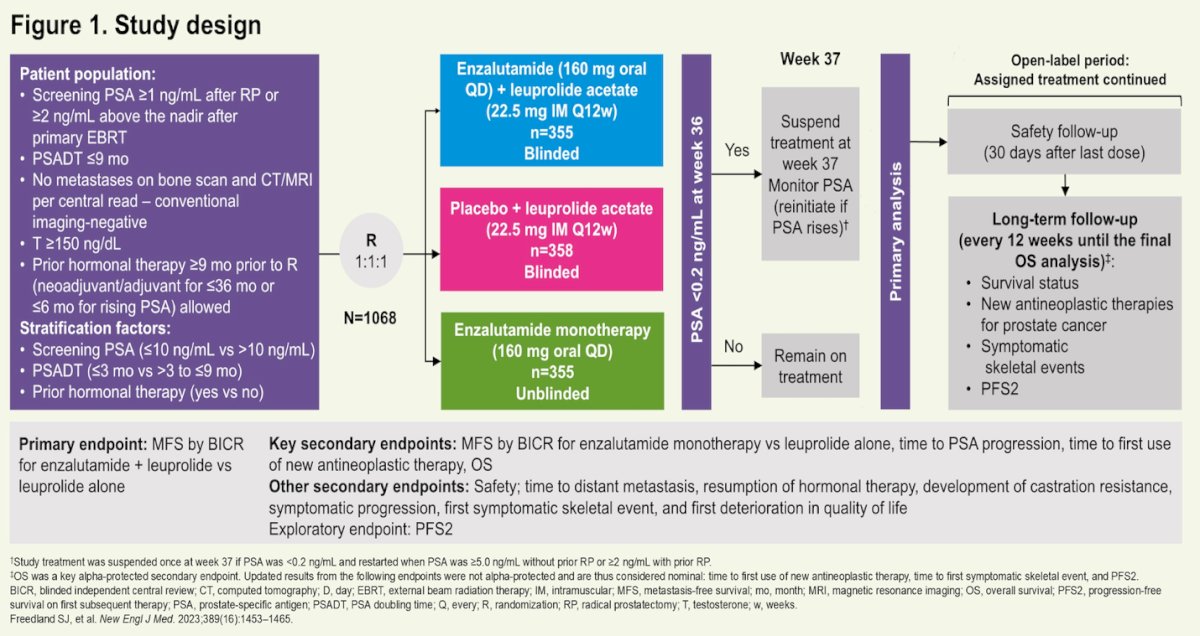
Dr. Shore emphasized that EMBARK previously demonstrated significant improvements in metastasis-free survival with enzalutamide plus leuprolide (enza combo) and enzalutamide monotherapy (enza mono), as well as an overall survival benefit with the combination in patients with high-risk biochemical recurrence.1 A distinctive feature of EMBARK was treatment suspension after 36 to 37 weeks in patients who achieved PSA <0.2 ng/mL. This analysis explored the durability of PSA suppression following treatment discontinuation, particularly in the setting of testosterone recovery.
In EMBARK (NCT02319837), patients were randomized 1:1:1 to enza combo, leuprolide alone (LA), or enza mono. After 36 weeks of therapy, treatment was suspended in patients with PSA <0.2 ng/mL. This post hoc analysis evaluated the proportion of patients maintaining PSA <0.2 ng/mL at 12, 24, and 36 months following suspension, and assessed testosterone recovery to baseline, >175 ng/dL, and >250 ng/dL. The study design is presented below.
At 36 months after treatment suspension, 9.3% of patients in the enza combo group maintained PSA <0.2 ng/mL, compared with 3.4% in the LA group and 2.3% in the enza mono group. Rates were higher at earlier timepoints and gradually declined over time, but remained consistently greatest in the combination arm.
The proportions of patients maintaining deep PSA suppression with testosterone recovery varied across treatment groups. At 36 months after treatment suspension, 3.7% of patients in the enzalutamide combination group, 1.4% in the leuprolide-alone group, and 1.1% in the enzalutamide monotherapy group had maintained PSA levels <0.2 ng/mL and achieved testosterone recovery to 250 ng/dL.
At the same 36-month timepoint, 3.7% of patients treated with the enzalutamide combination, 0.8% of those receiving leuprolide alone, and 0.6% of those receiving enzalutamide monotherapy-maintained PSA <0.2 ng/mL without achieving testosterone recovery to 175 ng/dL.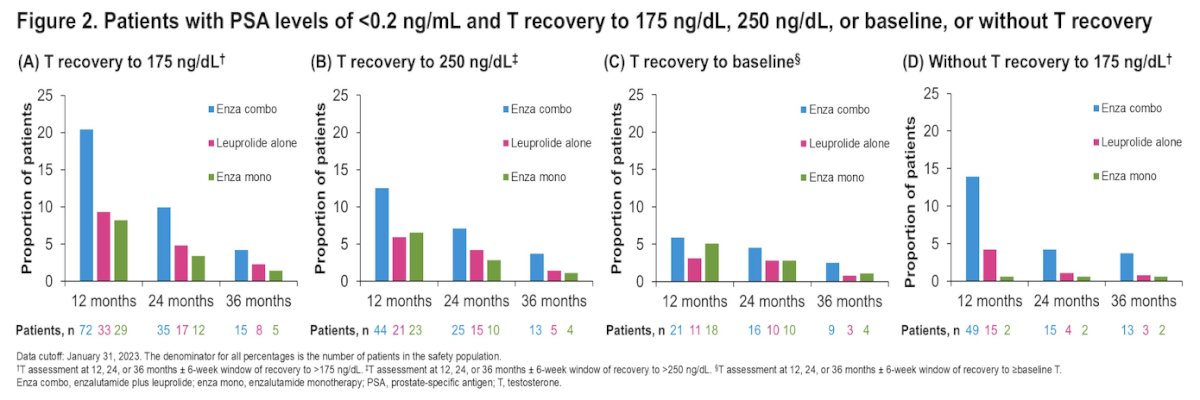
Moreover, at 36 months after treatment suspension, 2.0%, 1.4%, and 0.3% of patients in the enzalutamide combination, leuprolide-alone, and enzalutamide monotherapy groups, respectively, maintained PSA levels <0.02 ng/mL and achieved testosterone recovery to 250 ng/dL. Additionally, 1.1%, 0.6%, and 0.3%, respectively, maintained PSA levels <0.02 ng/mL but did not achieve testosterone recovery to 175 ng/dL, as illustrated in the accompanying figure.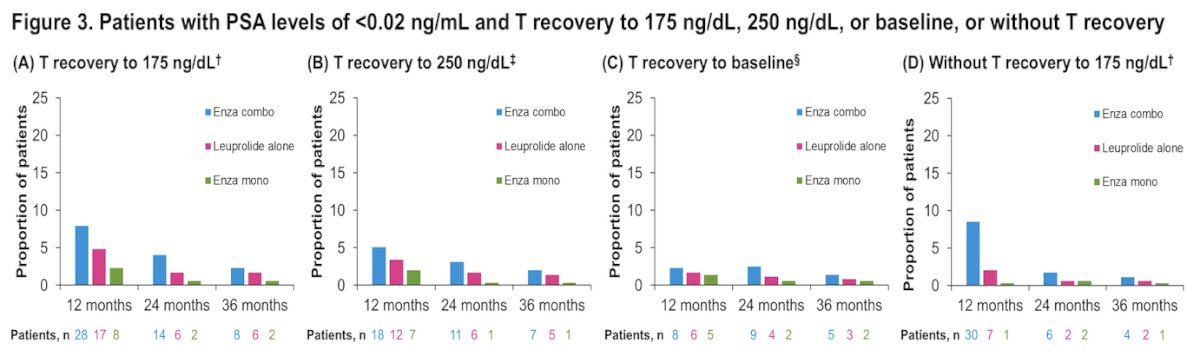
These findings suggest that a subset of patients experience sustained biochemical control despite normalization of testosterone, raising the possibility of treatment-free intervals with preserved disease control. Moreover, this analysis adds an important dimension to the EMBARK results by demonstrating that prolonged biochemical remissions are possible even after testosterone normalization.
Taken together, Dr. Shore concluded that this data support several key observations:
- Approximately 1 in 25 patients treated with enzalutamide plus leuprolide for 9 months maintained PSA <0.2 ng/mL with normalized testosterone levels (>250 ng/dL) three years after treatment suspension, supporting the possibility of durable treatment-free remissions after finite combination therapy.
- Corresponding rates in the leuprolide-alone and enzalutamide monotherapy groups were substantially lower, at approximately 1% in each arm compared with ~4% in the enzalutamide combination arm.
- Notably, about 2% of patients treated with the enzalutamide combination achieved even deeper biochemical responses, maintaining PSA levels below the lower limit of quantification (<0.02 ng/mL) with normal testosterone recovery at three years.
Presented by: Neal D. Shore, MD, FACS, Director, START Carolinas/Carolina Urologic Research Center, Head of GU Oncology and Radiopharm START Research, AUC Urology Specialists, Myrtle Beach, SC
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Reference: