(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a prostate cancer poster session. Dr. Neal Shore presented real-world results from the Prostate Cancer Disease Observation (PRECISION) data platform evaluating the outcomes of 177Lu-PSMA-617 after sipuleucel-T in metastatic castration-resistant prostate cancer (mCRPC) patients.
Clinical trials have demonstrated the effectiveness of 177Lu-PSMA-617 in patients with mCRPC who have previously received androgen receptor pathway inhibitors (ARPIs) with or without taxane-based chemotherapy.1,2 In the phase III VISION trial, patients with prostate-specific membrane antigen (PSMA)-positive mCRPC previously treated with ARPIs and taxane-based chemotherapy who received 177Lu-PSMA-617 plus best standard of care had significantly prolonged radiographic progression-free survival (rPFS) of 8.7 months, a median overall survival (OS) of 15.3 months, and a 46% reduction in the risk of progression or death compared with standard of care alone.1 In the 177Lu-PSMA-617 arm of the PSMAfore trial, taxane-naïve patients with PSMA-positive mCRPC who had progressed on prior ARPI therapy demonstrated a median rPFS of 11.6 months and a median OS of 24.5 months,3 with notable PSA response rates including PSA50 responses exceeding 50%.2
Sipuleucel-T is an immunotherapy indicated for patients with asymptomatic or minimally symptomatic mCRPC and has been associated with improved survival benefit, particularly among patients with lower baseline PSA levels.4,5 However, data evaluating the effectiveness of 177Lu-PSMA-617 following prior sipuleucel-T therapy remain limited, which is particularly important given the prevalent use of sipuleucel-T in community urology settings.4 This real-world study was therefore performed to assess the effectiveness of 177Lu-PSMA-617 in patients previously treated with sipuleucel-T.
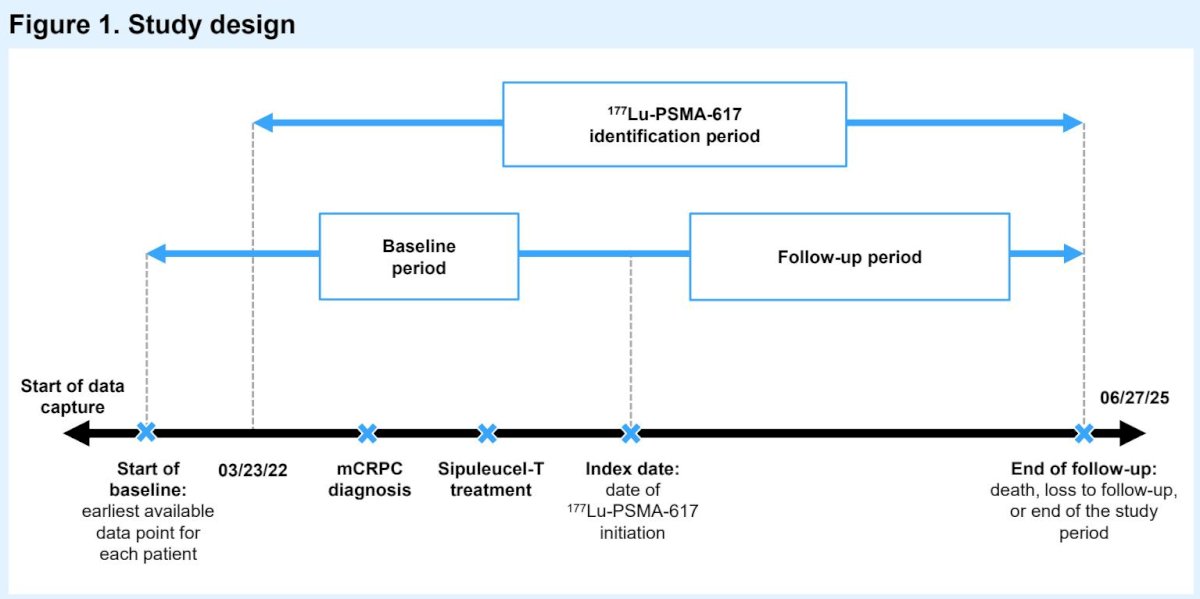
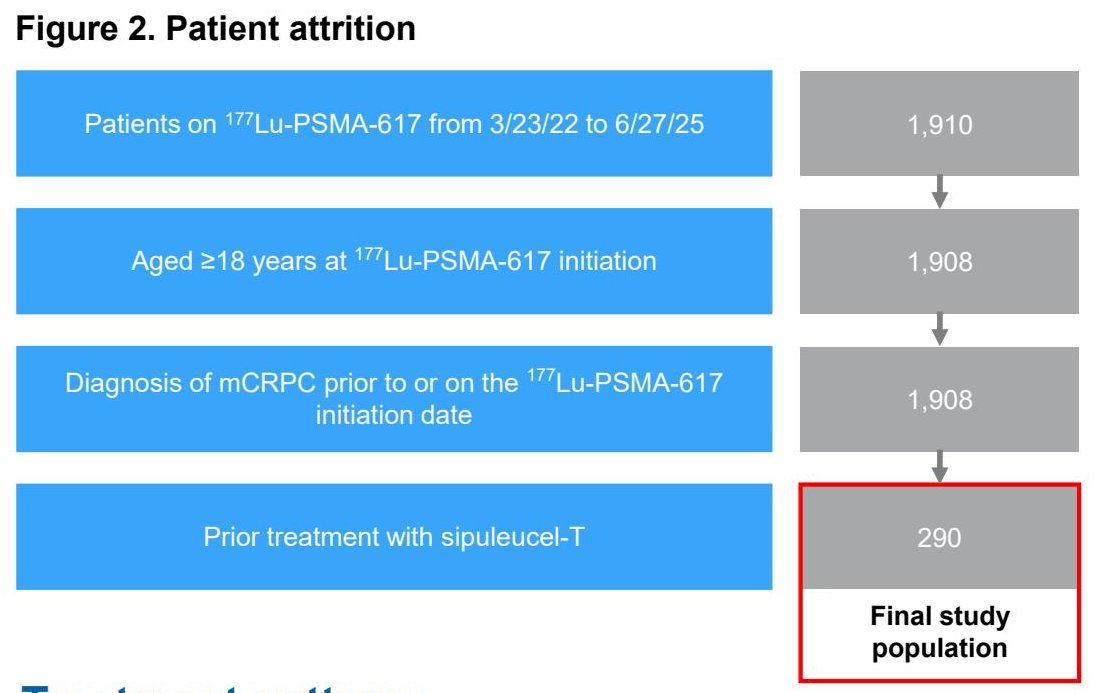
This was a retrospective, observational study using data extracted from the Prostate Cancer dISease observatiON (PRECISION) data platform, a harmonized dataset integrating electronic health records and claims data from community, academic, urology, and medical oncology settings.5 Adult patients with clinically documented mCRPC who had received ≥1 dose of 177Lu-PSMA-617 between March 23, 2022, and June 27, 2025, and who had a history of sipuleucel-T treatment were included. The index date was defined as the date of 177Lu-PSMA-617 initiation.
Patient characteristics and treatment patterns were evaluated descriptively. PSA outcomes included PSA declines ≥50% (PSA50) and ≥90% (PSA90) comparing baseline PSA (within 120 days prior to 177Lu-PSMA-617 initiation) with the lowest PSA value between 28 days after treatment initiation and the last day of therapy. Progression-free survival (PFS) and overall survival (OS) were analyzed using Kaplan-Meier methodology.
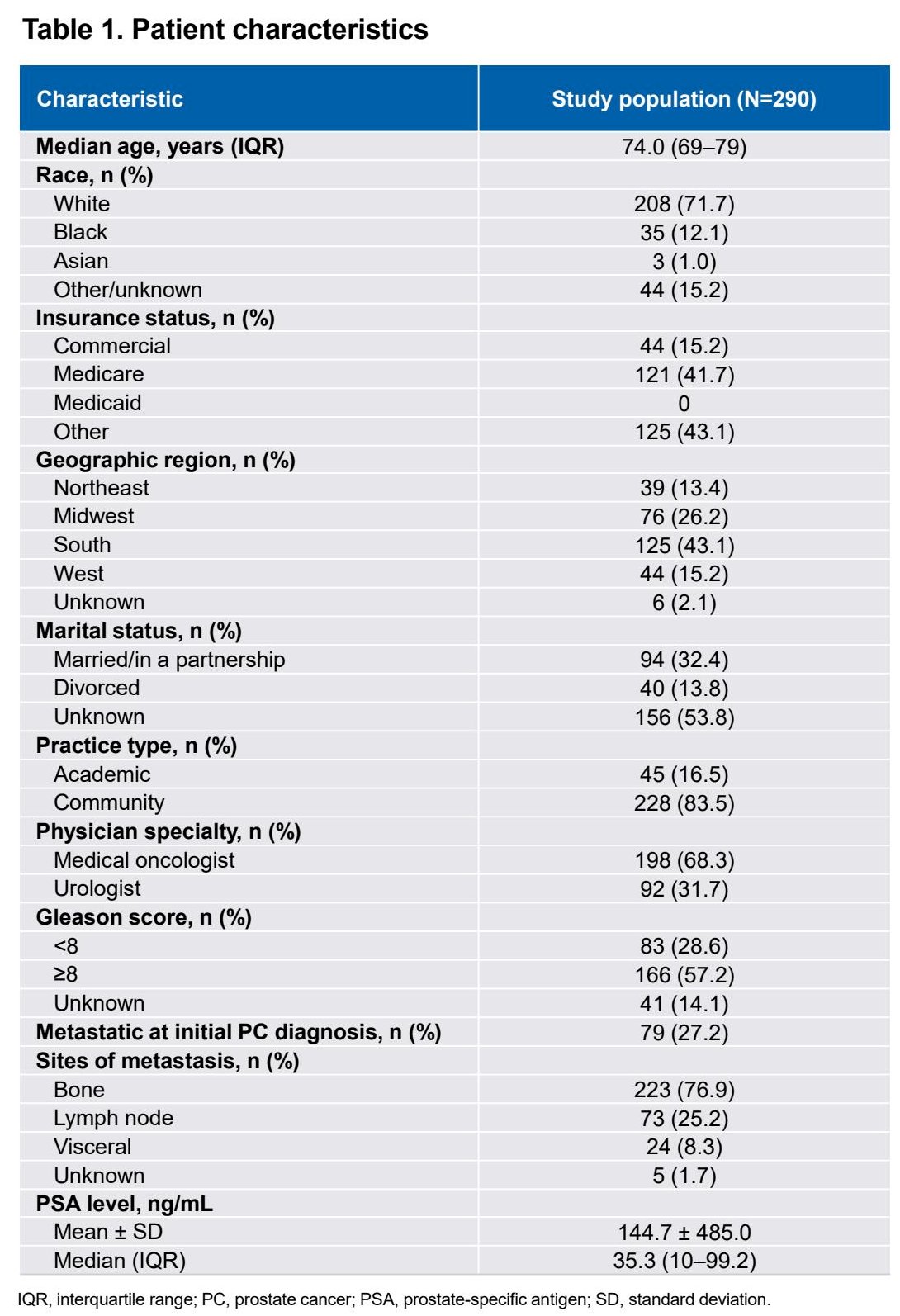
A total of 290 patients were included in the final study population. The median age was 74 years (IQR: 69–79). At index, 32% of patients were in urology and 68% in oncology settings.
The cohort was predominantly White (71.7%), with 12.1% Black patients and smaller proportions of Asian and other racial groups. The median baseline PSA was 35.3 ng/mL (IQR 10.0–99.2), and 57% of patients had Gleason score ≥8 disease. At initial prostate cancer diagnosis, 76.9% had bone metastases, 25.2% lymph node metastases, 8.3% visceral metastases, and 1.7% unknown metastatic status.
Treatment patterns reflected a heavily pretreated population. Prior to 177Lu-PSMA-617 initiation, 77% of patients had received at least one ARPI and 79% had received at least one taxane chemotherapy, with 89% initiating 177Lu-PSMA-617 in the fourth line of therapy or later in the mCRPC setting. The median time from prostate cancer diagnosis to 177Lu-PSMA-617 initiation was 7.4 years, and from mCRPC diagnosis to treatment initiation was 3.1 years. The median interval between sipuleucel-T treatment and 177Lu-PSMA-617 initiation was 2.8 years (IQR 1.5–5.0). The median duration of 177Lu-PSMA-617 therapy was 148 days (IQR 50–211 days), with a median number of treatment cycles of five (IQR 2–6).
During therapy, 14% of patients received at least one other guideline-recommended therapy for mCRPC, and among patients receiving concomitant treatment, 65% received an ARPI, 13% a PARP inhibitor, and the remainder other systemic therapies.
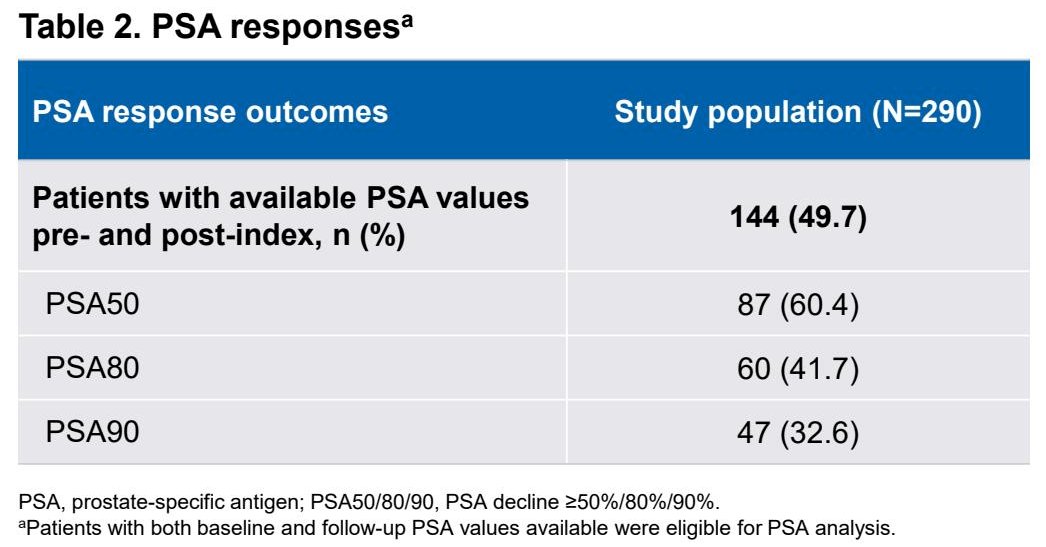
Among the 144 patients with evaluable PSA values both before and after treatment initiation, 60.4% achieved PSA50 responses, 41.7% achieved PSA80 responses, and 32.6% achieved PSA90 responses. These PSA response rates are consistent with prior prospective data evaluating PSMA-targeted radioligand therapy in later-line mCRPC populations.
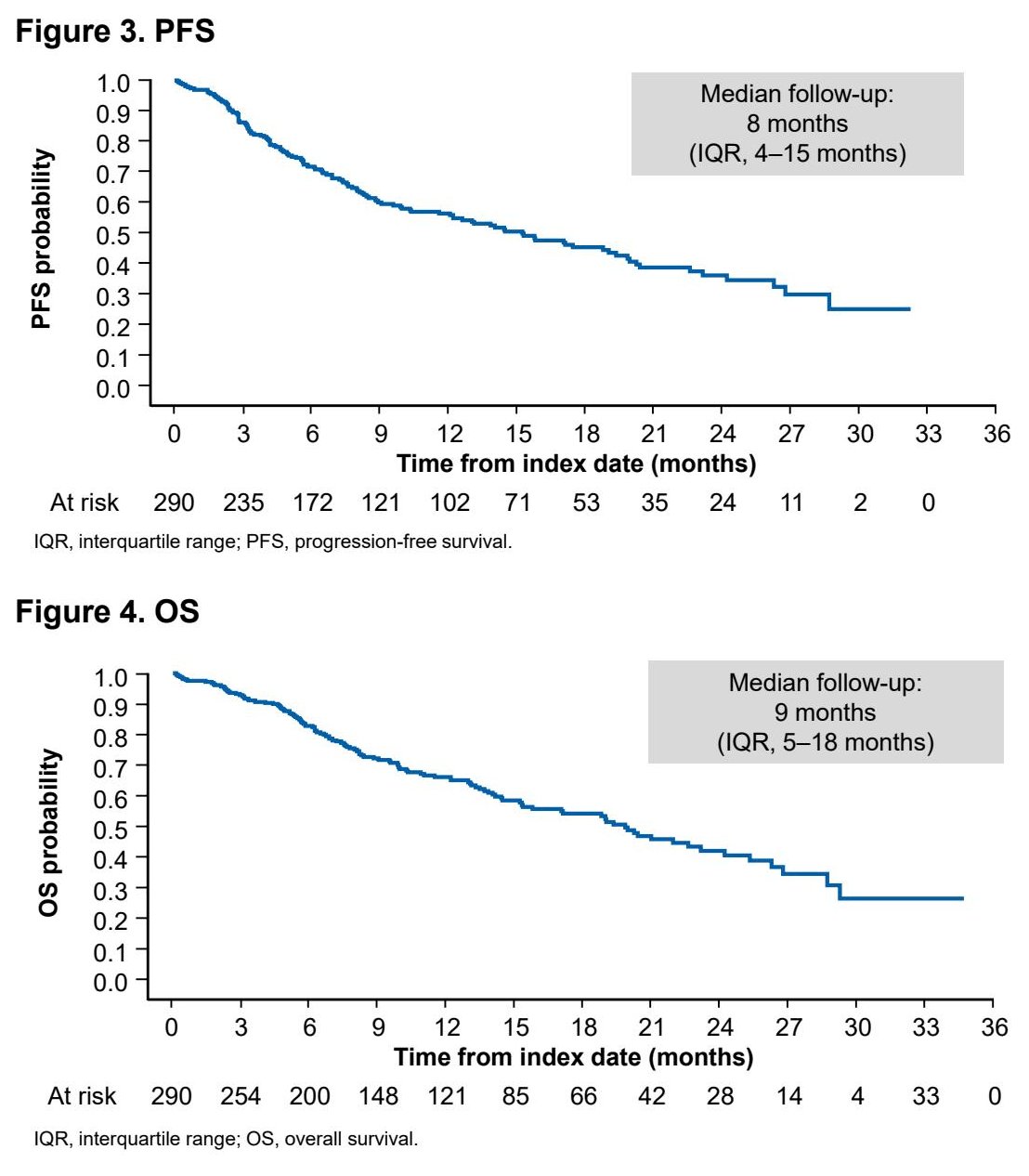
With a median follow-up of approximately 8 months (IQR 4–15 months), median progression-free survival was 15.2 months (95% CI 11.6–19.4 months). Median overall survival was 19.8 months (95% CI 15.3–23.2 months), consistent with previously reported outcomes for 177Lu-PSMA-617 in advanced mCRPC cohorts.
Study limitations included restriction of PSA response analyses to patients with available baseline and follow-up PSA data, limiting generalizability to the entire cohort. Additionally, reasons for treatment decision-making were not available within the PRECISION platform, and this was a relatively small cohort requiring further validation in larger datasets.
Dr. Shore concluded as follows:
- In this real-world analysis, the effectiveness of ¹⁷⁷Lu-PSMA-617 in patients previously treated with sipuleucel-T was broadly similar to that observed in patients in the Phase 3 VISION and PSMAfore clinical trials
- In addition to sipuleucel-T, the majority of patients had a history of ≥1 ARPI and/or ≥1 taxane treatment
- The median PFS was 15.2 months, the median OS was 19.8 months, and high percentages of patients experienced deep PSA responses
- Overall, these results suggest that patients receiving ¹⁷⁷Lu-PSMA-617 after sipuleucel-T have a relatively slow disease course, with a median time from mCRPC onset of >3 years, but still responded well to ¹⁷⁷Lu-PSMA-617
Presented by: Neal D. Shore, MD, FACS, Medical Director, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
References:
- Sartor O, de Bono J, Chi KN, et al. Lutetium-177-PSMA-617 for metastatic castration-resistant prostate cancer. N Engl J Med. 2021;385:1091-1103.
- Morris MJ, De Bono JS, Chi KN, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024;404:1227-1239.
- Fizazi K, Morris MJ, Chi KN, et al. Final overall survival and safety analyses of the phase III PSMAfore trial of [177Lu]Lu-PSMA-617 versus change of androgen receptor pathway inhibitor in taxane-naïve patients with metastatic castration-resistant prostate cancer. Ann Oncol. 2025;36:1319-1330.
- Caram MEV, Ross R, Lin P, et al. Factors associated with use of sipuleucel-T to treat patients with advanced prostate cancer. JAMA Netw Open. 2019;2:e192589.
- Heath E, George DJ, Shore ND, et al. Real-world treatment patterns and outcomes in advanced prostate cancer: a cohort study using the PRECISION (PRostate Cancer dISease observatiON) data platform. Presented at: ASCO Genitourinary Cancers Symposium; February 13-15, 2025; San Francisco, CA. Poster presentation.