(UroToday.com) The 2026 ASCO GU Annual Symposium hosted a prostate cancer poster session. Dr. Takuma Kato presented the results of a Japanese multicenter, retrospective study evaluating the outcomes of Radium-223 + enzalutamide for metastatic castration-resistant prostate cancer (mCRPC).
The PEACE-3 trial previously demonstrated improved survival outcomes with the combination of enzalutamide and radium-223 in patients with mCRPC.1 However, the incremental benefit of adding enzalutamide to radium-223, as opposed to radium-223 to enzalutamide (as in PEACE-3), in routine clinical practice remains incompletely characterized. The study investigators, therefore, conducted a nationwide multicenter retrospective study in Japan to evaluate the real-world effectiveness and safety of radium-223 plus enzalutamide compared with radium-223 monotherapy.
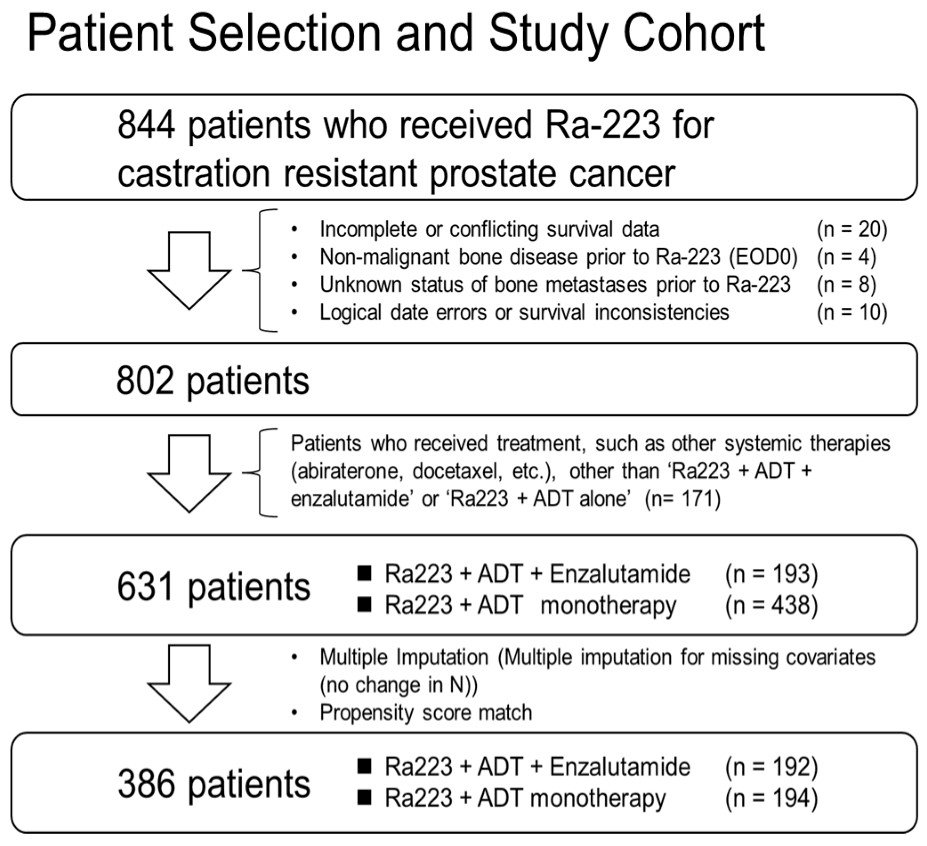
Patients with mCRPC treated with radium-223 between January 2020 and December 2023 across 84 institutions in Japan were retrospectively identified. Patients were categorized according to treatment received: radium-223 plus enzalutamide versus radium-223 monotherapy. To reduce baseline imbalances, propensity score matching was performed. Continuous variables were compared using the Mann–Whitney U test or Student’s t-test, categorical variables using the chi-square test, and overall survival outcomes were estimated using Kaplan–Meier methodology with log-rank comparisons.
Among 844 patients treated with radium-223, 802 met eligibility criteria. After propensity score matching, 386 patients were included in the final analysis: 192 treated with radium-223 plus enzalutamide and 194 treated with radium-223 alone.
Baseline characteristics were generally well-balanced between groups. Most patients in both cohorts had ECOG performance status 0–1, comparable extent of bone metastatic disease by EOD classification, similar hematologic and biochemical laboratory parameters, and similar rates of bone-modifying agent use (approximately three-quarters of patients in each cohort).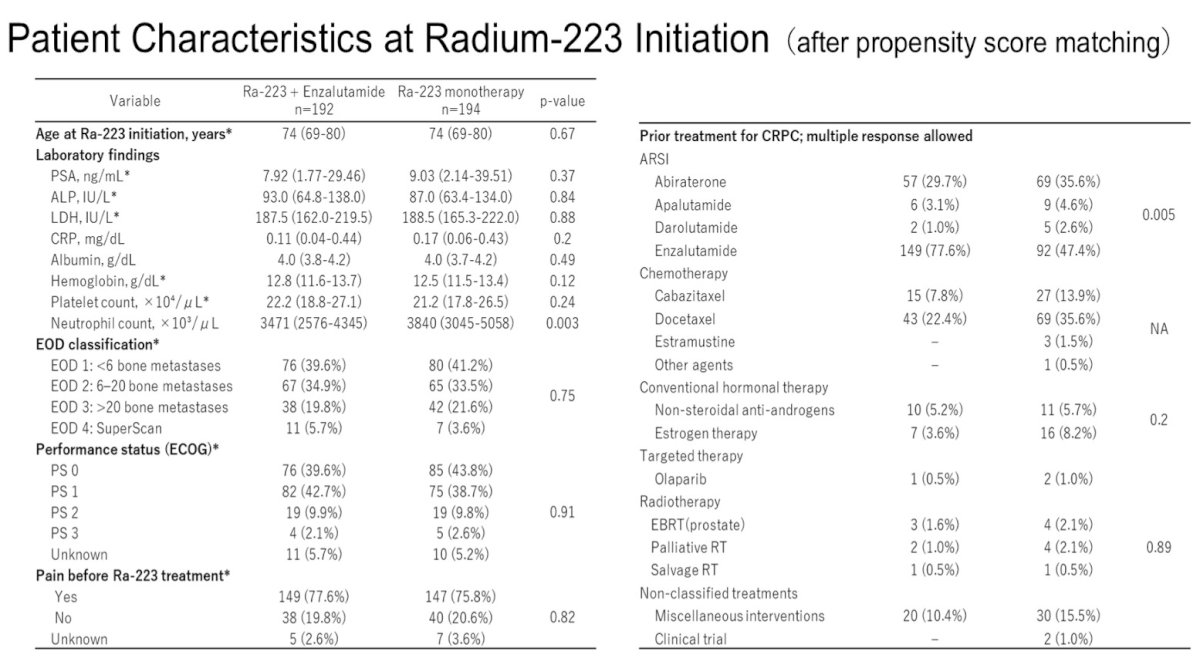
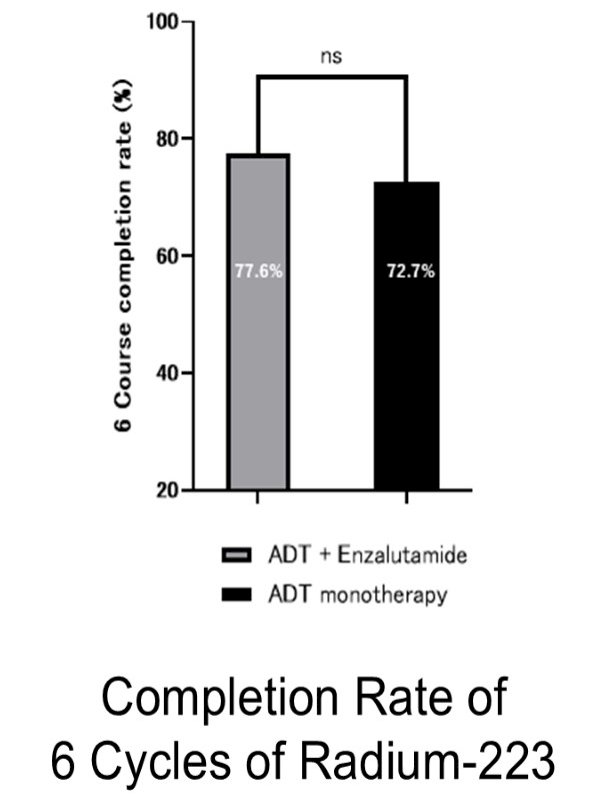
Radium-223 was administered across multiple lines of therapy, most commonly in the first- and second-line mCRPC settings. Treatment completion rates were similar between cohorts, with comparable proportions of patients completing the planned six-cycle course, indicating that concomitant enzalutamide did not appear to adversely affect treatment feasibility.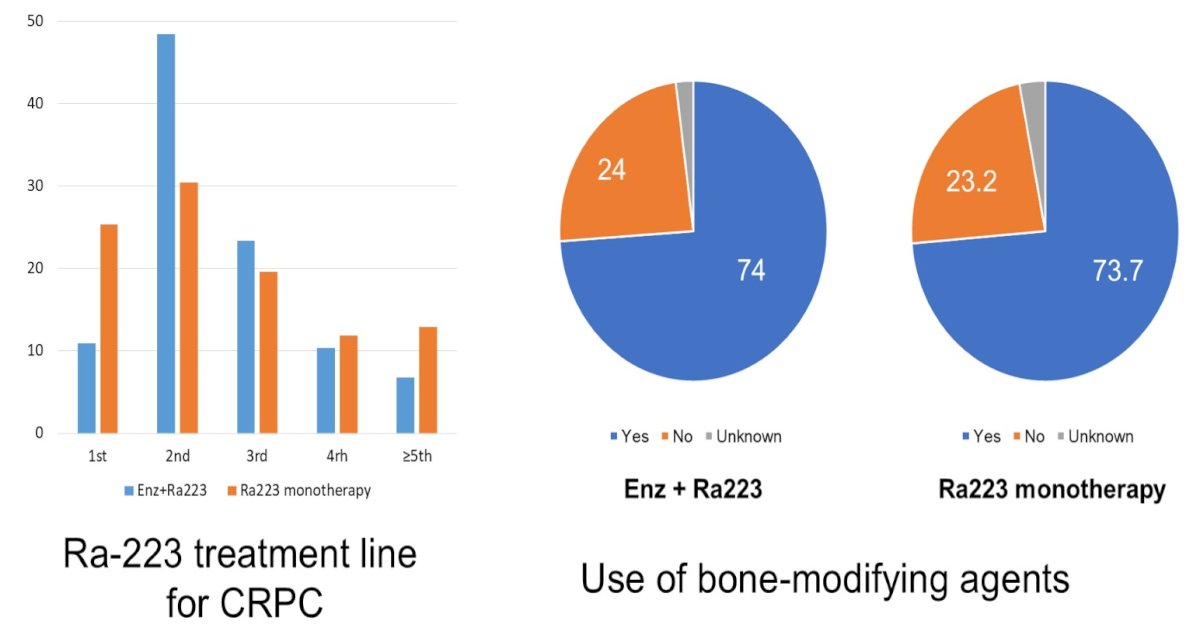
Progression outcomes modestly favored the combination cohort. At data cutoff, disease progression was reported in 78% of patients treated with radium-223 plus enzalutamide compared with 81% among those receiving radium-223 monotherapy. The median time to progression from radium-223 initiation was significantly longer in the combination cohort (6 months vs 5 months, p=0.01).
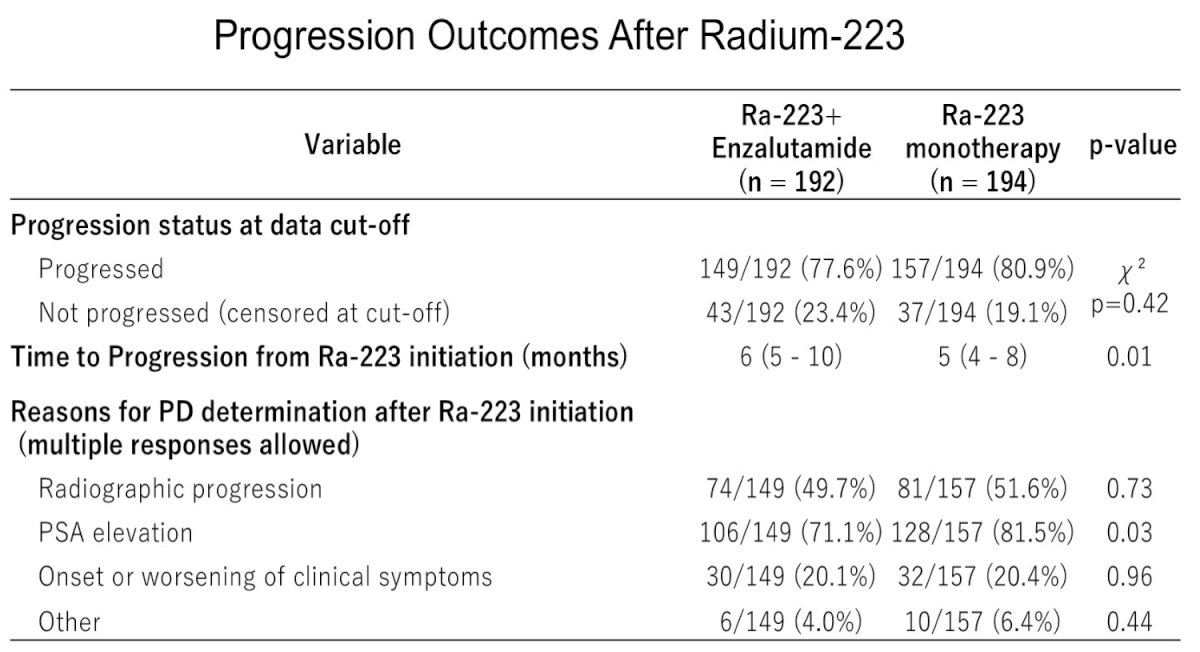
Patterns of progression were broadly similar between groups. Radiographic progression was the most common driver (~49% in the combination cohort vs ~52% with monotherapy). PSA progression appeared more frequent in the monotherapy group (approximately 81.5% vs 71.1%), whereas clinical symptomatic progression was relatively infrequent in both groups (~19–20%).
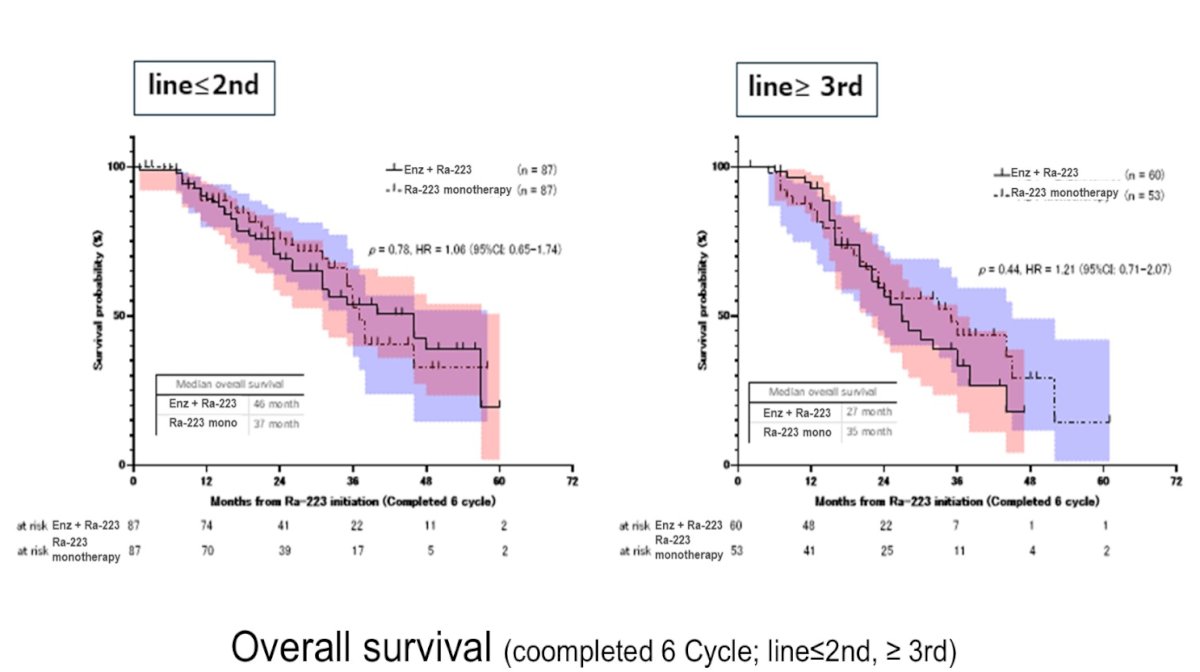
Overall survival analyses among patients completing six cycles of radium-223 demonstrated no statistically significant differences between cohorts, including analyses stratified by treatment line (second line or later). These findings suggest that while the addition of enzalutamide may modestly improve progression-related outcomes, a clear overall survival advantage was not observed in this real-world dataset.
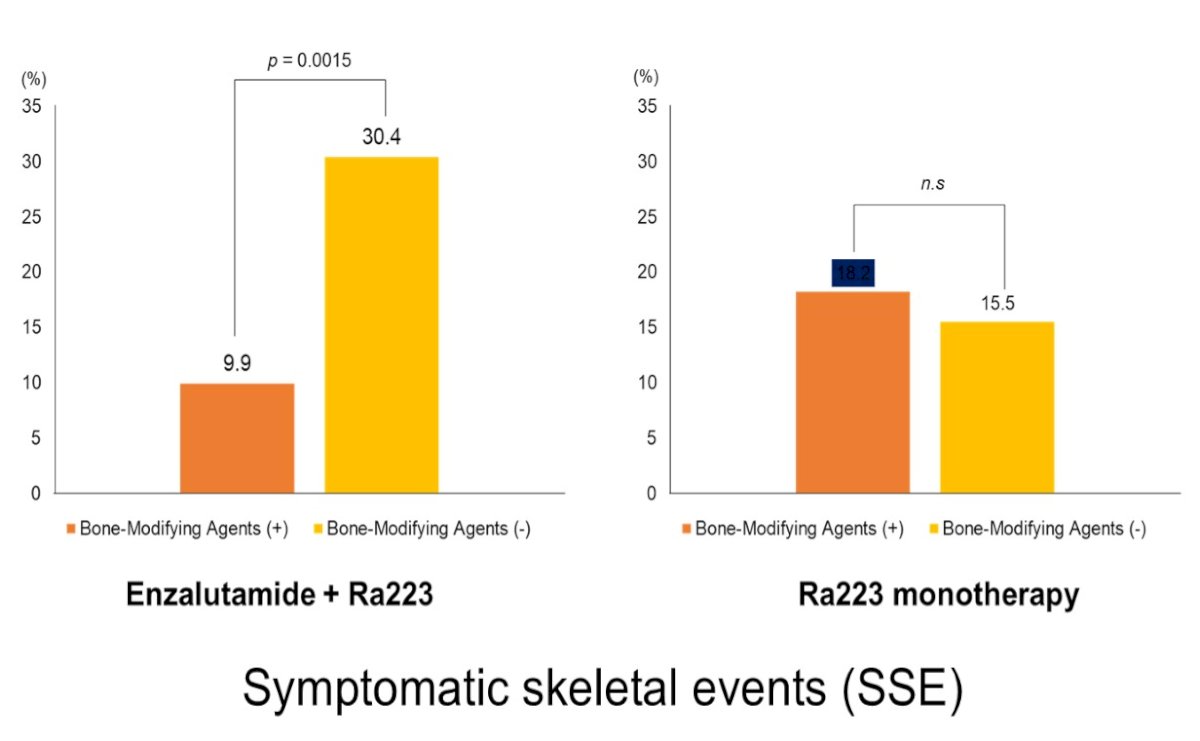
Safety profiles were generally comparable between cohorts. Hematologic toxicities and non-hematologic adverse events were similar between groups, with no major safety signals observed with the combination approach. Symptomatic skeletal events (SSEs) remained clinically relevant. Consistent with prior experience with radium-223, use of bone-modifying agents was associated with reduced SSE risk, and approximately three-quarters of patients in both cohorts received concomitant skeletal protection.
Overall, this Japanese nationwide retrospective analysis suggests that combining enzalutamide with radium-223 in patients with mCRPC may modestly prolong time to progression without compromising treatment tolerability, although overall survival outcomes appear comparable to radium-223 monotherapy. These findings support the feasibility of combination therapy in appropriately selected patients while reinforcing the continued importance of bone-modifying agents to mitigate skeletal complications.
Presented by: Takuma Kato, MD, PhD, Assistant Professor, Department of Urology, Faculty of Medicine, Kagawa University Hospital, Miki, Kagawa, Japan
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 ASCO GU Annual Symposium, San Francisco, CA, February 26th-28th, 2026
Reference: