(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer trials in progress session and a presentation by Dr. Fernando de Moura discussing COACTION, a randomized trial of neoadjuvant leuprorelin, darolutamide, or both prior to radical prostatectomy for intermediate or high risk prostate cancer. While radical prostatectomy results in excellent survival in patients with low- and favorable intermediate risk localized prostate cancer, the role of surgery in the setting of higher risk disease remains controversial. Many unfavorable intermediate, high, and very high risk patients are treated with ADT in combination with radiation. Although surgery can be curative for these patients, a subset will experience recurrence and have an increased risk of prostate cancer mortality. These recurrences result from either residual local disease and/or undiagnosed micrometastatic disease. Neoadjuvant therapy may improve local disease control by downstaging the primary tumor, treat occult distant metastasis, facilitate surgical resection, reduce or delay the need for post-surgery treatment, and provide an in vivo assessment of response to treatment.
COACTION is a prospective, randomized, open-label, with blinded endpoint adjudication multicenter clinical trial to assess whether a neoadjuvant combined treatment with leuprorelin and darolutamide is superior to monotherapy in terms of complete or almost complete pathological response. Key inclusion criteria include:
- Age ≥ 18 years
- Unfavorable intermediate or high/very high risk non metastatic prostate adenocarcinoma intended for surgery
- ECOG performance status ≤ 1
- Testosterone > 230 ng/dL
- No prior prostate cancer treatment
There will be 144 patients randomized 1:1:1 to three arms: darolutamide 600 mg PO BID for 24 weeks + leuprorelin 22.5 mg SC in 0 and 12 weeks versus darolutamide 600 mg PO BID alone for 24 weeks versus leuprorelin 22.5 mg SC 0 and 12 weeks alone:
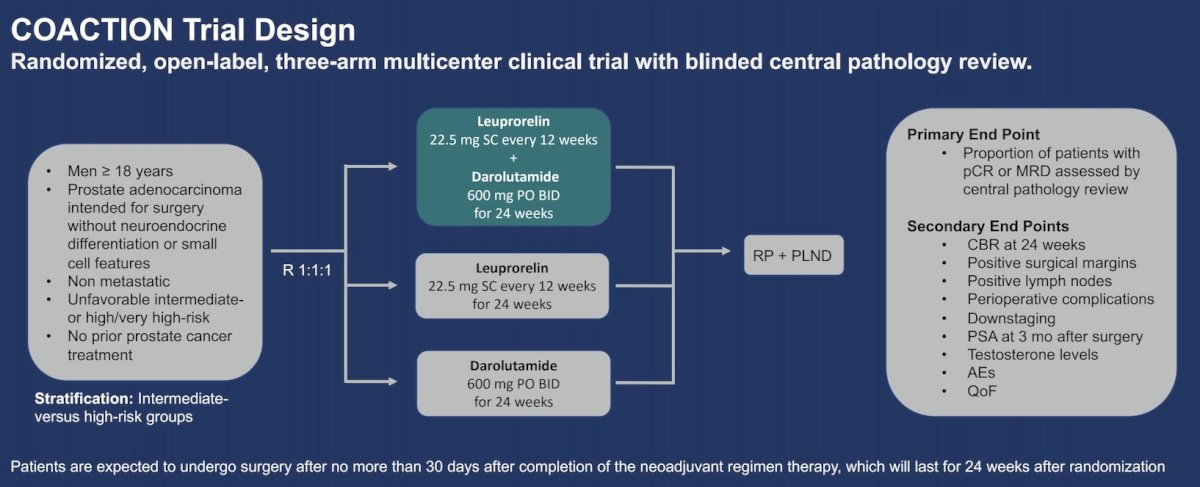
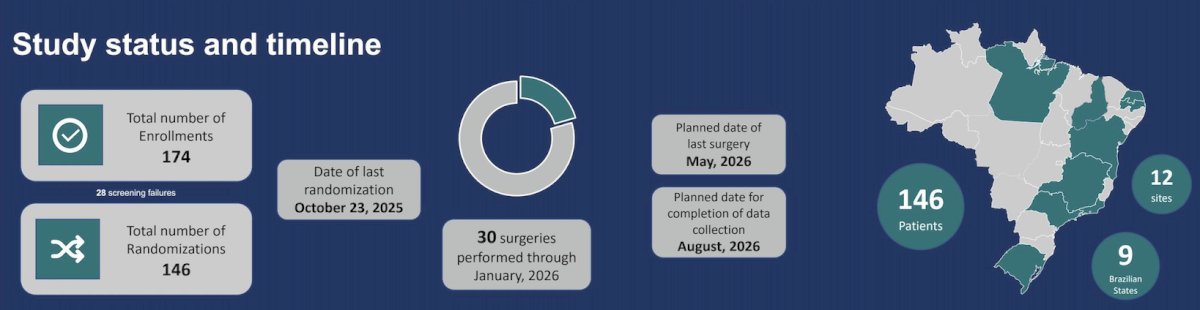
The primary endpoint is the proportion of patients with minimal residual disease, defined as residual cancer burden ≤ 0.25 cm3 or complete pathological response. The study's main analysis will compare the combination therapy group versus the pooled monotherapy groups. If null hypothesis is rejected, then the combination therapy group will be compared with either monotherapy group individually. Groups will be compared for the primary endpoint by a model from the binomial family and the log link function will be used to generate risk ratios and 95% CIs. Models will be adjusted for the stratification variable (intermediate versus high risk groups), for age, and race (white versus non-white). Dr. de Moura anticipates that the proportion of patients with minimal residual disease will be 10% in the pooled monotherapy groups and 30% in the combination therapy groups. For an alpha error of 5% and 80% power, the study will need a total of 132 patients included in the analytical population (44 in each group). In order to compensate for losses and patients who do not undergo surgery, they decided to enroll a total of ~144 patients. If all enrolled patients are included in the main analysis, the study will have 84% power to detect such a difference. The study timeline is highlighted as follows, noting that the planned date of the last surgery is May 2025 and the planned date for completion of data collection is August 2026:
Presented by: Fernando de Moura, Hospital Beneficencia Portuguesa, Sao Paulo, Brazil
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.