(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Fred Saad discussing ARANOTE post hoc analyses assessing efficacy and safety of darolutamide and androgen deprivation therapy (ADT) in patient subgroups by baseline comorbidities and concomitant medications. Darolutamide + ADT significantly improved radiological progression-free survival versus placebo + ADT (HR 0.54, 95% CI 0.41–0.71; p < 0.0001) in patients with metastatic hormone-sensitive prostate cancer (mHSPC) in the phase 3 ARANOTE trial, with a favorable safety profile.1
Darolutamide is also associated with low blood-brain barrier penetration and limited drug-drug interactions. Additionally, patients with prostate cancer, particularly older adult males, often have multiple comorbidities and are associated with polypharmacy (>= 5 medications), resulting in a substantial burden for this population. At ASCO GU 2026, Dr. Saad and colleagues reported outcomes in patients treated with darolutamide or placebo by comorbidities and use of concomitant medications at baseline.
Patients were randomized 2:1 to darolutamide 600 mg orally twice daily or placebo, both with ADT: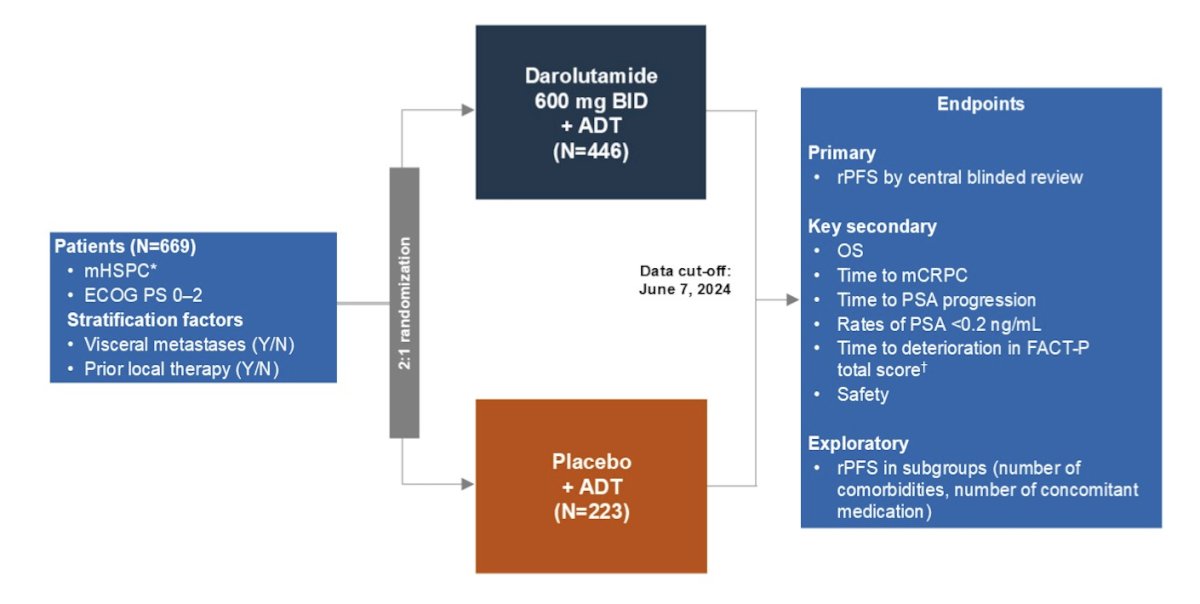
Patients were grouped by the median number and type of comorbidities or concomitant medications reported at baseline. A post hoc analysis was conducted for radiological progression-free survival, and hazard ratios were estimated using a Cox regression model. Descriptive statistics summarized baseline demographics, disease characteristics, and treatment-emergent adverse events by treatment group.
Baseline demographics and disease characteristics were generally similar between darolutamide (n = 446) and placebo (n = 223) across all subgroups, defined as a median of <5 or >=5 comorbidities or concomitant medications: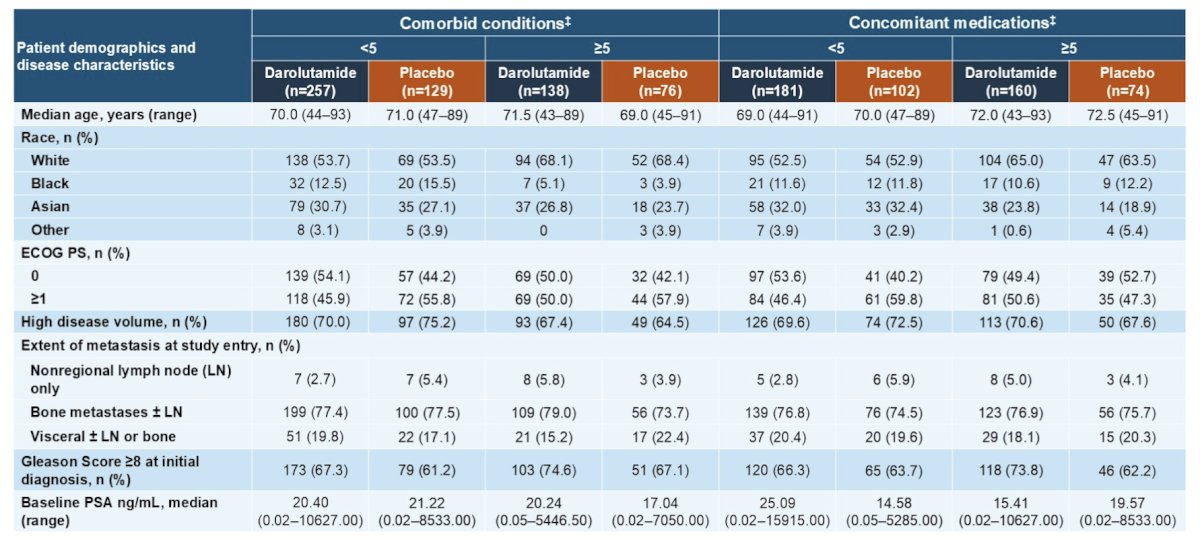
A radiological progression free survival benefit for darolutamide versus placebo was seen across all comorbidities (<5, HR 0.46, 95% CI 0.32–0.65; >=5, HR 0.58, 95% CI 0.36–0.93) and concomitant medications (<5, HR 0.48, 95% CI 0.32–0.72; >=5, HR 0.61, 95% CI 0.38–0.97) subgroups:
When analyzing specific comorbidities reported at baseline that are commonly associated with mHSPC and older age, darolutamide showed a consistent radiological progression free survival benefit compared with placebo, including in patients with/without metabolic (n = 185/415), cardiovascular (n = 372/228), renal or urinary (n = 237/363), gastrointestinal (n = 113/487), and musculoskeletal (n=190/410) disorders (HR range: 0.35–0.62):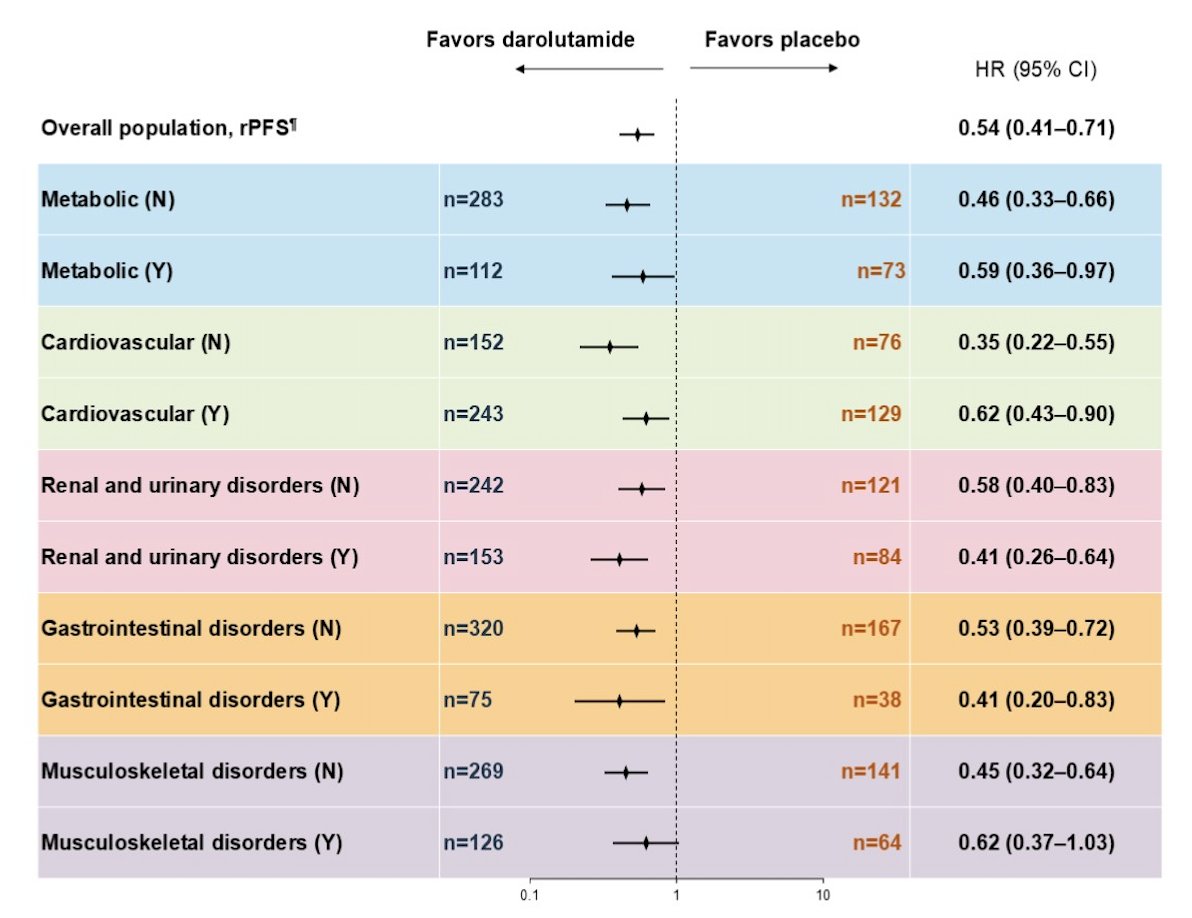
With darolutamide, the radiological progression-free survival benefit was similar in patients with cardiovascular disorders with or without corresponding concomitant medications (HR 1.07, 95% CI 0.58–1.94) and in patients with metabolic disorders with or without corresponding concomitant medications (HR 0.83, 95% CI 0.42–1.64):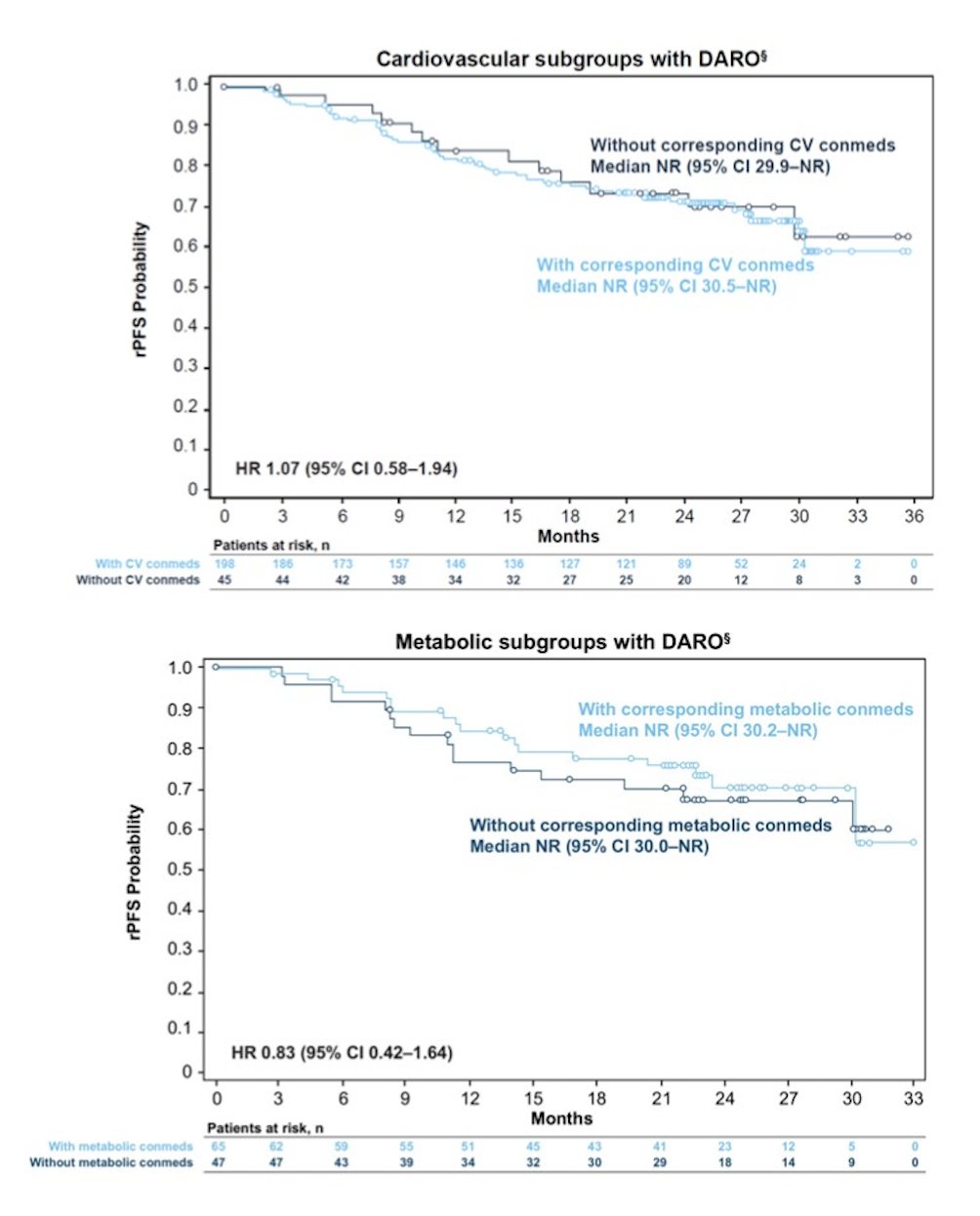
Treatment emergent adverse events, including those commonly associated with androgen receptor inhibitors and ADT, were generally similar between darolutamide versus placebo across comorbidities (grade 3–5; <5, 34.1% versus 32.8%; >=5, 38.4% versus 43.4%), and concomitant medications subgroups (grade 3–5; <5, 33.5% versus 34.7%; >=5, 39.4% versus 48.6%):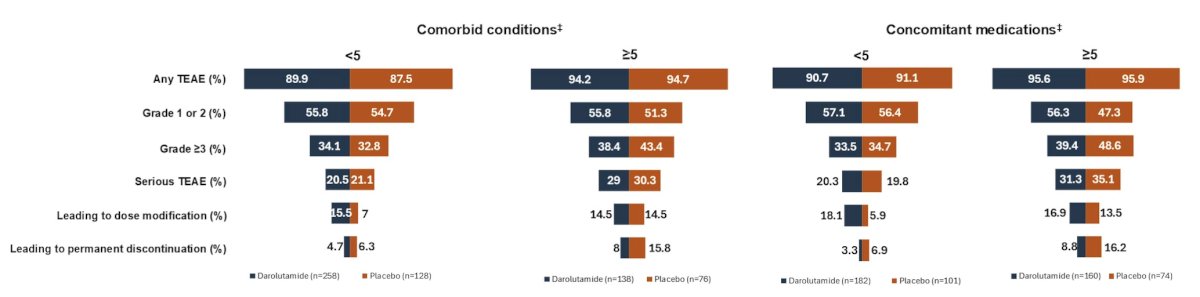
Discontinuations due to treatment-emergent adverse events in the darolutamide group were lower versus placebo for all patients in both the comorbidities (<5; 4.7% versus 6.3%; >=5, 8.0% versus 15.8%) and concomitant medications (<5; 3.3% versus 6.9%; >=5, 8.8% versus 16.2%) subgroups.
Dr. Saad concluded his presentation discussing ARANOTE post hoc analyses assessing efficacy and safety of darolutamide and ADT in patient subgroups by baseline comorbidities and concomitant medications with the following take-home points:
- The radiographic progression-free survival benefit of darolutamide was observed across all subgroups, regardless of the number of comorbidities and concomitant medications reported at baseline
- Darolutamide was well tolerated across all subgroups, with no new safety signals, supporting the use of darolutamide in mHSPC, even in patients with multiple comorbidities and greater use of concomitant medication
Presented by: Fred Saad, CQ, MD, FRCS, FCAHS, Professor, Department of Surgery, Raymond Garneau Chair in Prostate Cancer, Director of Prostate Cancer Research, Director of GU Oncology, Université de Montréal, University of Montreal Hospital Centers, CRCHUM, Montréal, QC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.