(UroToday.com) The 2026 GU ASCO annual meeting featured a testicular cancer session and a presentation by Dr. Jennifer King discussing a phase II trial of cabozantinib in relapsed refractory germ cell tumors. Overall, 20% of patients with metastatic germ cell tumors relapse after front-line therapy, and up to 50% relapse after salvage chemotherapy. Thus, there remains a need for new therapeutic options for those not cured with salvage therapies. Vascular endothelial growth factor expression, increased angiogenesis, and activation of the c-MET pathway have biological importance in germ cell tumors. Cabozantinib is a multi-targeted oral tyrosine-kinase inhibitor targeting c-MET, VEGF, RET, and AXL. At ASCO GU 2026, Dr. King and colleagues reported results from a phase II trial of cabozantinib in refractory germ cell tumors.
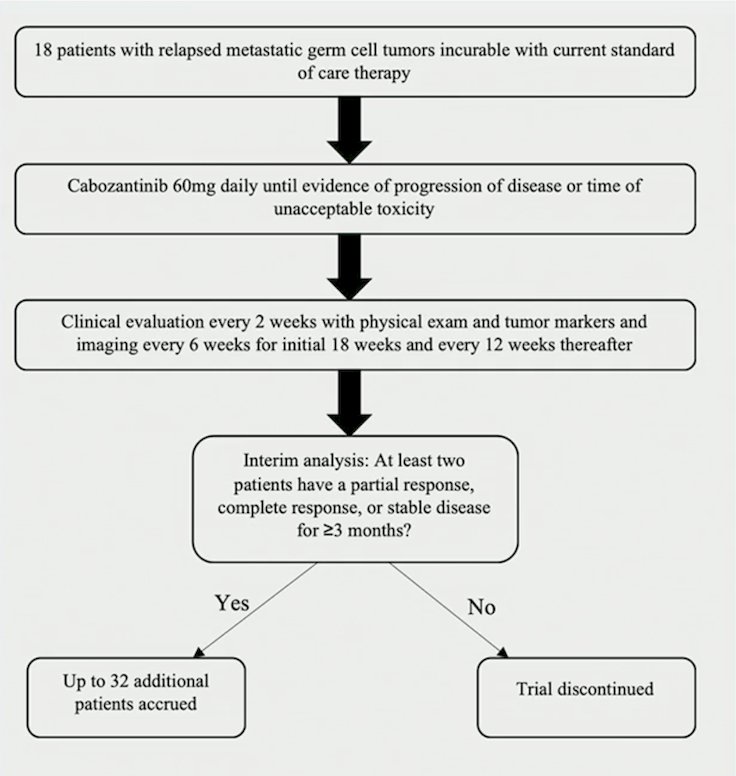
This single arm phase II trial used a Simon two-stage design investigating cabozantinib 60 mg in patients with incurable relapsed/refractory germ cell tumors. Patients aged≥18 years with progressive metastatic germ cell tumors after first line cisplatin-based chemotherapy and at least 1 salvage regimen were eligible. The primary endpoint was clinical benefit rate, defined as the proportion of complete response, partial response, and stable disease for ≥3 months using RECIST 1.1, modified to include AFP and hCG. Simon’s 2-stage required clinical benefit in ≥ 2/18 patients to proceed to stage 2, and then enrolled up to 50 patients:
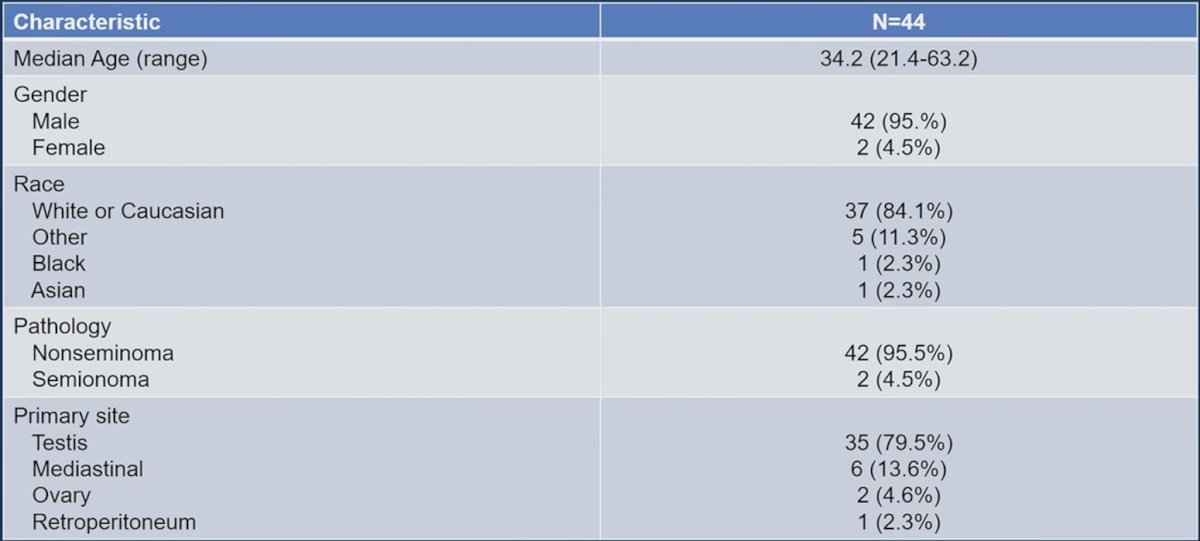
Simon stage I was met and expanded to stage 2; there were 44 patients evaluable, including two females. The median age was 34.2 years (range: 21.4-63.2), and 42 patients (95.5%) had nonseminomatous germ cell tumors. The primary sites included the testis for 79.5%, mediastinal 13.6%, ovary 4.6%, and retroperitoneal 2.3%. IGCCCG risk at initial diagnosis was good for 22.7%, intermediate 25%, poor 47.8%, and unknown 4.5%. There were 18 patients (40.9%) who had late relapse disease. The median number of prior chemotherapy regimens was 4, and 63.6% of patients previously received high-dose chemotherapy with peripheral blood stem-cell transplant. The median AFP was 210.3 (range: 1.1-120,693), and hCG was 0.95 (range: 0.6-72,759):

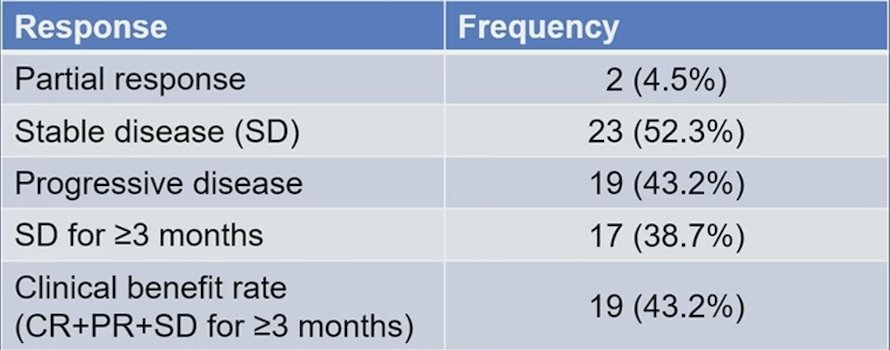
The clinical benefit rate was 43.2%, with 2 patients (4.5%) achieving a partial response and 17 (38.6%) achieving stable disease for ≥3 months. No complete responses were seen:
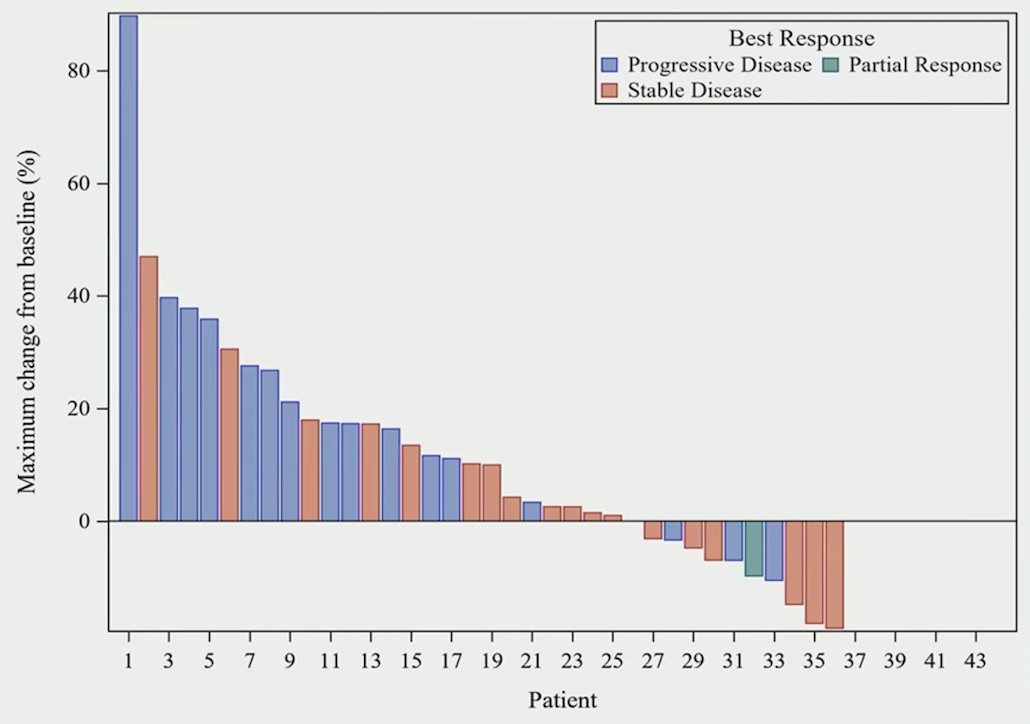
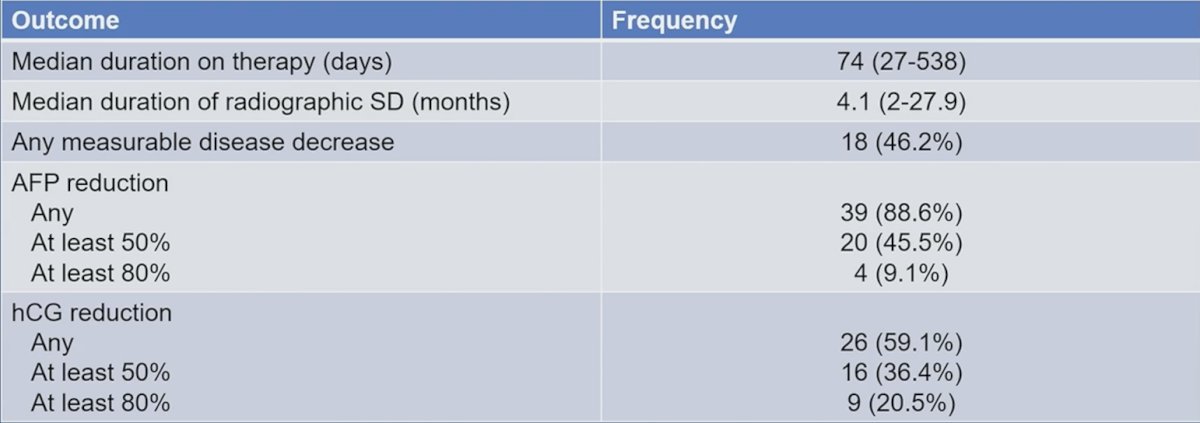
The median progression free survival was 2.4 months, and the median overall survival was 7.3 months. The median duration of treatment was 74 days (range: 27-848). For those with stable disease as best response, the median duration of stable disease was 3.7 months (range: 2.0-18.5). Stable radiographic disease was seen in 50% of patients, with a median duration of 4.1 months (range: 2.01-27.9). Any measurable disease decrease was seen in 18 patients (46.2%). Overall, 95.5% of patients had AFP or hCG reduction, with 65.9% achieving at least 50% AFP or hCG reduction and 27.3% achieving at least 80% AFP or hCG reduction:
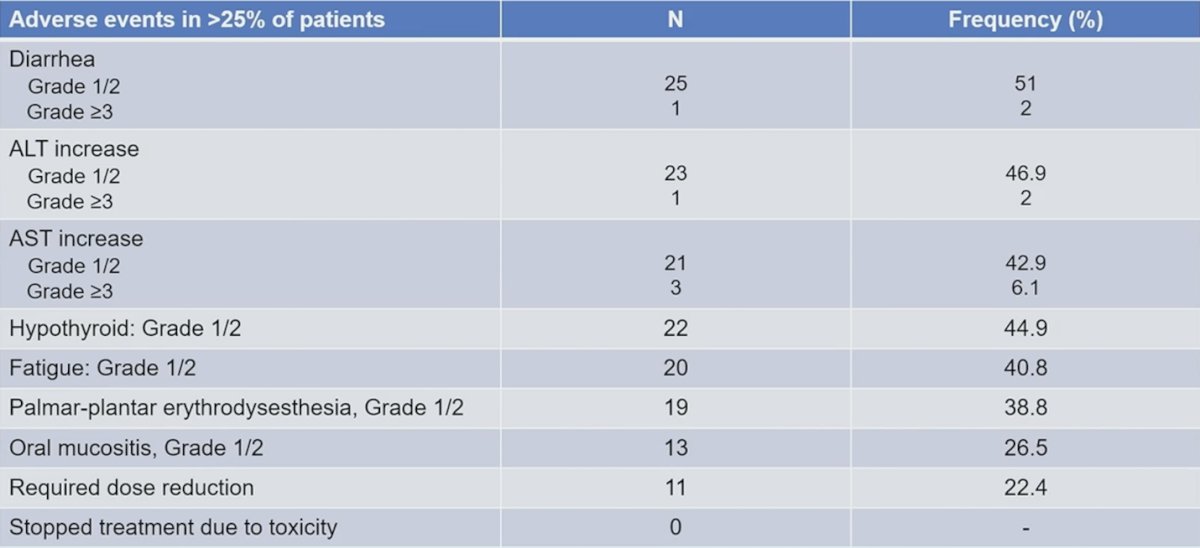
The most common adverse event was diarrhea, occurring in 59.1% of patients, with 96.2% being grade 1/grade 2. The most common grade ≥3 adverse event was increased AST, occurring in 6.8% of patients. There were 11 patients requiring a dose reduction, and two patients remain on treatment:
Dr. King concluded her presentation discussing a phase II trial of cabozantinib in relapsed refractory germ cell tumors with the following take-home points:
- Cabozantinib demonstrated a clinical benefit rate of 43.2% in a heavily pre-treated patient population with relapsed, refractory germ cell tumors
- The adverse event profile has little overlapping toxicities with cytotoxic chemotherapy typically used for germ cell tumors, thus allowing for less cumulative toxicity of platinum chemotherapy
- There is an ongoing study (n = 38) of zanzalintinib plus oral etoposide in a safety lead-in cohort of patients with relapsed, refractory germ cell tumors. Once safety has been demonstrated, the study transitions to single arm, phase II maintenance post-salvage high dose chemotherapy
Presented by: Jennifer King, MD, Indiana University Simon Comprehensive Cancer Center, Indianapolis, IN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.