(UroToday.com) The 2026 GU ASCO annual meeting featured a renal cell carcinoma session and a discussant presentation by Dr. Beckermann, discussing three abstracts, “Belzutifan + lenvatinib versus cabozantinib for advanced renal cell carcinoma (RCC) after anti-PD-(L)1 therapy: Open-label phase 3 LITESPARK-011 study” by Dr. Robert Motzer, “Adjuvant pembrolizumab + belzutifan versus pembrolizumab for clear cell RCC: The randomized phase 3 LITESPARK-022 study” by Dr. Toni Choueiri, and “Patient-reported outcomes in resected RCC: Active monitoring vs. durvalumab and tremelimumab in the RAMPART trial” by Dr. Sophie Merrick.
Dr. Merrick started her discussion with LITESPARK-022, noting that there are two important hypotheses regarding HIF-2alpha:
- Adjuvant HIF-2alpha targeting may shut down early truncal biology
- Targeting HIF creates synergy with PD-1
The following table highlights the positive adjuvant immunotherapy trials in RCC:

Of note, LITESPARK-022 had the same KEYNOTE-564 risk groups, but expanded the M1 NED inclusion to resection within 2 years, narrowing the allowed metastatic sites, and shifted stratification from geography and ECOG performance status to grade and risk type. In LITESPARK-022 over 28.3 months of follow-up, pembrolizumab + belzutifan significantly improved disease-free survival versus pembrolizumab + placebo (HR 0.72, 95% CI 0.59–0.87; p = 0.0003). The estimated 24-month disease-free survival rate was 80.7% versus 73.7%. In KEYNOTE-5641 over a 30.1-month follow-up, pembrolizumab significantly improved disease-free survival versus placebo (HR 0.63, 95% CI 0.50–0.80; p < 0.0001). The estimated 24-month disease-free survival rate was 78.3% versus 67.3%:
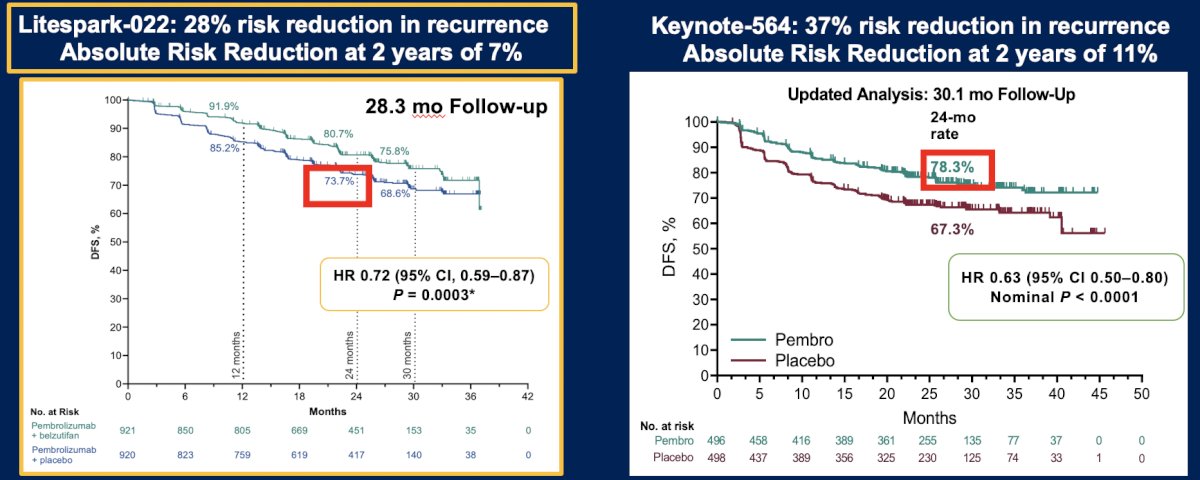
Dr. Beckermann notes that there was early and stable separation of the curves that persists after completion of 12 months of belzutifan, but will there be a tail of the curve in LITESPARK-022? Did differences in eligibility (M1 NED fraction, risk strata) result in different performance of pembrolizumab?
Importantly, LITESPARK-022 disease-free survival subgroups specific to risk category differ from the results seen in KEYNOTE-564:
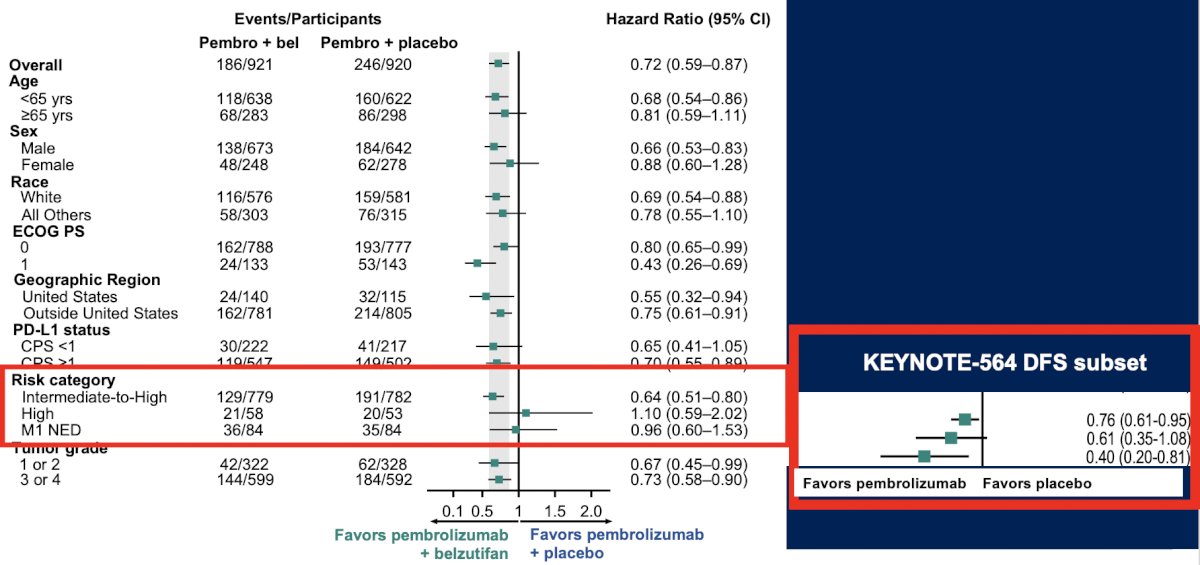
The subgroup differences may reflect biologic heterogeneity, but this remains hypothesis-generating, and we need biomarker enrichment.
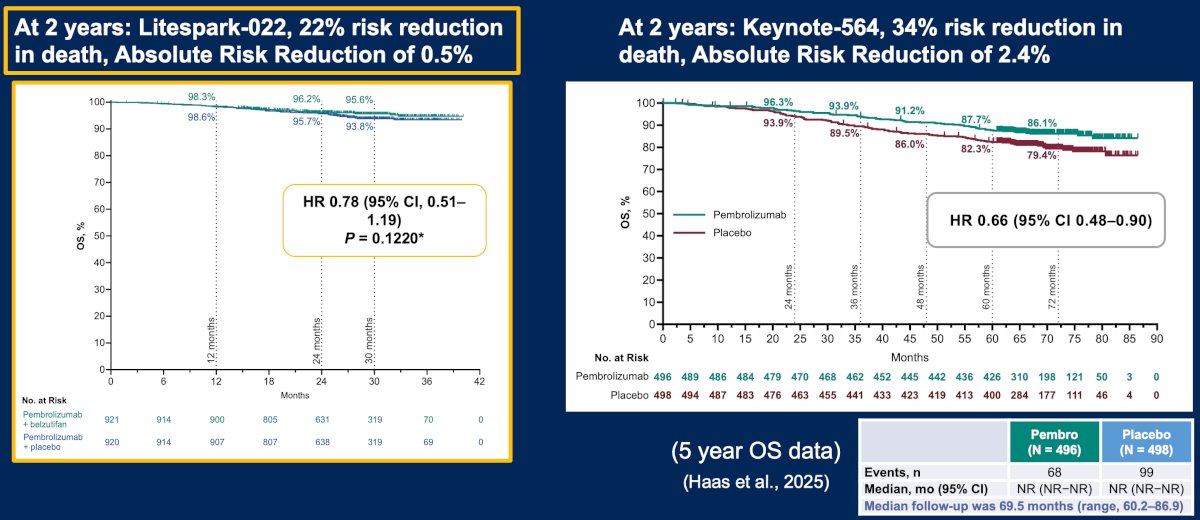
With regards to survival, will this follow the IO + IO (stable hazard ratio over time) and IO + TKI (worsening hazard ratio over time) as in the metastatic setting? At 2 years in LITESPARK, there was a 22% reduction in death (absolute risk reduction of 0.54%), compared to at 2 years in KEYNOTE-564, which showed a 34% risk reduction in death (absolute risk reduction of 2.4%):
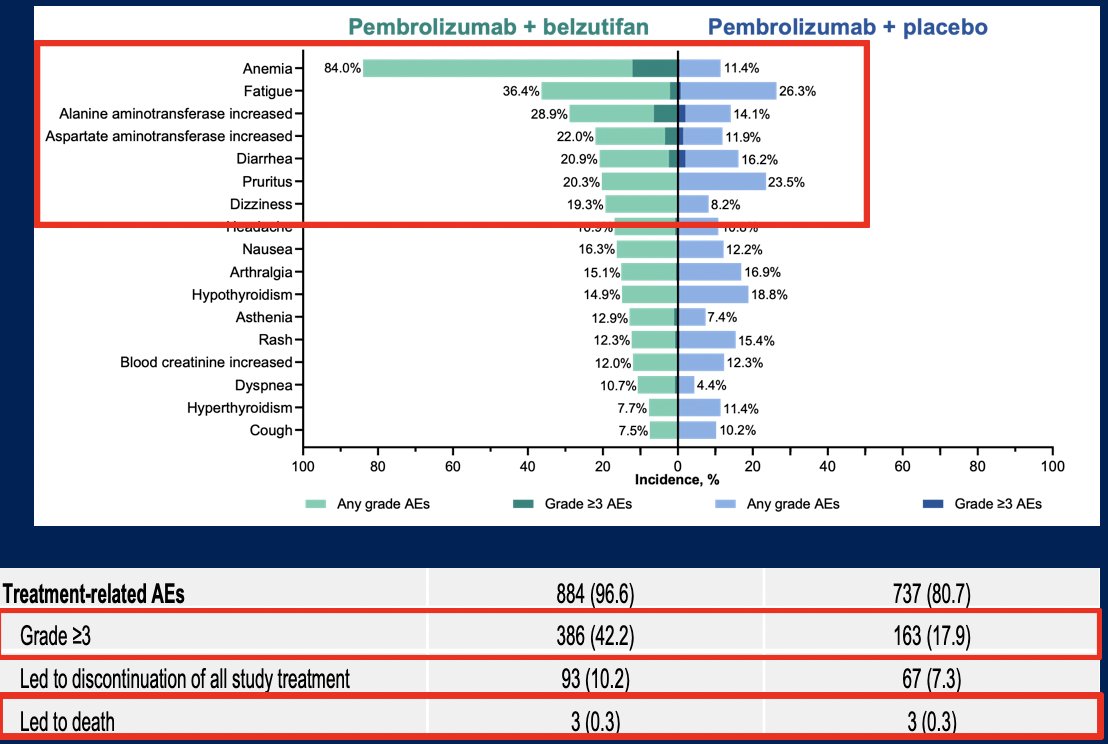
As with any adjuvant trial, there is a risk-benefit calculation between a disease-free survival improvement versus exposing patients with no evidence of disease to treatment harms. As expected, pembrolizumab + belzutifan had reversible side effects, with no worsening of immune related adverse events, However, anemia lead to (i) 25% of patients requiring a dose interruption, (ii) 17% of patients requiring a dose reduction, (iii) 4% of patients discontinuing belzutifan, and (iv) 12% of patients receiving blood or erythropoietin. Moreover, hypoxia resulted in 5% grade adverse events, 2.5% of patients needing a dose interruption, and 3.5% of patients needing a dose reduction:
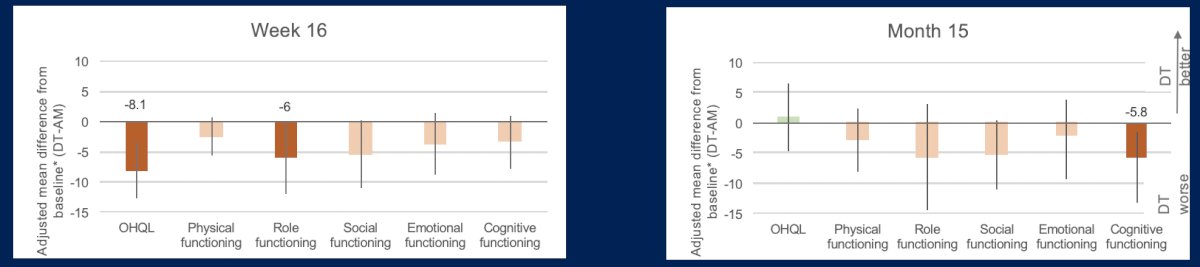
Dr. Beckermann then discussed the RAMPART the trial, which assessed efficacy and toxicity for adjuvant durvalumab and tremelimumab. Patient reported outcomes matter: when there is no tumor, every side effect counts. In RAMPART, outcomes assessed included overall health and quality of life (Q29–30) at week 16, five functional domains, eight symptom domains, and financial difficulties at both week 16 and month 15. This analysis found that at week 16, durvalumab + tremelimumab was associated with worse quality of life, with clinically meaningful declines in overall health related quality of life, role functioning, fatigue, and insomnia. These early effects appeared to improve by month 15
At month 15, durvalumab + tremelimumab was associated with new clinically meaningful declines in pain and cognitive function:
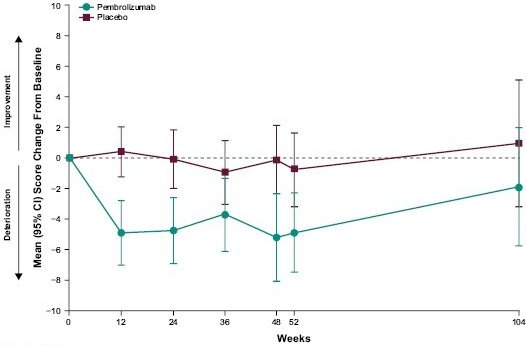
A similar pattern was seen in KEYNOTE-564 of a decline during treatment, though this was not clinically meaningful per trial definition:
Dr. Beckermann importantly notes that there is a real quality of life decline on treatment, including overall health quality of life, fatigue, and insomnia that mostly resolve after treatment but some may emerge or persist after therapy completion, such as pain and cognitive function. She notes that perhaps nursing check-ins may provide supportive care for fatigue/insomnia, but regardless, clinicians need to counsel on the disease-free survival benefit in the context of early symptom burden.
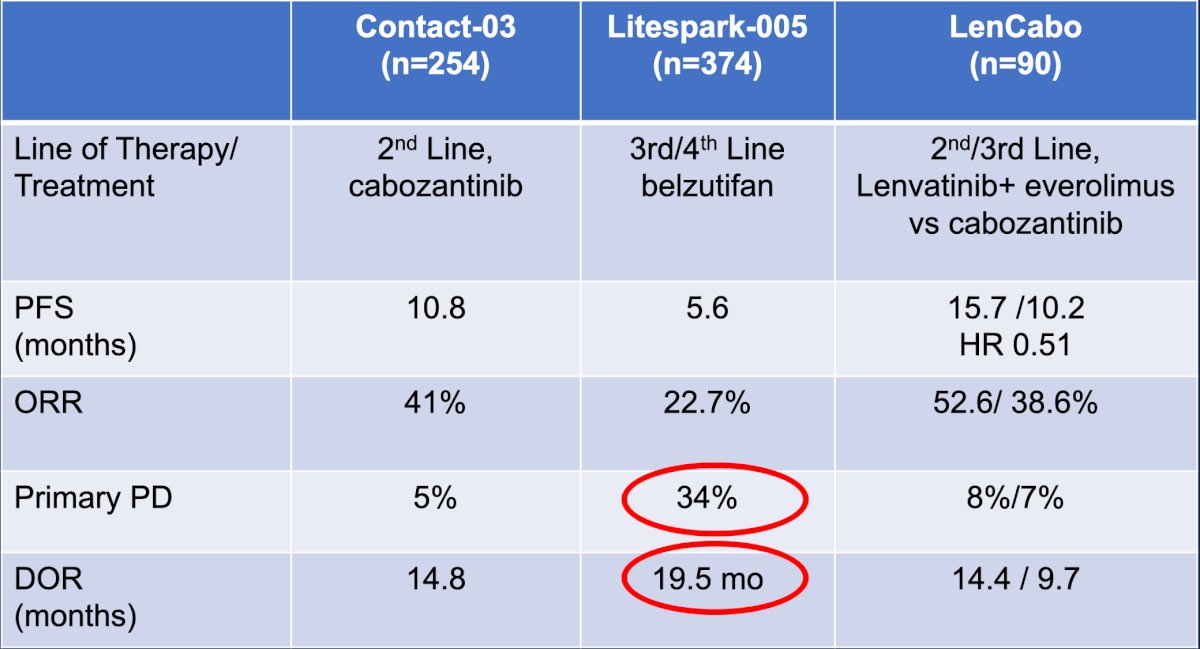
Finally, Dr. Beckermann discussed the LITESPARK-011 trial, first highlighting the limited durable options available after metastatic post-PD1 progression:
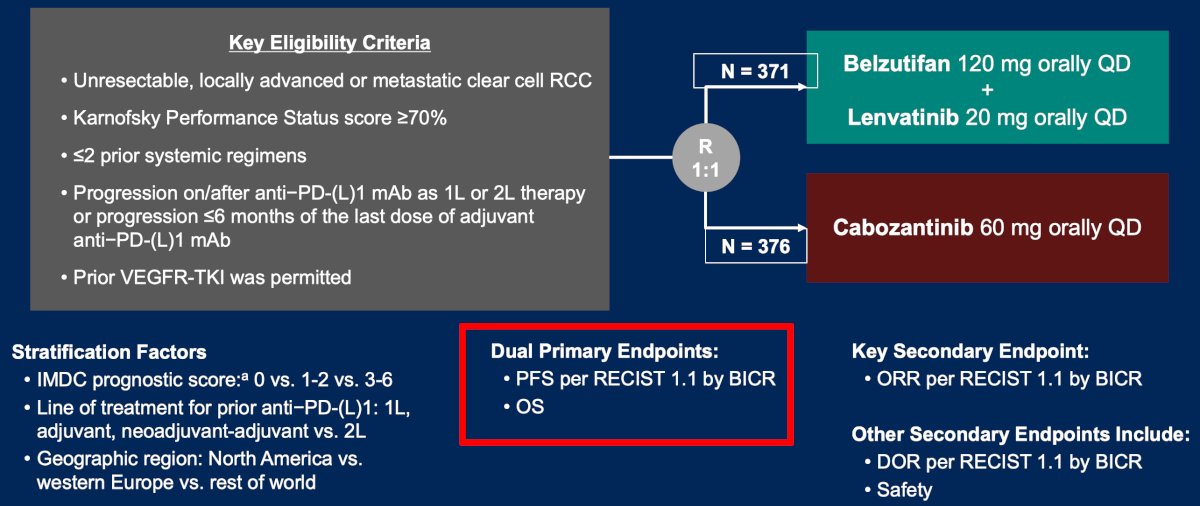
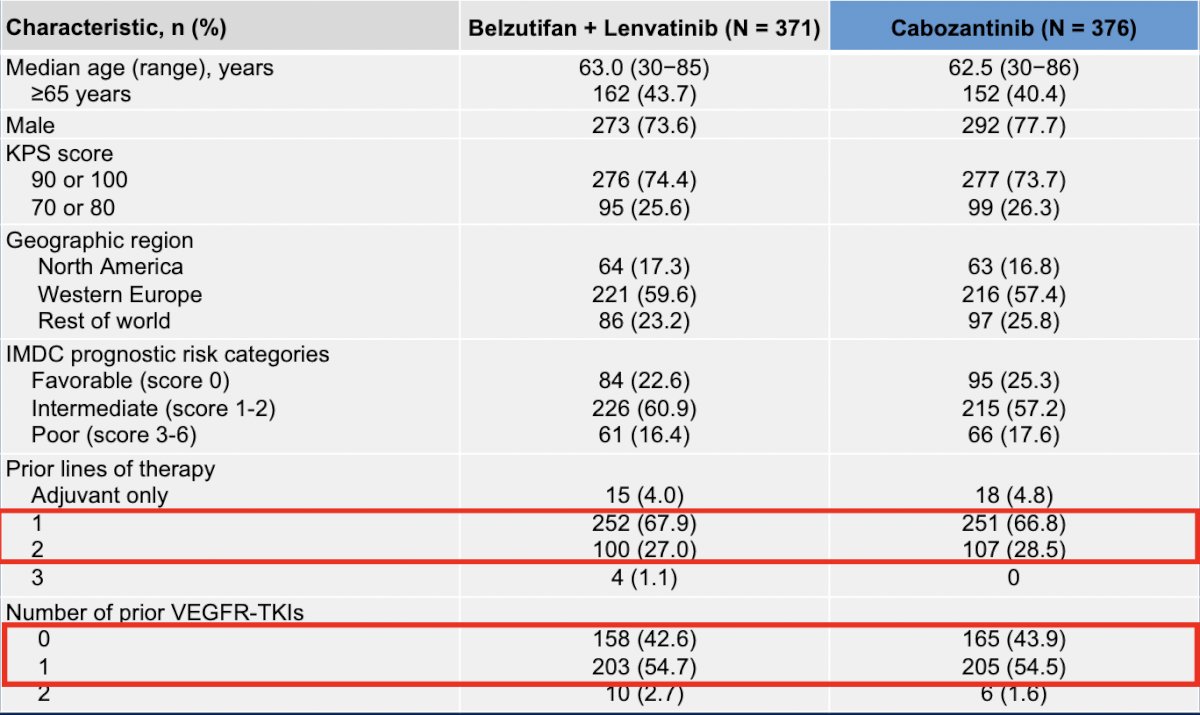
In LITESPARK-011, eligible patients were ≥18 years old with advanced clear cell RCC that progressed on or after first line or second line anti–PD-(L)1 therapy or ≤6 months of last dose of adjuvant anti–PD-(L)1 therapy. Patients were randomized 1:1 to belzutifan 120 mg + lenvatinib 20 mg QD versus cabozantinib 60 mg QD. The dual primary endpoints were progression-free survival by blinded independent central review per RECIST 1.1 and overall survival. Secondary endpoints included objective response rate (key secondary endpoint) and duration of response by blinded independent central review per RECIST 1.1, and safety:
The majority of patients received belzutifan + lenvatinib in the second line, with 43% of patients having not received a prior TKI:
Belzutifan + lenvatinib had a median progression-free survival of 14.8 months versus 10.7 months for cabozantinib, which was statistically significant (HR 0.70, 95% CI 0.59-0.84). At the time of the second interim analysis, the median overall survival was 34.9 months for belzutifan + lenvatinib versus 27.6 months in the cabozantinib arm (HR 0.85, 95% CI 0.68-1.05). The objective response rate for belzutifan + lenvatinib was 52.6% (including 5.4% complete response) versus 40.2% (including 1.1% complete response) for cabozantinib: 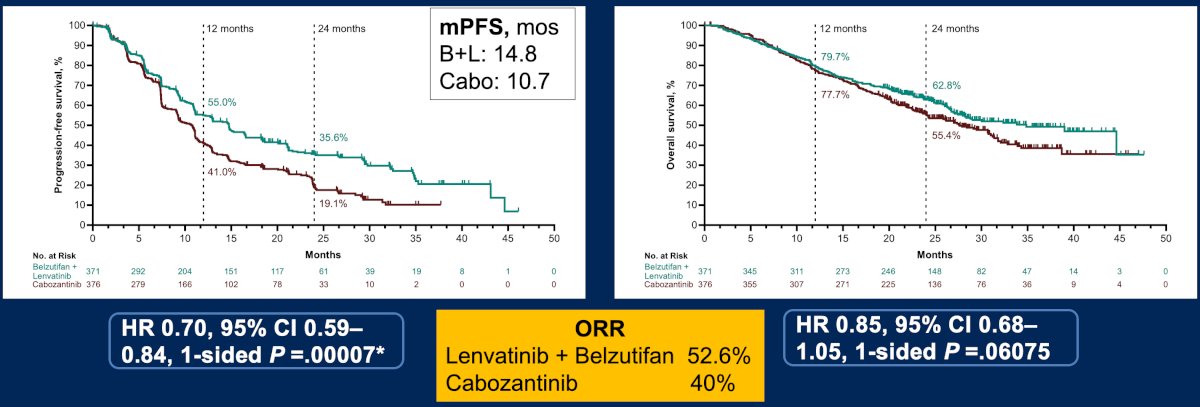
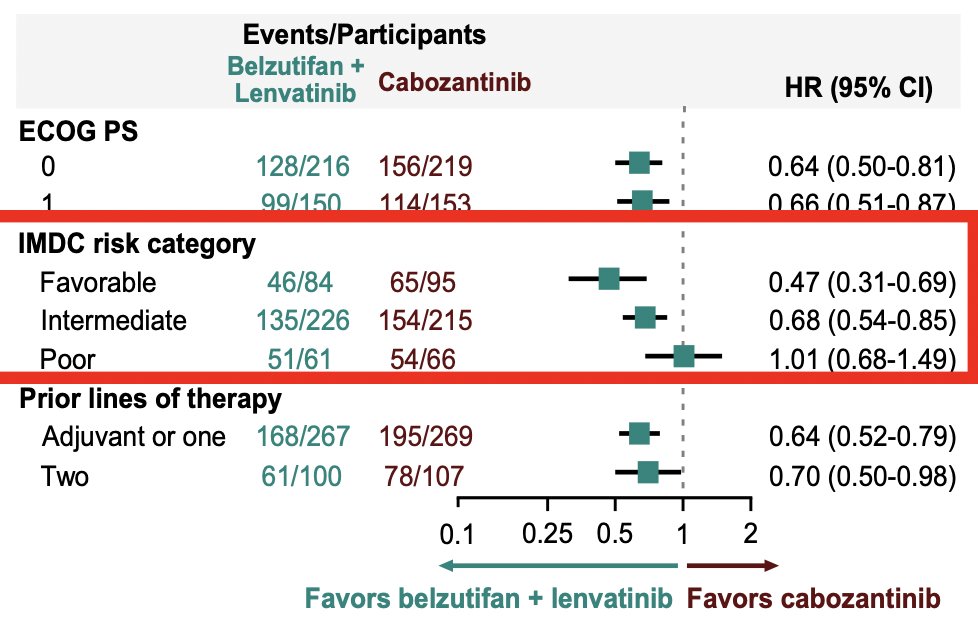
There are several notable findings, including (i) the progression-free survival tail suggests a durable control in a subset of patients, (ii) overall survival data are immature and not yet significant, and (iii) early events are driven by heterogeneity and aggressive biology, while later separation reflects the more indolent disease where durability differs. Dr. Beckermann emphasized that one of the key takeaway points from this trial is that when assessing the IMDC subgroup, the belzutifan + lenvatinib effect is strongest in favorable-risk disease, remains meaningful in intermediate-risk disease, and essentially disappears in poor-risk patients:
Toxicity was not inconsequential in LITESPARK-011, including anemia (69%), hypoxia (15%), and cardiac dysfunction (7%). Additionally, 33% of patients required a belzutifan dose reduction, 66% a lenvatinib dose reduction, 17% discontinued belzutifan, and 21% discontinued lenvatinib.
Dr. Beckerman concluded her discussion of LITESPARK-011 with the following messages and outstanding questions:
- Lenvatinib + belzutifan demonstrates a higher progression-free survival and a clinically meaningful duration of response
- Toxicity will drive patient selection and real-world feasibility
- Who are the durable responders, and can we predict them?
- What happens after discontinuation?
- What will be the final overall survival outcomes, and what are the salvage treatment choices?
Dr. Beckermann concluded her discussant presentation by highlighting her Monday morning clinic message:
- Adjuvant (NED) treatment:
- Shared decision making: disease-free survival gain versus toxicity/monitoring burden
- Best fit: prioritizing disease-free survival delay and ability to tolerate anemia/hypoxia risk
- For NED patients, the patient experience and quality of life must be part of the discussion
- We need an overall survival benefit
- Post PD-1 metastatic RCC patients:
- Lenvatinib + belzutifan is a new option after PD-1
- Patient selection, not escalation, is the challenge
- Baseline anemia, cardiac, pulmonary risk, and prior TKI tolerance need to be assessed
Presented by: Kathryn Beckermann, MD, PHD, Medical Director of GU Clinical Research/ Medical Oncology, Tennessee Oncology, Nashville, TN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.