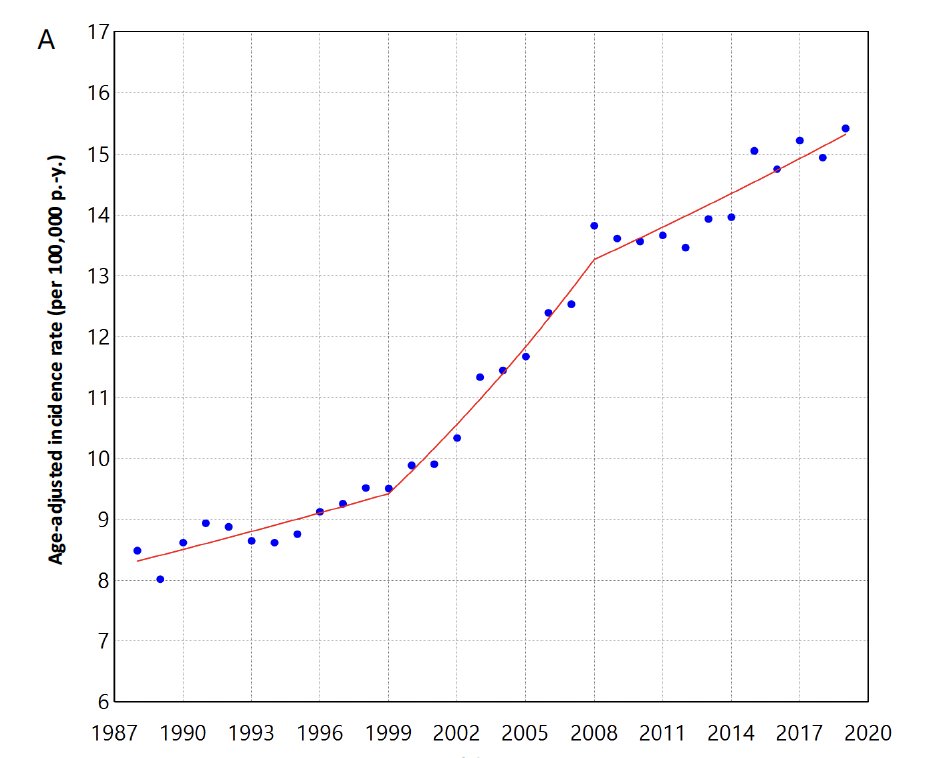
(UroToday.com) The 2026 GU ASCO annual meeting featured an "Innovations in kidney cancer in 2026" session and a presentation by Dr. Shuchi Gulati discussing the current state of the art of imaging for renal cell carcinoma (RCC). There has been a rising incidence of kidney cancer noted between the 1990s-2010, which may reflect increased use and availability of imaging techniques:
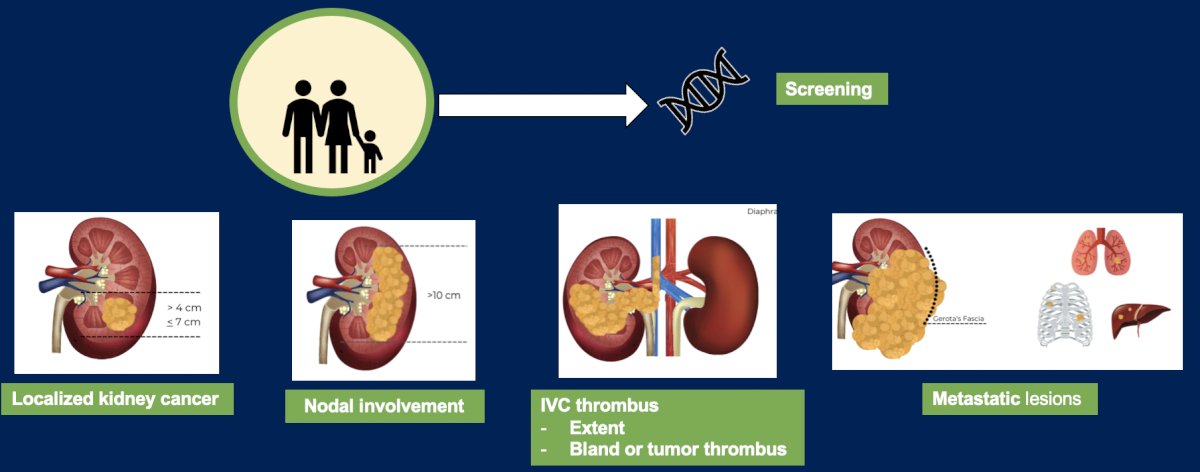
There are several imaging scenarios for kidney cancer, including localized disease, nodal involvement, IVC thrombus (assessing extent and bland versus tumor thrombus), and metastatic disease assessment:
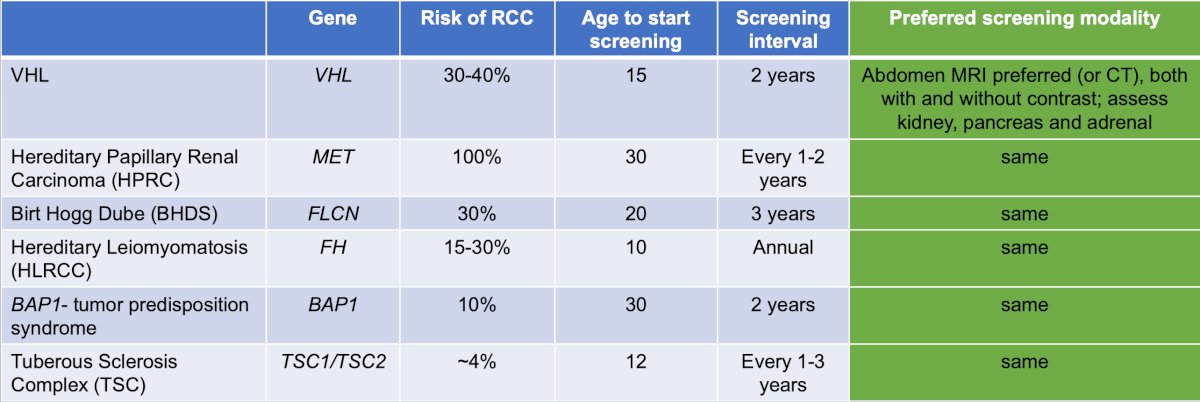
Dr. Gulati then presented a case vignette highlighting hereditary kidney cancer. This was a 19-year-old man recently diagnosed with genetically confirmed VHL after his father was found to carry a pathogenic VHL mutation following resection of a clear cell RCC. He is currently asymptomatic with a normal physical exam. Notably, he is concerned about “lifelong scans and radiation”. He asked ChatGPT and was informed that “CT scans use ionizing radiation. If someone with VHL had repeated CT scans of the abdomen and chest every year for decades, cumulative radiation exposure could become significant”. So, what is the preferred baseline abdominal imaging modality? Contrast-enhanced MRI, contrast-enhanced CT, ultrasound first and an MRI if abnormal, or MRI without contrast? For hereditary kidney cancer screening, the NCCN guidelines recommend an MRI of the abdomen (preferred; or CT scan), both with and without contrast to assess the kidneys, pancreas, and adrenal glands, typically at an interval of 1-2 years, depending on the syndrome:
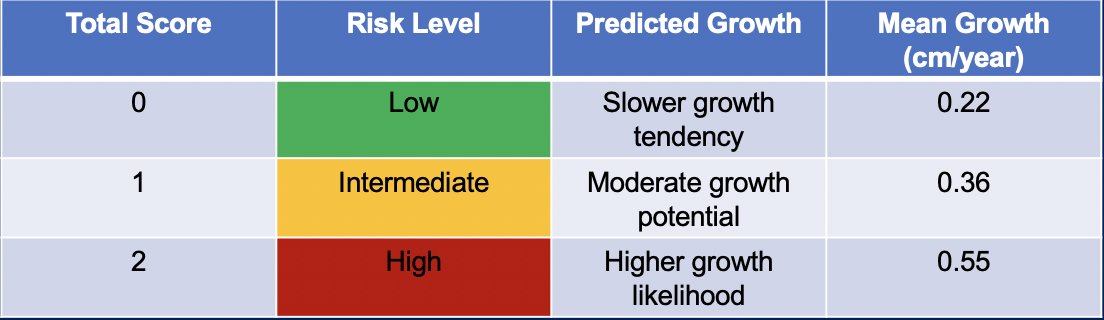
The MRI-based Kidney Imaging Surveillance Scoring System (KISSS) in VHL is based on:
- Tumor composition
- Predominantly cystic Score 0
- Mixed/predominantly solid Score 1
- Diffusing Restriction (ADC b500-800):
- Signal <= cortex Score 0
- Signal > cortex Score 1
For lymph node metastases in RCC, there are several pros and cons to using a CT or MRI:
- CT scan: overall median sensitivity of 76% and specificity of 79%
- Pros
- Short axis diameter > 1 cm
- Shape
- Enhancement characteristics (ie. necrosis)
- Cons
- Micro-metastases < 1 cm can be missed
- Even nodes > 1 cm can have reactive hyperplasia (up to 58%)
- Pros
- MRI: overall median sensitivity of 100% and specificity of 92%
- Pros
- Short axis diameter > 1 cm
- Shape
- Signal intensity on T2W (ie, necrosis?)
- Cons: micro-metastases <1 cm can be missed
- Pros
Functional imaging may have a role in assessing lymph node metastases. Previous reports (small sample sizes) have shown that FDG-PET/CT has a detection rate of 94%, and 89Zr-DFO-girentuximab PET/CT has a detection rate of 83%.
Dr. Gulati then discussed imaging tumor thrombi in RCC, noting that contrast-enhanced CT and MRI have equal efficacy for the detection of tumor thrombus. However, in some cases, an MRI may be warranted for surgical planning and to distinguish tumor thrombus from bland thrombus: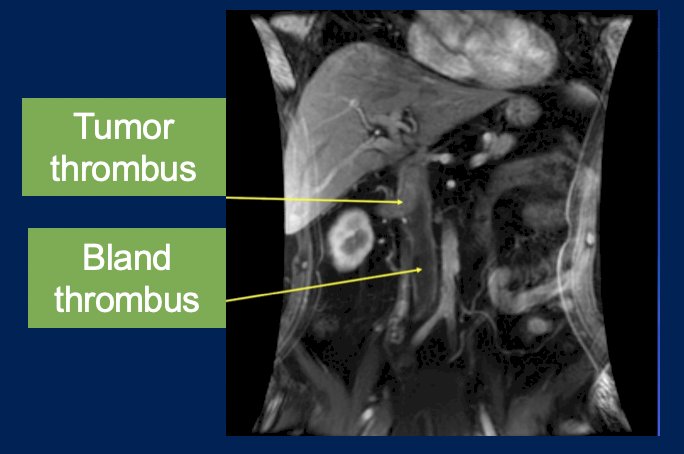
Ultimately, we should consider an MRI as an alternative to CT for: (i) hereditary cancers, (ii) patients with contrast allergies, (iii) pregnant patients in order to avoid radiation exposure and gadolinium, (iv) nodal metastases, (v) IVC thrombus evaluation, and (vi) assessment of liver metastases.
Dr. Gulati presented a second case vignette of a 44-year-old man who presented with a 4.3-cm incidental left-sided renal mass found during workup of lupus nephritis. On dedicated contrast-enhanced MRI, the tumor is avidly enhancing. Given his history of lupus nephritis and related concerns over a decline in renal function, the patient elects to undergo a biopsy prior to deciding on the mode of treatment. The core needle biopsy suggests an oncocytic renal neoplasm. Possible next steps may include:
- Additional imaging with a contrast-enhanced CT
- Ultrastructural evaluation with electron microscopy
- Repeat biopsy and tissue assessment with IHC
- Another imaging modality
- Surgery
Dr. Gulati then discussed the role of 99mTc-sestamibi imaging in the diagnosis of benign and indolent renal masses, with the following representative SPECT/CT images:
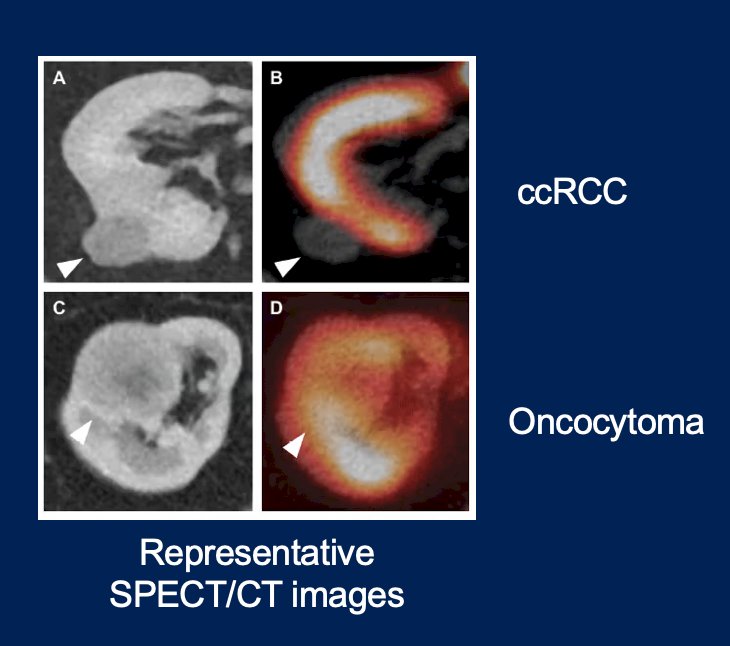
In a recent study from Rowe et al,1 they evaluated the accuracy of 99mTc-sestamibi SPECT/CT imaging for characterizing histologically diagnosed renal masses using 2 cohorts of patients; one from a prospective scan and resect clinical trial and a second from routine clinical care. Among 344 patients with 361 tumors, most clear cell RCC (97%) and papillary or clear cell papillary RCC (80%-84%) were cold, while chromophobe RCCs were equally likely to be hot or cold (52% versus 48%). Surgically resected oncocytoma tended to be hot (69%), with even higher positivity for biopsy with oncocytic neoplasms (87%): 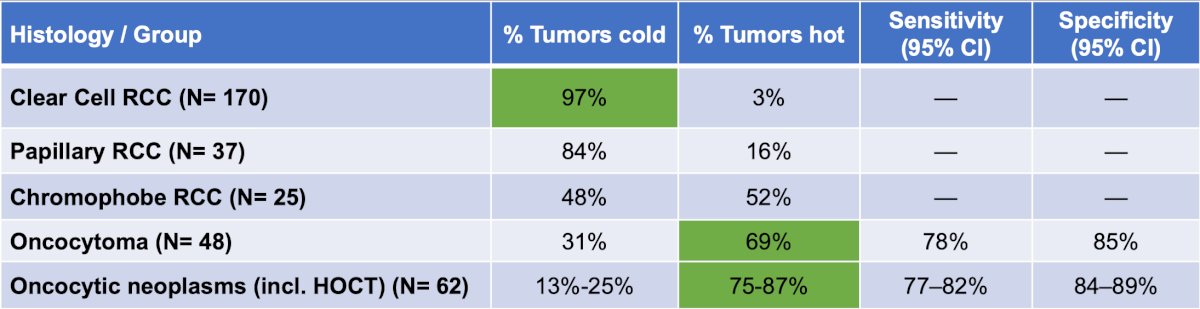
99mTc-sestamibi SPECT/CT shows promising diagnostic performance for risk-stratifying renal masses and could reduce unnecessary biopsies or resections when interpreted alongside clinical and histologic context.
The ZIRCON trial2 was an open-label, multicenter clinical trial including patients with an indeterminate renal mass (≤ 7 cm; tumor stage cT1) who were scheduled for partial nephrectomy within 90 days from planned 89Zr-DFO-girentuximab administration. Enrolled patients received a single dose of 89Zr-DFO-girentuximab IV (37 MBq ± 10%; 10 mg girentuximab) on Day 0 and underwent PET/CT imaging on Day 5 (± 2 days) prior to surgery. Of 284 evaluable patients included in primary analysis, the average across all 3 readers for sensitivity and specificity was 86% [95% CI 80%, 90%] and 87% [95% CI 79%, 92%], respectively, for co-primary endpoints, and 85% [95% CI 77%, 91%] and 90% [95% CI 79%, 95%], respectively, for key secondary endpoints:
![The ZIRCON trial2 was an open-label, multicenter clinical trial including patients with an indeterminate renal mass (≤ 7 cm; tumor stage cT1) who were scheduled for partial nephrectomy within 90 days from planned 89Zr-DFO-girentuximab administration. Enrolled patients received a single dose of 89Zr-DFO-girentuximab IV (37 MBq ± 10%; 10 mg girentuximab) on Day 0 and underwent PET/CT imaging on Day 5 (± 2 days) prior to surgery. Of 284 evaluable patients included in primary analysis, the average across all 3 readers for sensitivity and specificity was 86% [95% CI 80%, 90%] and 87% [95% CI 79%, 92%], respectively, for co-primary endpoints, and 85% [95% CI 77%, 91%] and 90% [95% CI 79%, 95%], respectively, for key secondary endpoints:](/images/com-doc-importer/249-asco-gu-2026/asco-gu-2026-imaging-for-renal-cell-carcinoma-current-state-of-the-art/image-7.jpg)
89ZrZr-girentuximab PET–CT has shown to have a favorable safety profile and proven to be a highly accurate, non-invasive imaging modality for the detection and characterization of clear cell RCC.
Dr. Gulati presented a third case vignette of a 28-year-old male patient admitted to the hospital with cord compression. A CT scan revealed a 10.3 cm renal mass with several metastatic lymph nodes and pulmonary nodules. A biopsy showed carcinoma, high grade, not otherwise specified, and additional IHC findings supported RCC. Subsequently, tissue NGS showed an SDHB S239fs*8 mutation, confirming SDH-deficient RCC. At this time, what is the preferred modality for baseline staging? Contrast-enhanced CT of the chest, abdomen, and pelvis? MRI abdomen + chest CT? Whole body MRI? FDG PET/CT?
The nature of SDH-deficient RCC is a complete loss of SDH and FH, leading to an accumulation of upstream metabolites (such as succinate) and disruption of metabolic pathways that depend on the TCA cycle, which leads to increased aerobic glycolysis. Generally, there are biological and technical limitations of 18FDG-PET and 18FDG PET/CT in RCC:
- Variable tumor glycolysis
- Reduced/ heterogeneous GLUT1/GLUT3 expression and non glycolytic metabolism
- Variable tumor uptake
- Renal excretion of FDG obscures primary and urothelial lesions
- Reduced sensitivity and negative predictive value for primary tumors
- No clear diagnostic advantage over contrast-enhanced CT
- Not recommended for routine diagnosis or staging
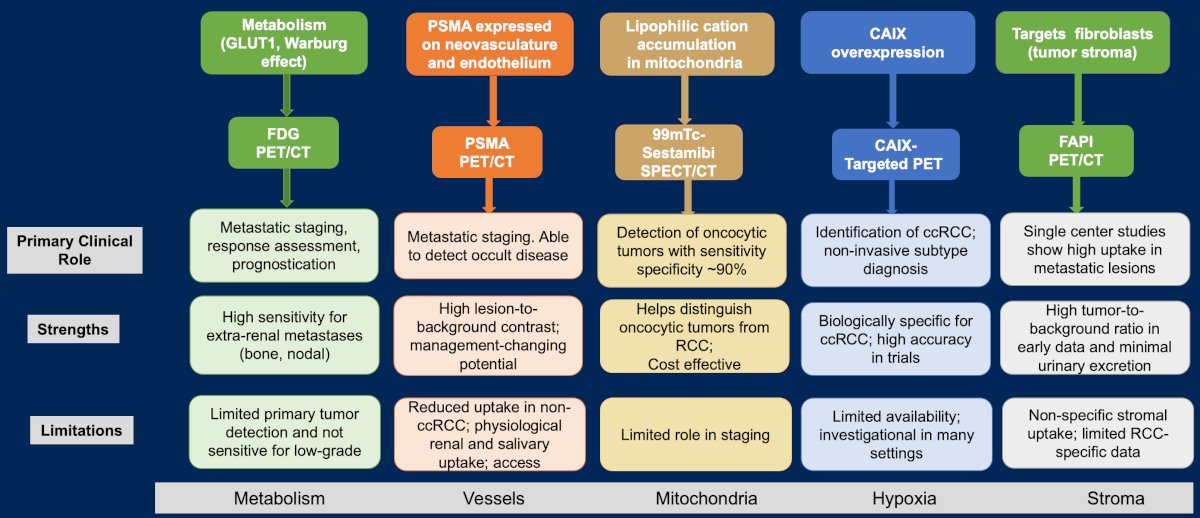
What scenarios can PET scans still be useful in? Dr. Gulati notes that an FDG/PET (i) may improve prognostication in metastatic RCC, (ii) may assist with treatment decisions such as incorporation of metastasectomy or stereotactic body radiotherapy in non-metastatic RCC, and (iii) may be incorporated to improve detection of bone metastases. The following figure highlights biology-driven PET-radiotracers in RCC:
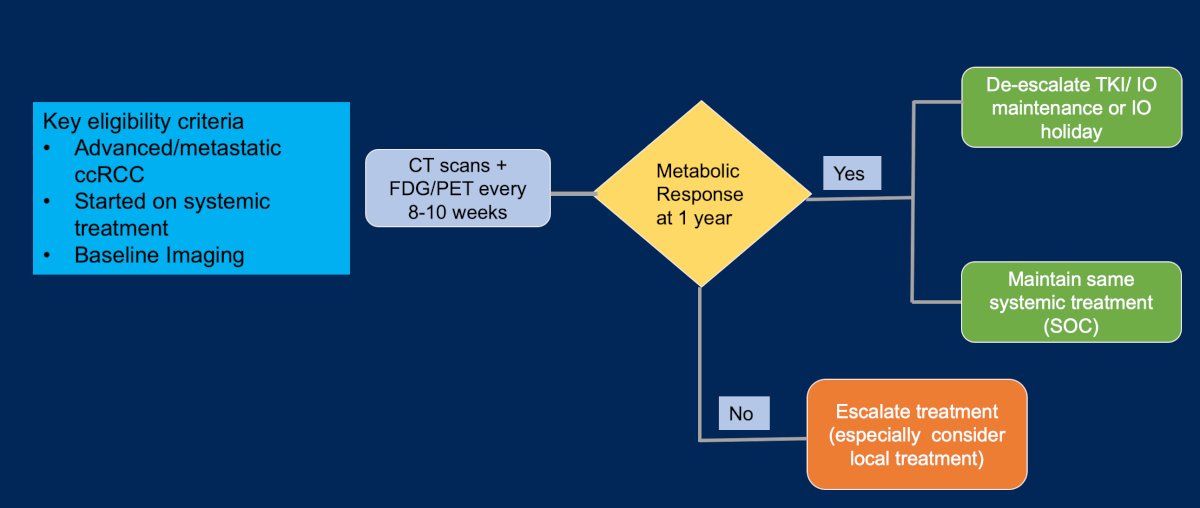
Future directions include incorporating novel imaging into clinical trials:
Dr. Gulati concluded her presentation discussing the current state of the art of imaging for RCC with the following take-home points:
- Imaging in RCC is central to staging, therapy selection, and response assessment
- It is imperative to know when to use each modality
- New imaging modalities need to be validated in clinical trials
Presented by: Shuchi Gulati, MD, MSc, University of California Davis School of Medicine and the UC Davis Comprehensive Cancer Center, Sacramento, CA
References:
- Rowe SP, Murtazaliev S, Amindarolzarbi A, et al. Performance of 99mTc-sestamibi single-photon emission computed tomography/computed tomography for characterizing renal masses: Combined results from a prospective scan-and-resect trial and clinical experience. J Urol. 2026 Jan 8 [Epub ahead of print].
- Shuch B, Pantuck AJ, Bernhard JC, et al. [89Zr]Zr-girentuximab for PET-CT imaging of clear-cell renal cell carcinoma: A prospective, open-label, multicentre, phase 3 trial. Lancet Oncol. 2024 Oct;25(10):1277-1287.