(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Balaji Venugopal discussing a subgroup analysis from the JAVELIN Renal 101 trial assessing efficacy and safety of avelumab + axitinib versus sunitinib in patients with very favorable risk advanced RCC. In the JAVELIN Renal 101 phase 3 trial, first-line treatment with avelumab + axitinib in patients with advanced renal cell carcinoma (RCC) significantly prolonged progression-free survival and increased the objective response rate versus sunitinib, irrespective of International Metastatic RCC Database Consortium (IMDC) risk group or number of IMDC risk factors.1
In the final analysis, overall survival results favored avelumab + axitinib versus sunitinib but did not reach statistical significance.2 A previous study in patients with favorable risk within the IMDC dataset identified a very favorable-risk subgroup, defined as patients with time from primary diagnosis to systemic therapy ≥3 years, Karnofsky performance status >80, and no brain, liver, or bone metastasis. At ASCO GU 2026, Dr. Venugopal reported post hoc analyses in patients with very favorable-risk advanced RCC.
In JAVELIN Renal 101 (NCT02684006), eligible patients with untreated advanced RCC (any IMDC score) were randomized 1:1 to receive avelumab + axitinib or sunitinib. In this exploratory analysis, progression-free survival and objective response rate per investigator assessment (RECIST 1.1), overall survival, and safety were assessed in the subgroup with very favorable risk.
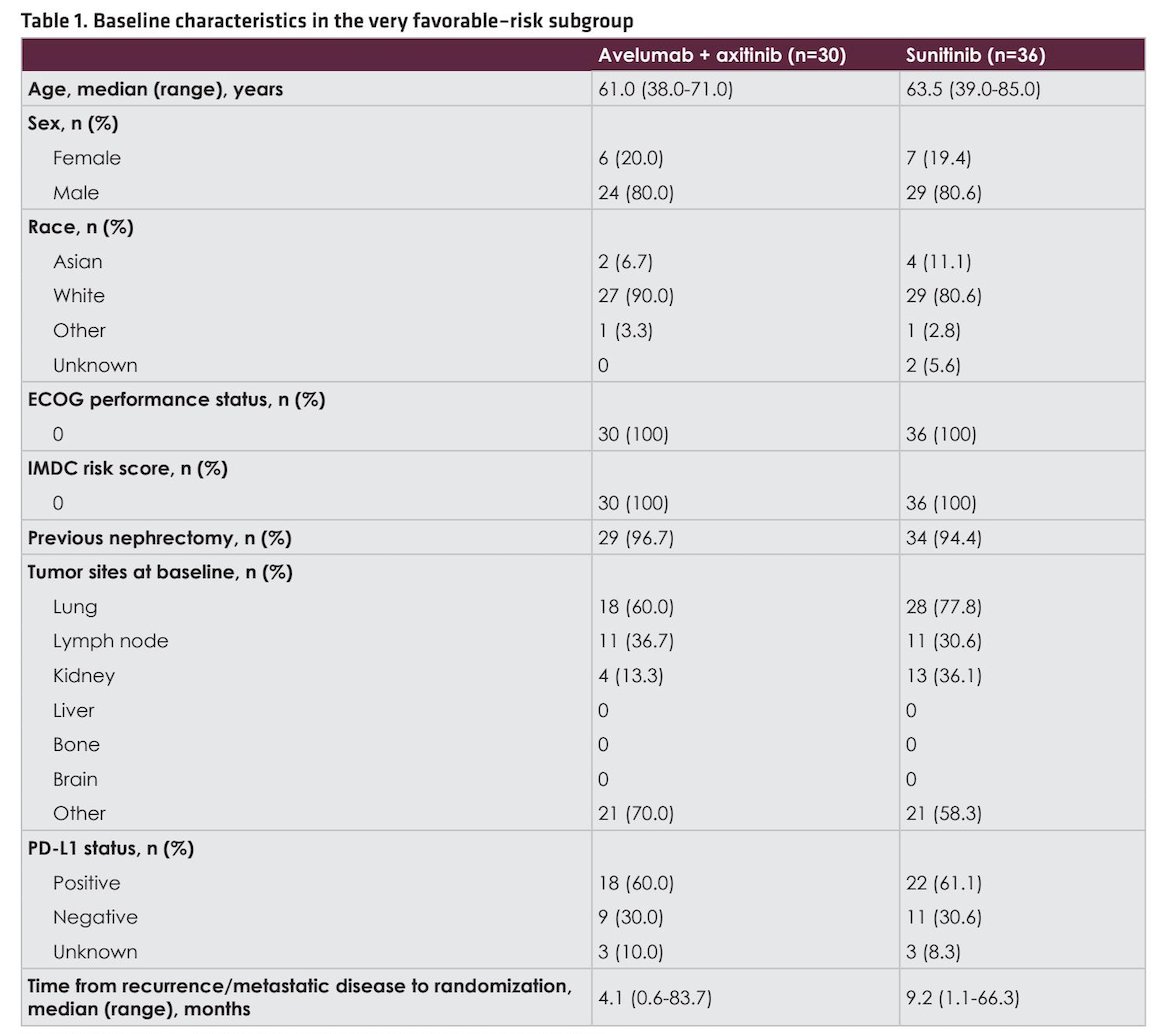
In the avelumab + axitinib (n = 442) and sunitinib (n = 444) arms, respectively, 30 (6.8%) and 36 (8.1%) patients had very favorable risk disease. Within these subgroups, the median age was 61.0 and 63.5 years, 96.7% and 94.4% patients had previous nephrectomy, and 60.0% and 61.1% had positive PD-L1 status, respectively:
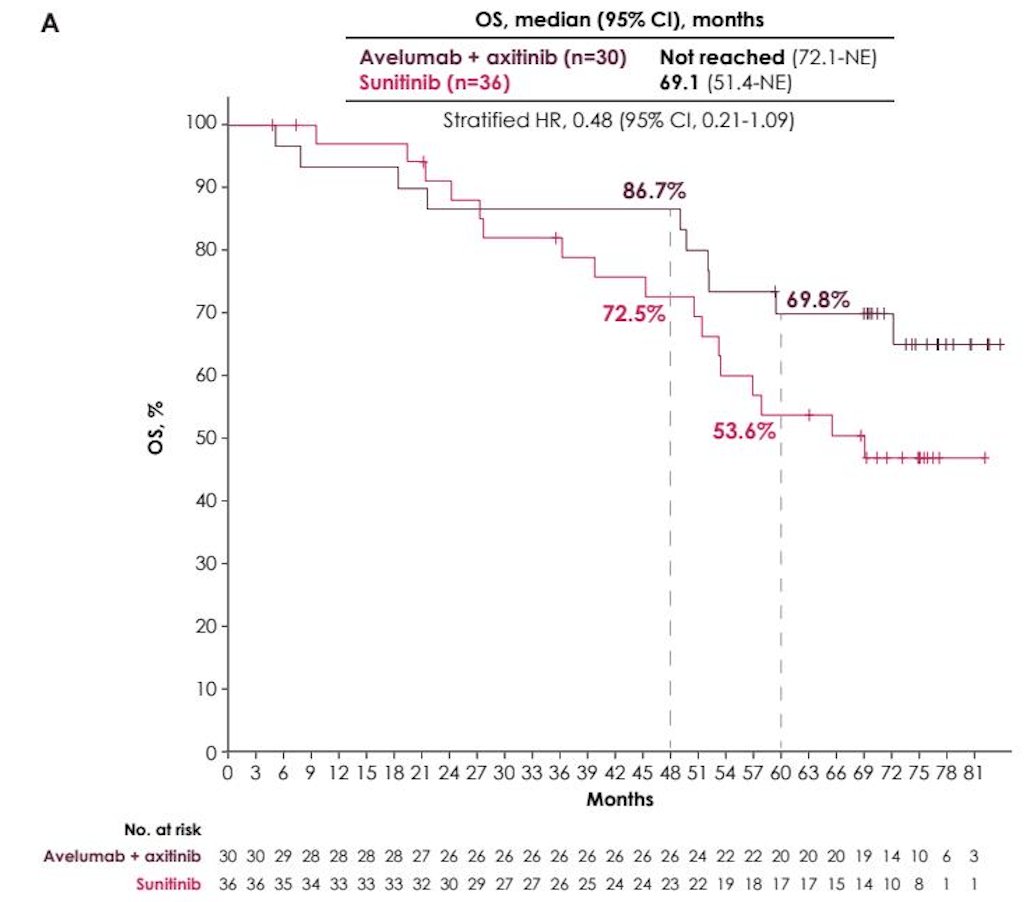
Follow-up was ≥68 months in all patients (data cutoff: August 31, 2023). In patients with very favorable risk disease in the avelumab + axitinib versus sunitinib arms, the median overall survival was not reached versus 69.1 months (HR 0.48, 95% CI 0.21-1.09):
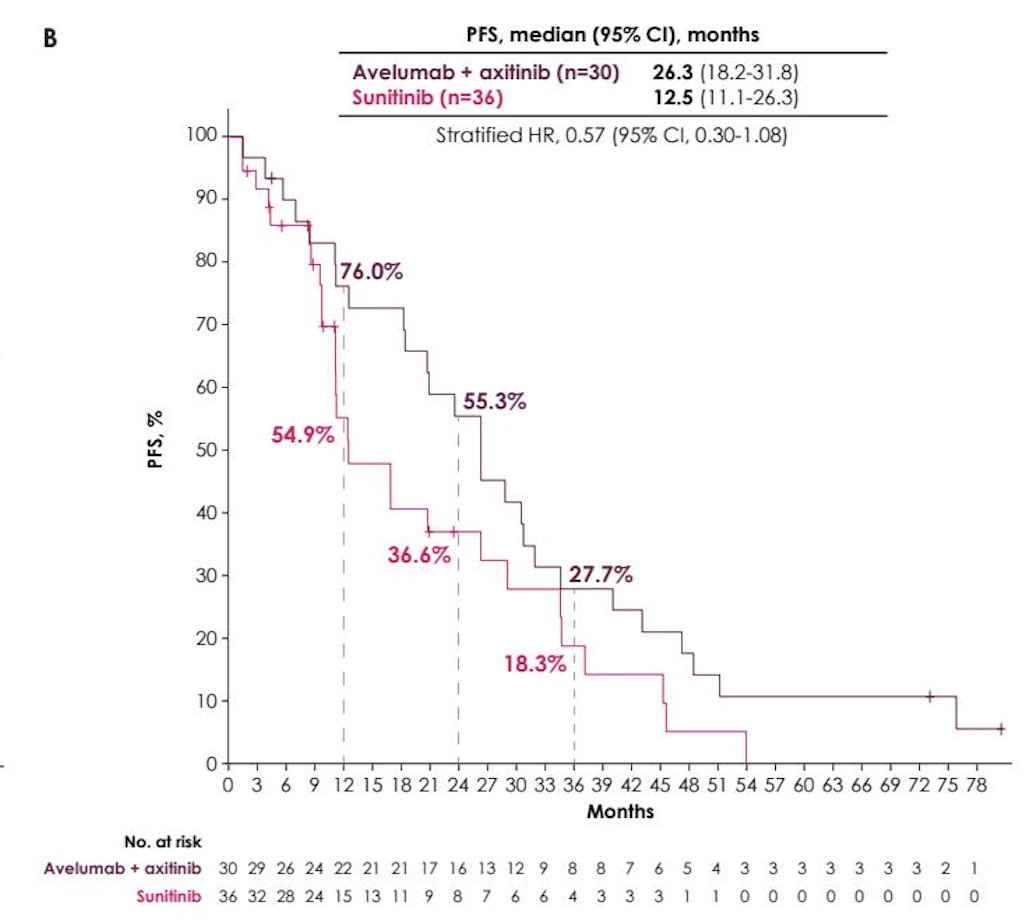
Regarding progression-free survival, patients with very favorable risk disease had a median of 26.3 months versus 12.5 months for the avelumab + axitinib versus sunitinib arms, respectively (HR 0.57, 95% CI 0.30-1.08):
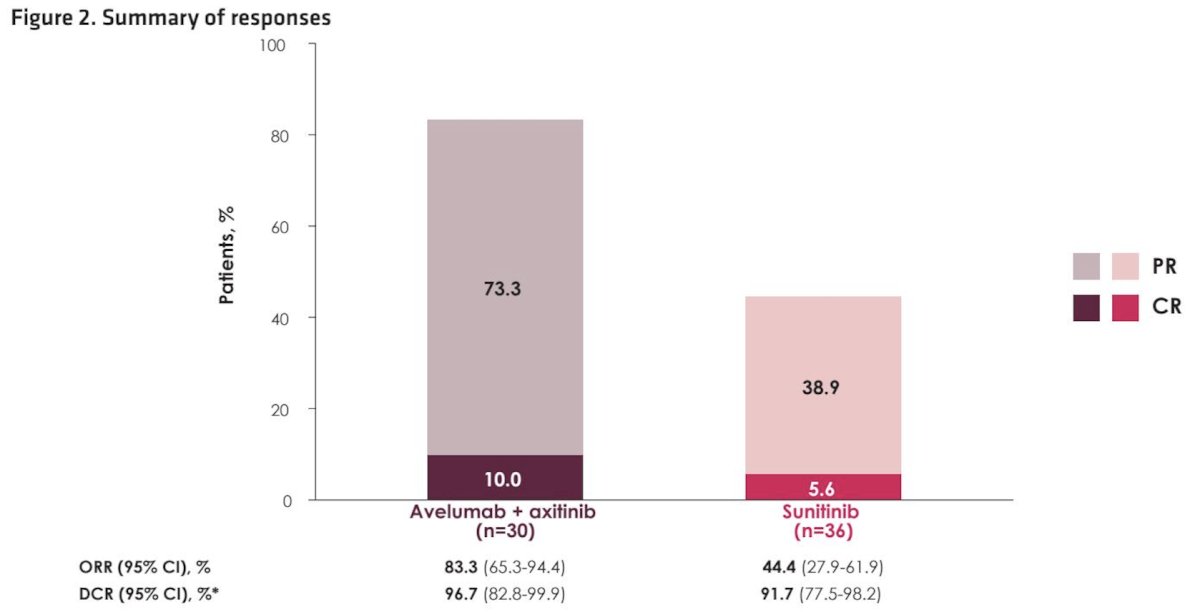
Objective response rates were 83.3% versus 44.4% for patients receiving avelumab + axitinib versus sunitinib, respectively:
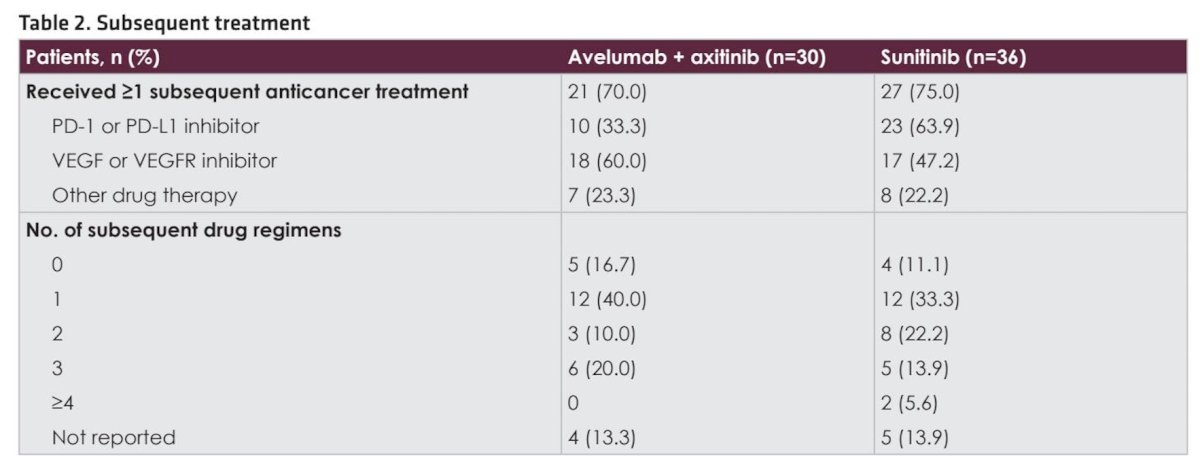
Subsequent anticancer drug treatments were received by 70.0% patients after avelumab + axitinib versus 75.0% after sunitinib, including a PD-(L)1 inhibitor in 33.3% versus 63.9%, respectively:
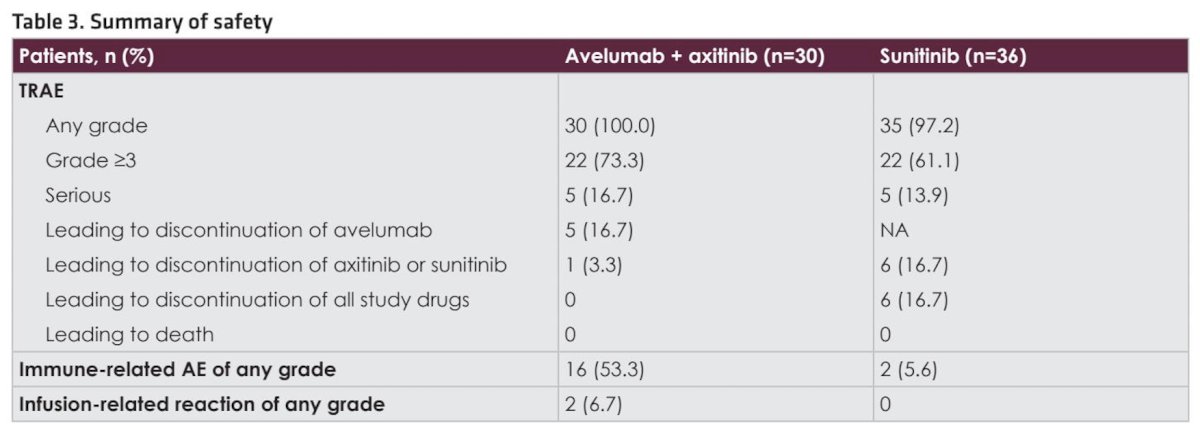
In the avelumab + axitinib versus sunitinib arms, respectively, treatment-related adverse events of any grade occurred in 100% versus 97.2% p patients, including grade ≥3 events in 73.3% versus 61.1%, and led to permanent discontinuation of all study drugs in 0% versus 16.7%:
Dr. Venugopal concluded his presentation discussing a subgroup analysis from the JAVELIN Renal 101 trial assessing efficacy and safety of avelumab + axitinib versus sunitinib in patients with very favorable risk advanced RCC with the following take-home points:
- Long-term efficacy benefits were observed with avelumab + axitinib versus sunitinib in the very favorable-risk subgroup, consistent with previous results in the overall population and IMDC favorable-risk group
- Median overall survival was not reached versus 69.1 months (HR 0.48, 95% CI, 0.21-1.09)
- Median progression-free survival was 26.3 versus 12.5 months (HR 0.57, 95% CI, 0.30-1.08)
- The objective response rate was 83.3% versus 44.4%
- Safety findings were consistent with previous results from the trial
- Overall, these results support the use of first-line avelumab + axitinib treatment in patients with very favorable-risk advanced RCC and suggest that a tailored treatment strategy may improve advanced RCC management in this population
Presented by: Balaji Venugopal, MBBS, MD, FRCP, Beatson West of Scotland Cancer Centre, Glasgow, UK
References:
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1103-1115.
- Choueiri TK, Motzer RJ, Rini BI, et al. Updated efficacy results from the JAVELIN Renal 101 trial: first-line avelumab plus axitinib versus sunitinib in patients with advanced renal cell carcinoma. Ann Oncol 2020 Apr 25;S0923-7534.