(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer trials in progress session and a presentation by Dr. Nazli Dizman discussing the phase II IVORY trial assessing ivonescimab in metastatic clear cell renal cell carcinoma (RCC) after immune checkpoint inhibitor therapy. Immune checkpoint inhibitor-based combinations, such as dual immune checkpoint inhibitors or immune checkpoint inhibitor plus a vascular endothelial growth factor tyrosine kinase inhibitor (VEGF-TKI), constitute the first-line treatment for metastatic clear cell RCC.
However, in the subsequent-line setting, adding immune checkpoint inhibitors to VEGF-TKIs did not demonstrate superior activity compared to VEGF-TKI monotherapy,1,2 highlighting the need for novel approaches to overcome immune checkpoint inhibitor resistance.
Ivonescimab is a first-in-class tetravalent bispecific antibody targeting PD1/PD-L1 and VEGF/VEGFR signaling, simultaneously inhibiting two key mechanisms of metastatic clear cell RCC pathogenesis: immune escape and angiogenesis.

In non-small cell lung cancer, ivonescimab has recently shown superiority over pembrolizumab (HARMONi-2). By spatially coordinated and simultaneous inhibition of PD-1 and VEGF pathways through a single molecule, Dr. Dizman and colleagues hypothesize that ivonescimab will enhance efficacy, address tumor heterogeneity, and reduce pharmacokinetic variability compared with separate agents.
This phase II, single-arm, open-label, investigator-initiated study evaluates the activity of ivonescimab monotherapy in patients with metastatic clear cell RCC previously treated with immune checkpoint inhibitors. Cohort 1 (n = 20) enrolls patients with no prior exposure to VEGF-directed agents, while Cohort 2 (n = 20) enrolls patients who have previously received VEGF-directed therapy. Ivonescimab is administered at a 20 mg/kg IV dose every 3 weeks until disease progression or unacceptable toxicities. Each cohort follows a time-to-event Bayesian Optimal Phase 2 (TOP) design, with simultaneous monitoring of two efficacy endpoints: objective response rate, defined as complete or partial response at any time, and disease control rate, defined as complete response, partial response, or stable disease at 24 weeks, per RECIST 1.1:
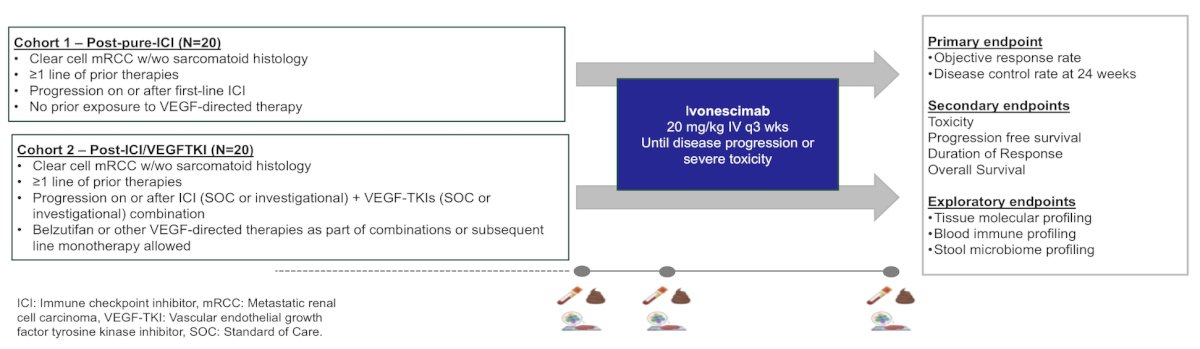
In cohort I, the null hypothesis is objective response rate is 10%, or the disease control rate is 30%, while the alternative hypothesis is objective response rate is 30%, or the disease control rate is 50%. The regimen will be deemed acceptable if more than 4 patients experience an objective response, or more than 9 patients experience disease control at 24 weeks, providing 96% power with 20% type I error rate. In cohort II, the null hypothesis is objective response rate is 5%, or the disease control rate is 20%, and the alternative hypothesis is objective response rate is 20%, or the disease control rate is 40%. The regimen will be considered acceptable if more than 2 patients experience an objective response, or more than 6 patients experience disease control at 24 weeks, with 91% power and 12.5% type I error rate.
Tissue, blood, and stool correlatives will be collected at baseline, during therapy, and at the end of treatment to identify changes in specific immune-cell and gut microbiome subsets and elucidate the dynamic evolution of tumor and immune-cell compartments as well as their spatial relationships following ivonescimab. As of February 6, 2026, a total of 19 patients have been enrolled.
Presented by: Nazli Dizman, MD, MD Anderson Cancer Center, Houston, TX
References:
- Pal SK, Albiges L, Tomczak P, et al. Atezolizumab plus cabozantinib versus cabozantinib monotherapy for patients with renal cell carcinoma after progression with previous immune checkpoint inhibitor treatment (CONTACT-03): A multicenter, randomized, open-label, phase 3 trial. Lancet 2023 Jul 15;402(10397):185-195.
- Choueiri TK, Albiges L, Barthelemy P, et al. Tivozanib plus nivolumab versus tivozanib monotherapy in patients with renal cell carcinoma following an immune checkpoint inhibitor: Results of the phase 3 TiNivo-2 study. Lancet. 2024 Oct 5;404(10460):1309-1320.