(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Laurence Albiges discussing novel investigative regimens for previously treated advanced clear cell RCC in the KEYMAKER-U03 substudy 03B. Immunotherapy-based combination regimens are the preferred first-line treatments for patients with advanced RCC, but approximately 30% of patients do not respond to treatment, and 70% will experience disease progression within 4 years of first-line treatment.
To date, there are no preferred second-line treatment options for patients with advanced clear cell RCC. The addition of agents with novel mechanisms of action to established treatment strategies may help improve outcomes for patients with previously treated advanced clear cell RCC. At ASCO GU 2026, Dr. Albiges and colleagues presented updated results from substudy 03B of KEYMAKER-U03, a phase I/II study evaluating novel regimens in clear cell RCC.
Adults with confirmed clear cell RCC and disease progression on or after PD-(L)1 inhibitor and VEGF-TKI were randomly assigned to open arms: pembrolizumab + quavonlimab (anti–CTLA-4), pembrolizumab + favezelimab (anti-LAG3), pembrolizumab + MK-4830 (anti-ILT4), pembrolizumab + belzutifan (HIF-2α inhibitor), belzutifan + lenvatinib (VEGF-TKI), and pembrolizumab + lenvatinib: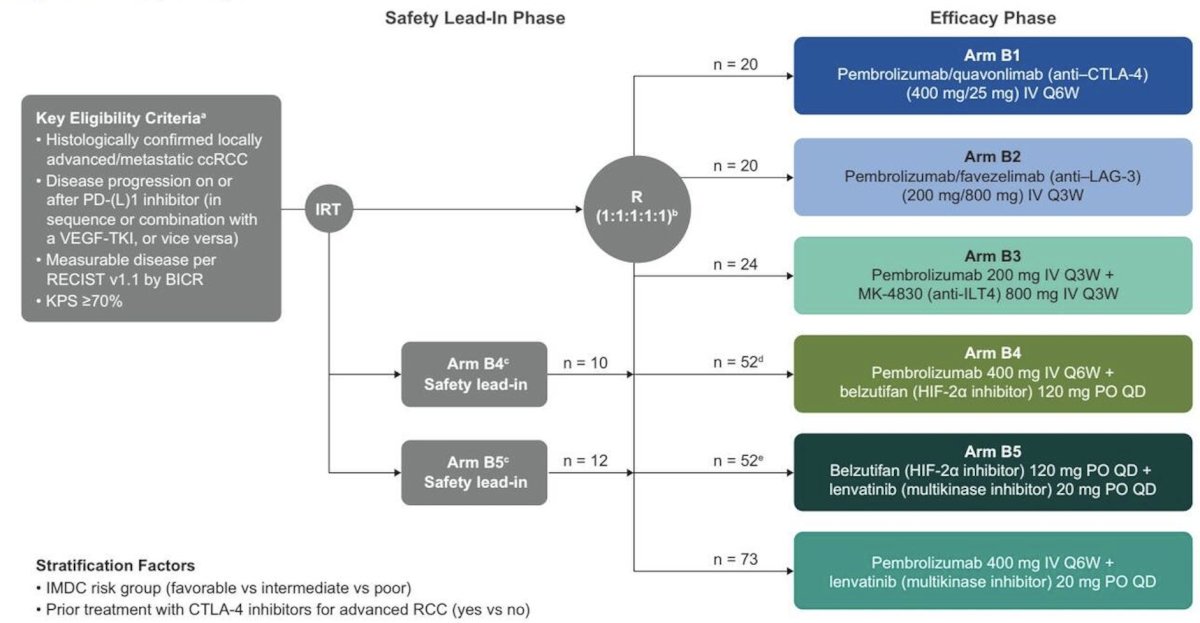
The primary endpoints were safety and confirmed objective response rate per RECIST v1.1 by blinded independent central review. Secondary end points included clinical benefit rate (complete response + partial response + stable disease ≥6 months), duration of response, and progression-free survival per RECIST v1.1 by blinded independent central review, and overall survival. No formal comparisons were made across arms. Enrollment was planned for 50 participants in each arm, although enrollment would be stopped if the 6-month progression-free survival rate was ≤40% among the first 20 enrolled participants per protocol design.
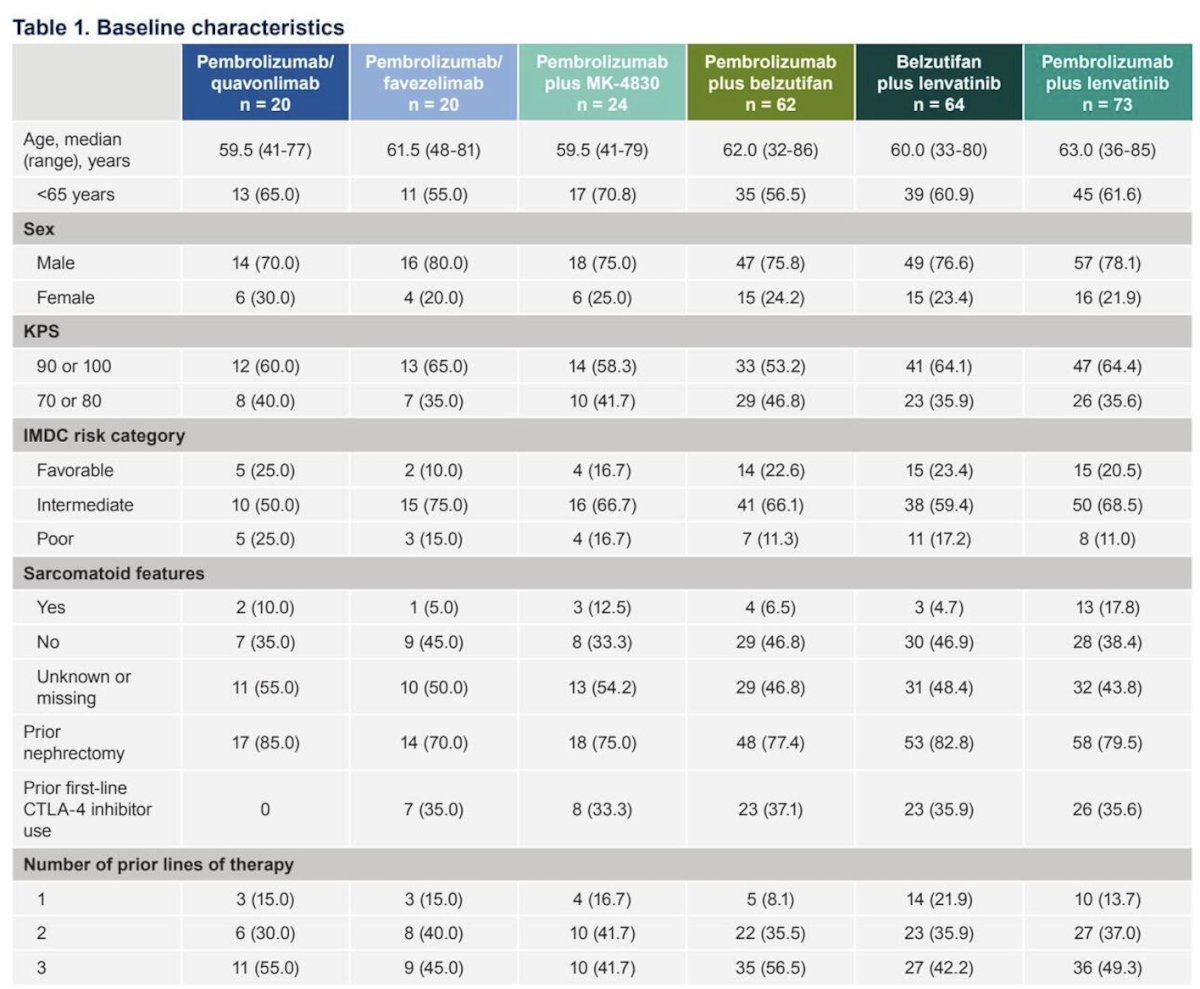
Overall, 263 participants were enrolled, with a median study follow-up of ≥22.9 months in all arms:
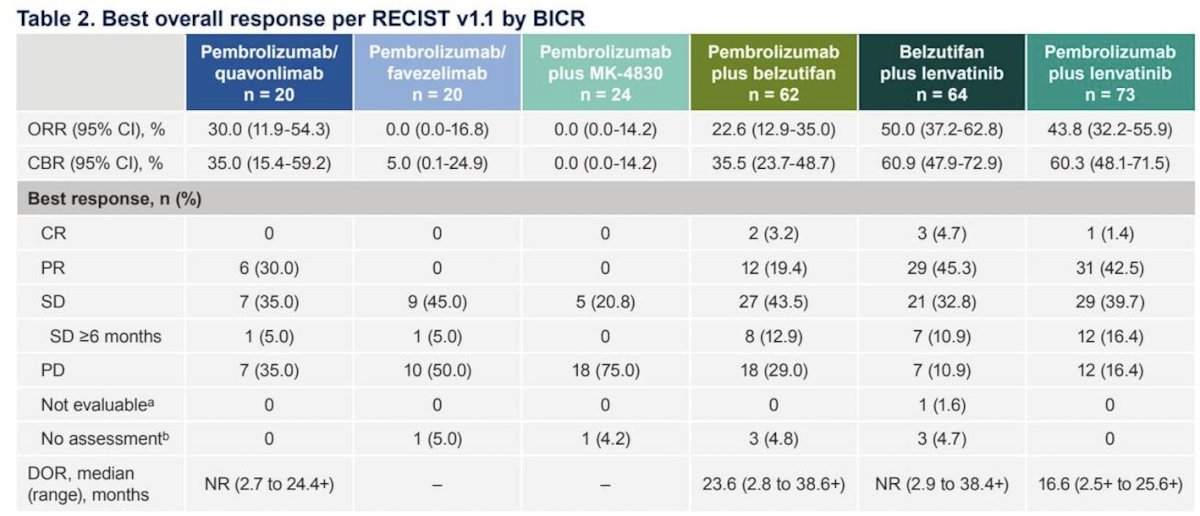
Efficacy results are reported in the following table, including an objective response rate ranging from 0%-50% across the six arms of treatment, with the highest being belzutifan + lenvatinib (50.0%):
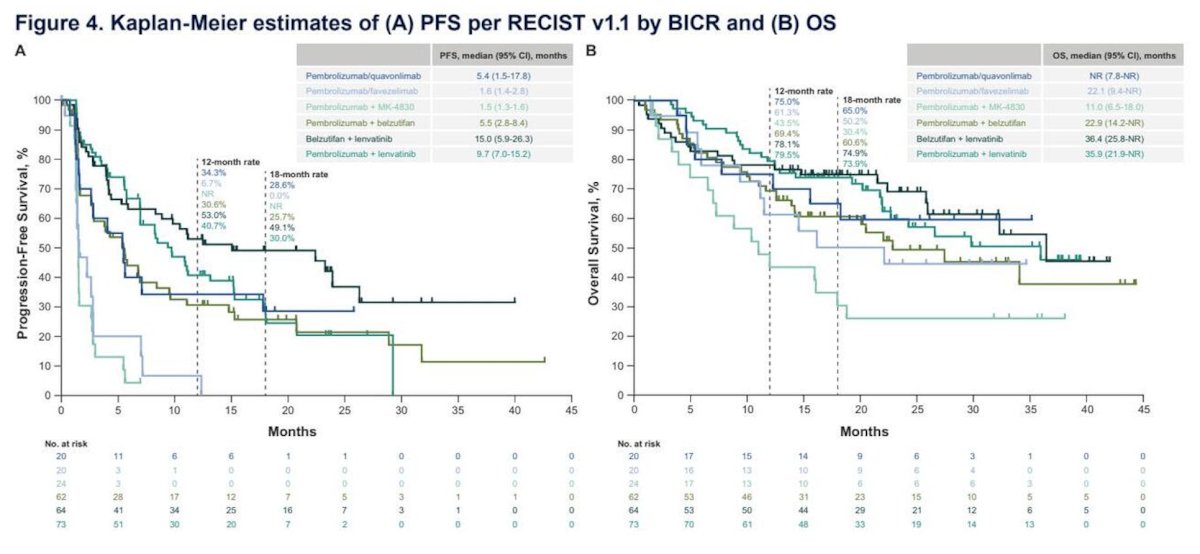
Moreover, across these groups, the median progression-free survival ranged from 1.5 to 15.0 months, and the median overall survival ranged from 11.0-not reached:
Grade 3-5 treatment-related adverse events occurred in 25.0%, 10.5%, 8.7%, 45.2%, 63.5%, and 52.1% of treated participants in the pembrolizumab + quavonlimab, pembrolizumab + favezelimab, pembrolizumab + MK-4830, pembrolizumab + belzutifan, belzutifan + lenvatinib, and pembrolizumab + lenvatinib arms, respectively. Treatment-related adverse events led to death in 2 participants in the belzutifan + lenvatinib arm (cerebral hemorrhage and intracranial hemorrhage) and 1 patient in the pembrolizumab + lenvatinib arm (esophageal perforation):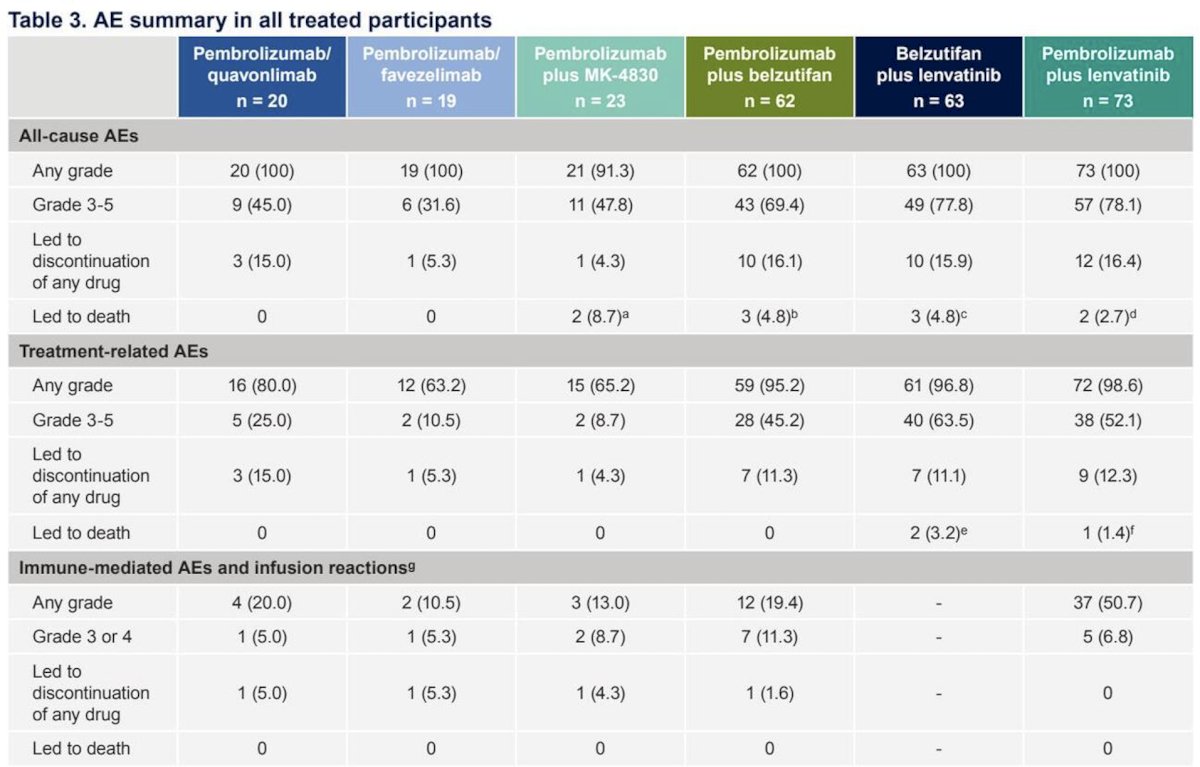
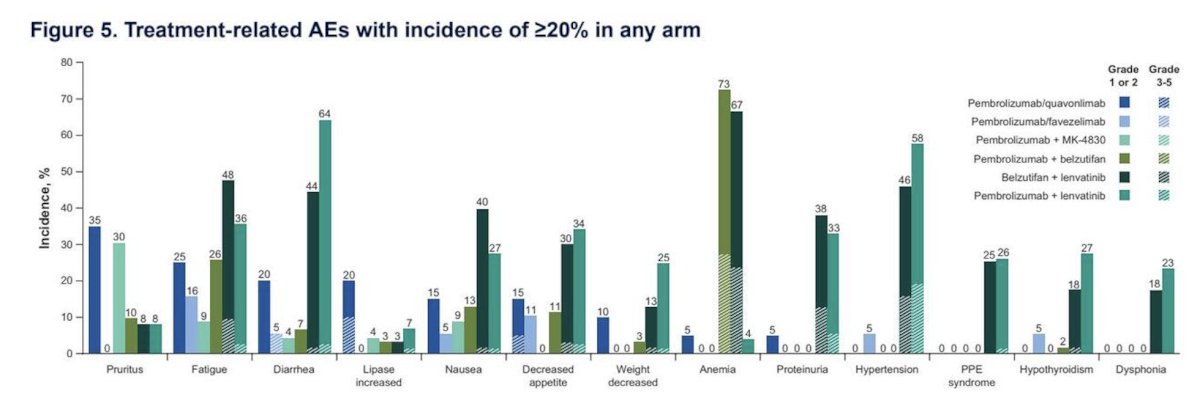
Across the six treatment arms, the most common treatment-related adverse events included anemia, diarrhea, hypertension, fatigue, and proteinuria:
Dr. Albiges concluded her presentation discussing novel investigative regimens for previously treated advanced clear cell RCC in the KEYMAKER-U03 substudy 03B with the following take-home points:
- With additional follow-up in the KEYMAKER-U03 substudy 03B trial, belzutifan + lenvatinib continued to show the highest antitumor activity in participants with heavily pretreated advanced clear cell RCC who had received both a PD-(L)1 inhibitor and VEGF-TKI therapy. The small sample size was a limitation of this study
- The phase 3 LITESPARK-011 trial confirms the antitumor activity of belzutifan + lenvatinib shown in this study
- No responses were observed in the anti–LAG-3 or anti–ILT4 combination arms
- The safety profiles of all regimens were manageable and consistent with the previous analysis
- Orthogonal inhibition of angiogenesis with a HIF-2α and VEGFR-TKI represents a promising treatment strategy in previously treated advanced clear cell RCC
Presented by: Laurence Albiges, MD, PhD, Medical Oncologist, Gustave Roussy Cancer Campus, University of Paris Sud, Paris, France