(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Toni K. Choueiri discussing the results from ARC-20 assessing the activity and biomarker analyses with casdatifan, a next-generation HIF-2α inhibitor, in refractory clear cell RCC. HIF-2α is a validated target in refractory clear cell RCC, fewer than 25% of patients with previously treated clear cell RCC respond to single agent belzutifan. ARC-20 is an open-label platform study evaluating casdatifan, a HIF-2α inhibitor, in metastatic clear cell RCC with prior anti–PD-(L)1 and VEGFR-TKI treatment. Casdatifan elicits deep and enduring reductions in serum erythropoietin. However, the approved HIF-2α inhibitor loses its effect on serum erythropoietin reduction after approximately 13 weeks.1 At ASCO GU 2026, Dr. Choueiri and colleagues presented updated efficacy with progression free survival, safety, and exploratory biomarker findings including the relationship between serum erythropoietin changes and clinical outcomes.
Data are reported from casdatifan monotherapy expansion cohorts from the phase 1 ARC-20 study (NCT05536141): casdatifan 100 mg daily and a total group comprising all monotherapy cohorts (50 mg daily, 50 mg BID, 100 mg daily, 150 mg daily):

The primary endpoint was safety, and the secondary endpoint was objective response rate. Progression free survival was an exploratory endpoint, and change in serum erythropoietin was assessed and correlated with efficacy.
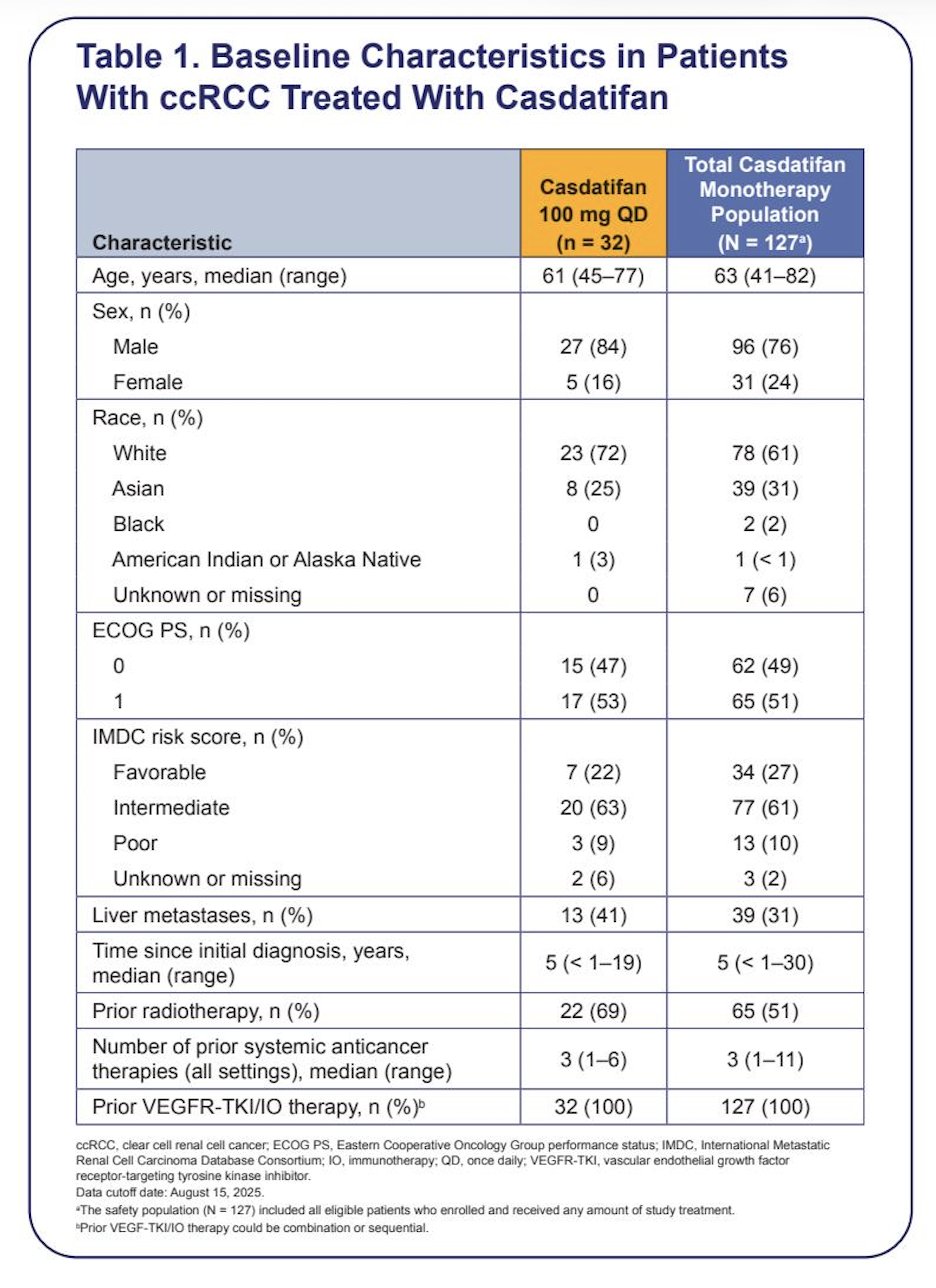
As of August 15, 2025, the median follow-up was 12.4 (range: 6.3–13.5) months (100 mg daily; n=32) and 15 (range: 6–26) months (all patients; n = 127). At baseline, 72% (100 mg daily) and 71% (all patients) had intermediate/poor IMDC risk score, and all patients received prior IO/VEGFR-TKI therapy (median 3 prior lines; range: 1–6 [100 mg daily], 1–11 [all patients]):
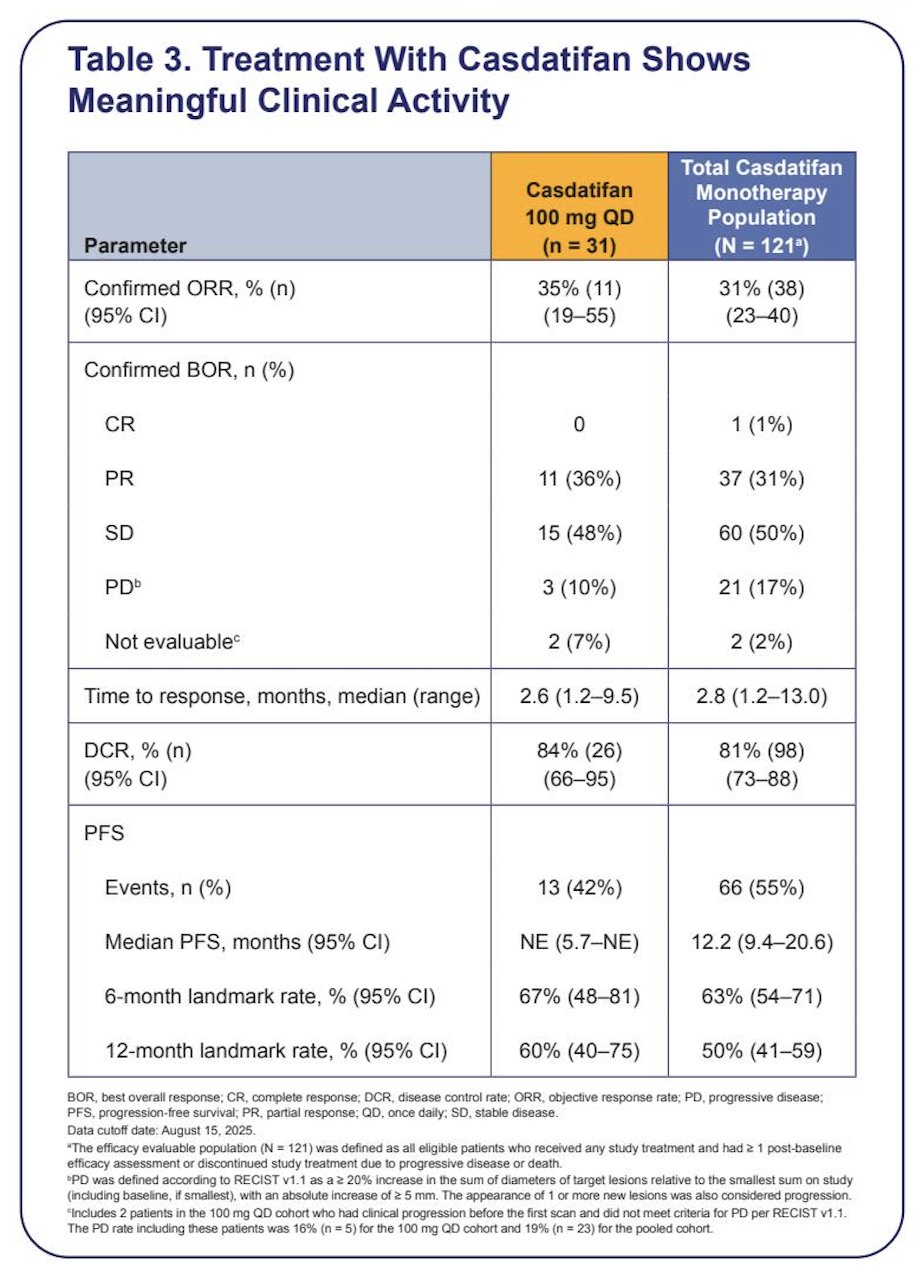
The confirmed objective response rate was 35% (95% CI 19, 55) in the 100 mg daily cohort (all partial responses) and 31% (95% CI 23, 40) in all patients (1 complete response, 37 partial responses). The median progression free survival was not reached (95% CI 5.7 months, not evaluable) and 12.2 (95% CI 9.4, 20.6) months, respectively:
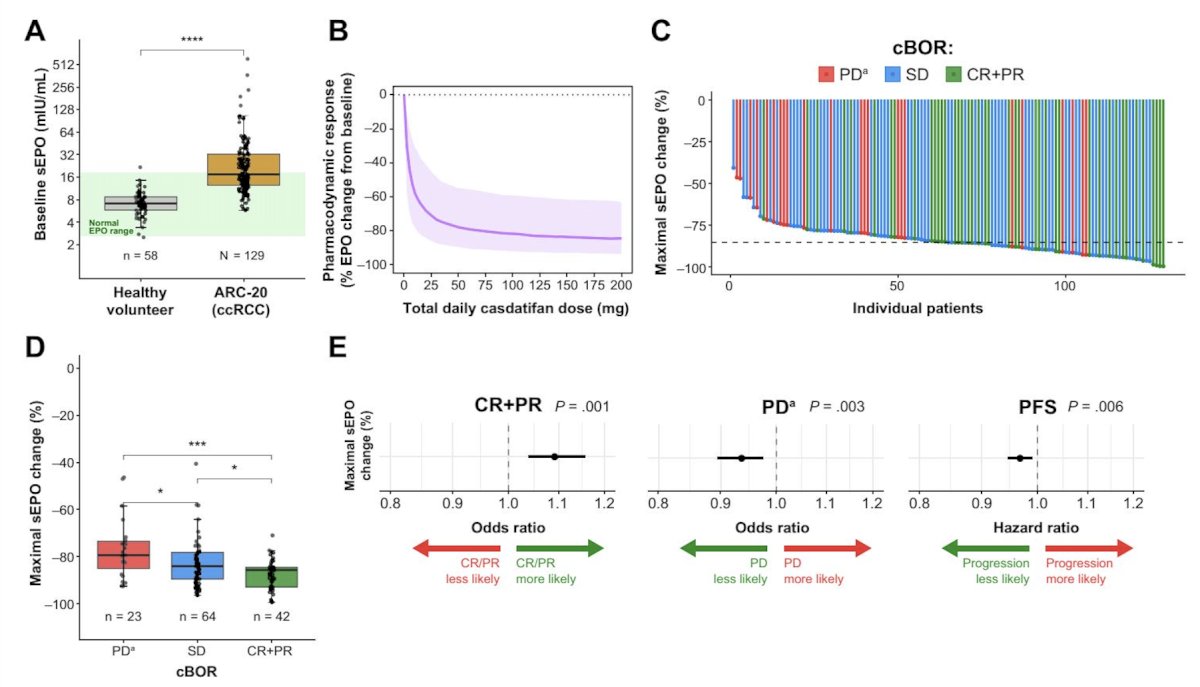
Deep serum erythropoietin reduction was observed by study week 2 and sustained through study week 52. Deeper serum erythropoietin reduction was associated with higher rates of complete response/partial response and lower rates of progressive disease. Additionally, serum erythropoietin reduction was significantly greater in those with disease control (complete response, partial response, stable disease) versus those without (p = .0018), with a median best reduction of 86% versus 79%:
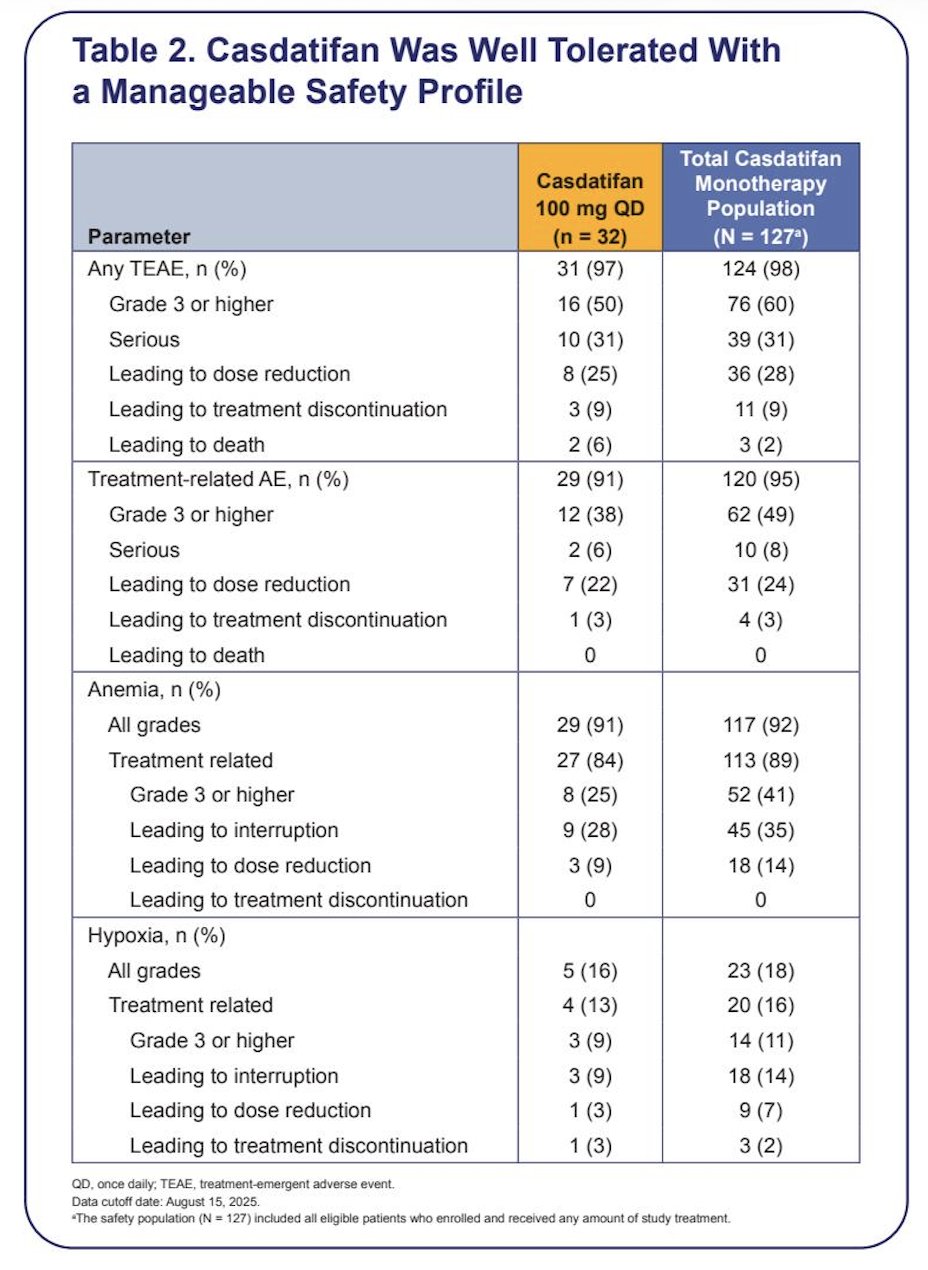
Dose reductions due to casdatifan-related treatment emergent adverse events occurred in 22% (100 mg daily) and 24% (all patients). Most dose reductions were due to anemia (9% [100 mg daily] and 14% [all patients]) and hypoxia (3% [100 mg daily] and 7% [all patients]). Treatment discontinuation due to casdatifan-related treatment emergent adverse events was infrequent in the 100 mg daily cohort (3%) and in all patients (3%), with no patients in the 100 mg daily cohort discontinued due to anemia despite deep erythropoietin suppression. No treatment-related deaths occurred:
Dr. Choueiri concluded his presentation discussing the results from ARC-20 with the following take-home points:
- Casdatifan achieved meaningful and durable responses with a manageable safety profile in a heavily pretreated metastatic ccRCC population, supporting evaluation of the 100 mg QD dose in the ongoing phase 3 PEAK-1 study (NCT07011719)
- The magnitude and durability of serum erythropoietin suppression paralleled clinical benefit, thereby linking a mechanistically precise pharmacodynamic marker to antitumor efficacy
- These data provide a translational framework linking on-target pharmacodynamic modulation, tumor HIF-2α biology, and clinical outcomes
Presented by: Toni K. Choueiri, MD, Dana Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References: