(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a discussant presentation by Dr. Jonathan L. Wright, discussing two abstracts, “ctDNA to guide response-adapted bladder preservation in MIBC: Integrated analysis of the RETAIN trials” by Dr. Pooja Ghatalia and “ctDNA-guided adjuvant atezolizumab in MIBC: Exploratory analysis of ctDNA dynamics in the IMvigor011 trial” by Dr. Thomas Powles. To start his discussion, Dr. Wright emphasized that he will highlight two practical principles for ctDNA:
- ctDNA is systemic (a metastatic risk signal)
- ctDNA is not binary – serial kinetics matter more than a single time point
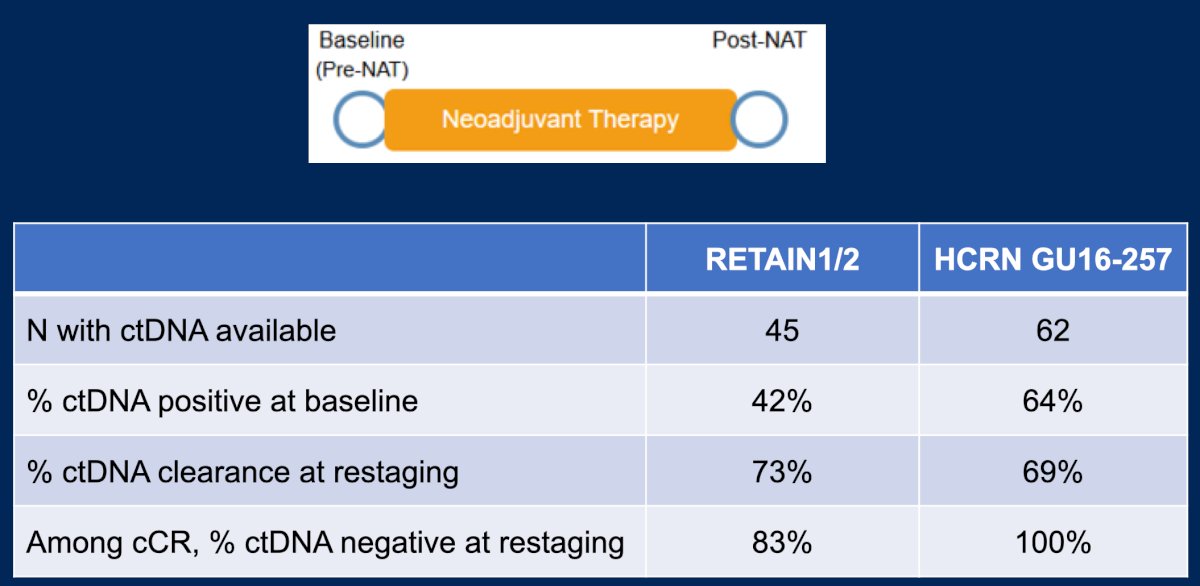
First, Dr. Wright discussed the integrated analysis of the RETAIN trials. With more data, we are learning behavior of ctDNA around neoadjuvant therapy. In the HCRN GU16-257 trial, patients were treated with gemcitabine + cisplatin + nivolumab, which is similar to the MVAC regimen + nivolumab in RETAIN. HRCN GU16-257 taught us that (i) ctDNA is commonly detectable pre-treatment, (ii) a substantial ctDNA fraction clears with therapy, and (iii) the majority of patients with a complete clinical response have negative ctDNA after finishing therapy. Dr. Wright emphasized that the key point is that ctDNA dynamics (detection → clearance) are measurable in real time and can be incorporated into adaptive strategies:
A key take home message from the RETAIN-1/2 analysis is that ctDNA after neoadjuvant therapy identifies metastatic risk. For ctDNA negative patients at restaging, there are excellent 2 year metastasis free survival outcomes of 85% in active surveillance patients, which is similar to ctDNA negative cystectomy patients. For ctDNA positive patients at restaging, there is a high risk of metastatic disease, with 70% developing metastasis within 1 year, despite radical cystectomy:

Thus, ctDNA positivity after neoadjuvant therapy may require systemic intensification rather than local consolidation.
A second key take home message from RETAIN-1/2 is that ctDNA does not reliably monitor the bladder compartment. In this analysis, 52% of patients developed local recurrence, with <10% of patients being ctDNA positive. Of note, all metastatic events were preceded by local recurrence. Thus, cystoscopy and imaging are required for bladder surveillance, and there is a question whether urine tumor DNA can fill the bladder compartment gap. Dr. Wright notes that we have to be cautious with urine tumor DNA. Based on several reports, we know that the same oncogenic mutations driving bladder cancer occur in the normal bladder at increasing frequency with aging:
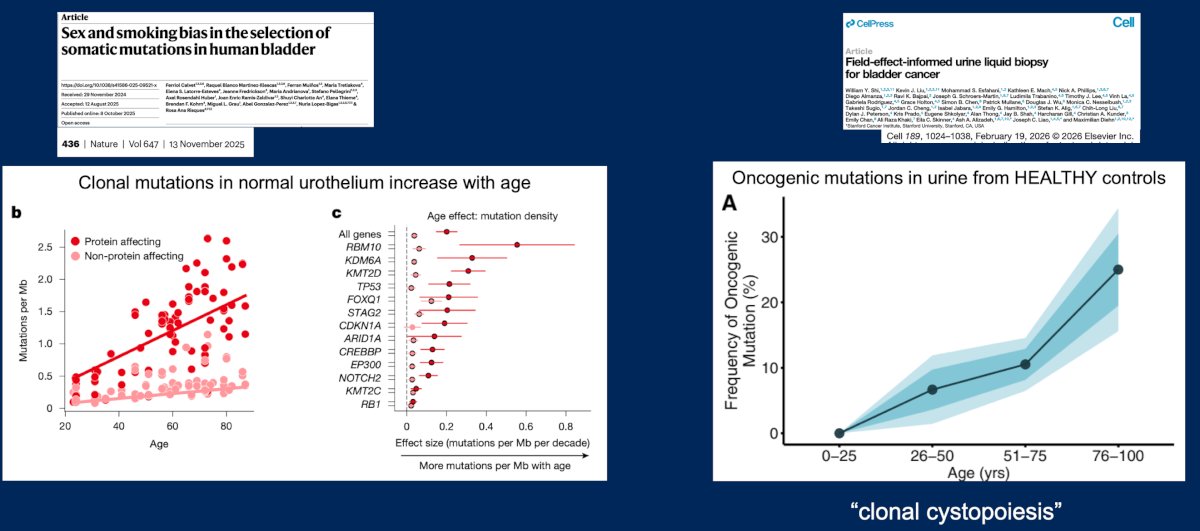
The practical implication is that urine-based assays will have to account for this field-effect biology, ie. “clonal cystopoiesis”. In HCRN GU16-257, urine tumor DNA was collected after neoadjuvant therapy with the hypothesis that among clinical complete response patients, urine tumor DNA may stratify bladder intact outcomes and anticipate earlier recurrence. Dr. Wright states that this evaluation may be promising, but urine tumor DNA needs more research, and the time for additional studies in the clinical complete response space is now.
Dr. Wright then discussed the exploratory analysis of ctDNA dynamics in the IMvigor011 trial. Based on previous work from the IMvigor011 trial led by Dr. Powles, ctDNA-guided adjuvant therapy improves outcomes post-radical cystectomy [1]:
- ctDNA positive patients should consider early adjuvant treatment
- ctDNA negative patients should be spared unnecessary therapy
Importantly, molecular relapse precedes clinical relapse.
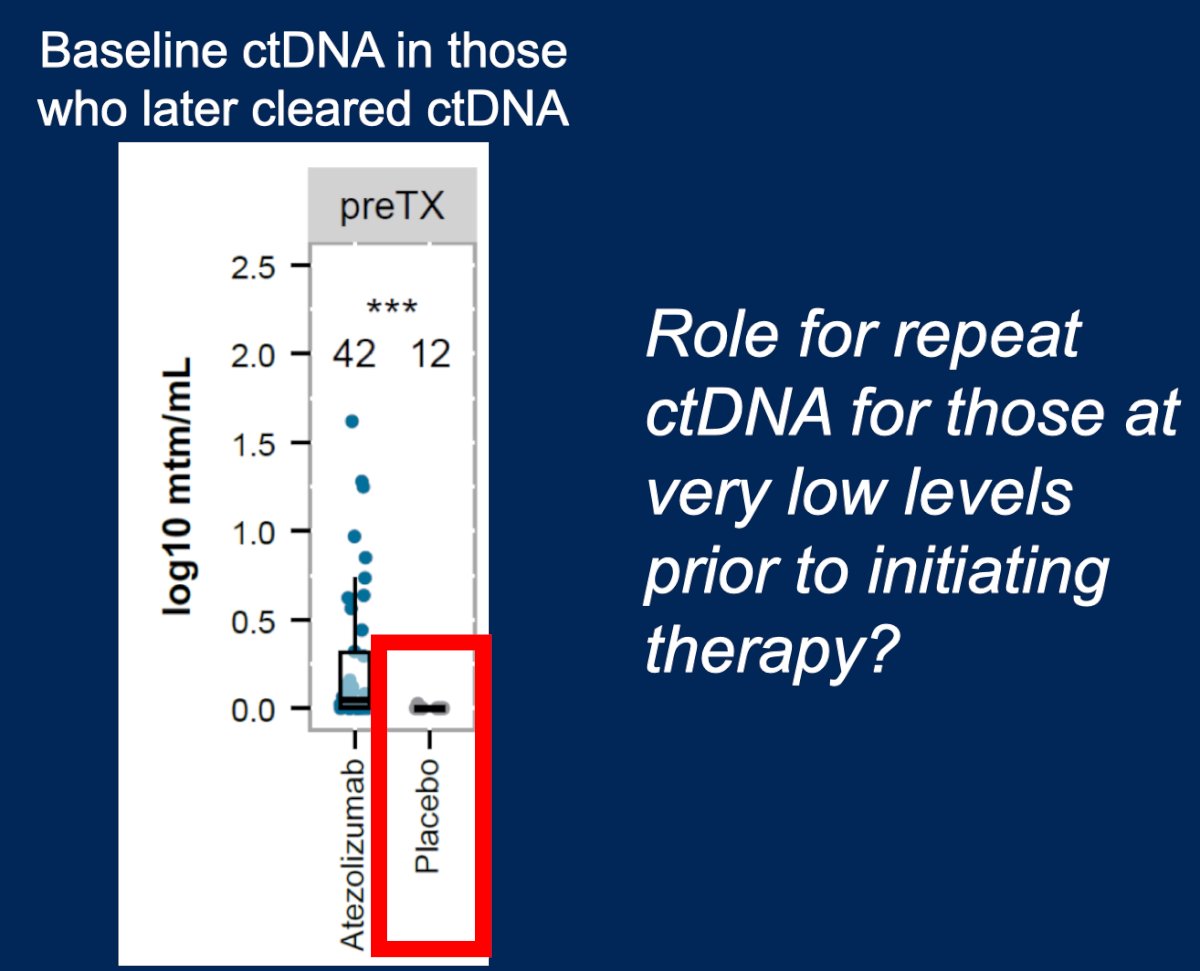
Based on the data presented at ASCO GU 2026, we now know that ctDNA is not binary. Higher ctDNA concentrations and early ctDNA positivity are associated with worse outcomes, and ctDNA clearance is associated with improved outcomes. Dr. Wright notes that another interesting observation with serial ctDNA testing comes from the placebo arm. Among this population, ~20% cleared ctDNA without treatment, which was associated with favorable outcomes. He notes that stochastic fluctuations near the assay detection threshold is the most likely explanation for this phenomenon. Thus, repeat testing may be clinically meaningful before initiating therapy—particularly if the next sample clarifies a rising versus clearing trajectory:
Moreover, in the placebo arm, ~40% of patients who converted to a negative ctDNA still ultimately developed metastasis. The reasons for this may include low-shedding tumors, an assay marker selection that misses the metastatic clone, and primary versus metastatic genomic dominance. Dr. Wright states that there are still unresolved clinical question for ctDNA:
- Clinical implication: testing frequency and surveillance de-escalation
- Operational: EMR integration, access/equity, and cost
Dr. Wright concluded his discussant presentation with the following take-home points:
- ctDNA identifies systemic risk with high precision
- The bladder compartment requires a separate assessment
- Serial ctDNA testing is informative
Presented by: Jonathan L. Wright, MD, MS, FACS, University of Washington, Seattle, WA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
References: