(UroToday.com) At the 2026 ASCO Genitourinary Cancers Symposium, Dr. Félix Guerrero-Ramos presented the “against” perspective in a debate examining whether Bacillus Calmette-Guérin (BCG) should be combined with immune checkpoint inhibitors (ICIs) for patients with high-risk non-muscle-invasive bladder cancer (HR-NMIBC). The central argument was that contemporary BCG therapy already provides excellent long-term outcomes, while the addition of systemic immunotherapy confers only modest incremental benefit at the cost of increased toxicity, complexity, and cost.
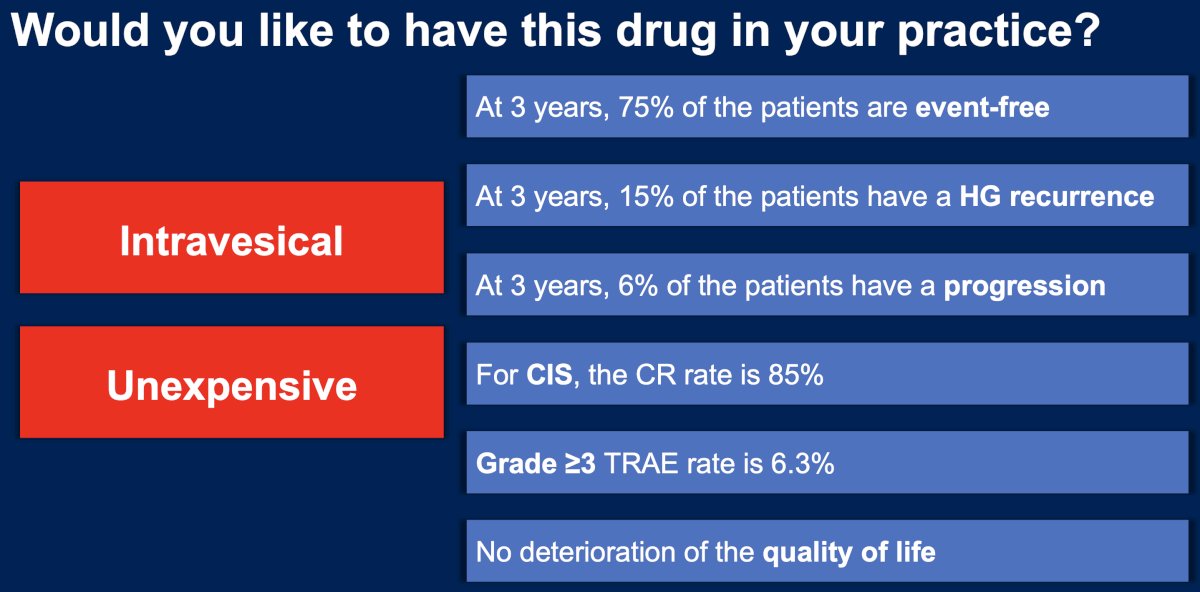
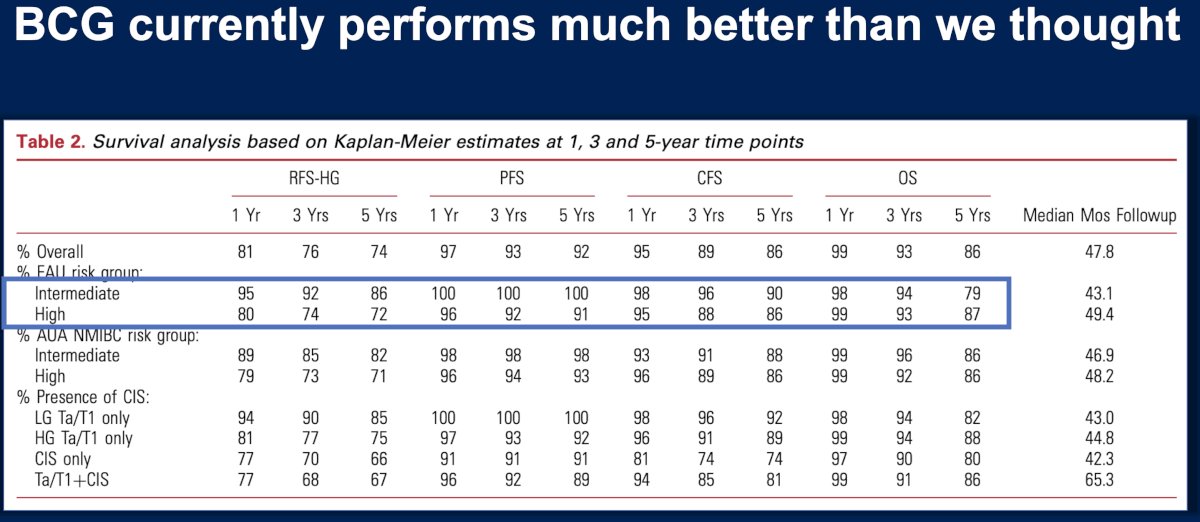
BCG remains the historical and current standard of care for HR-NMIBC. Long-term outcomes reported in contemporary trials demonstrate strong oncologic efficacy with acceptable toxicity. In particular, modern studies of optimized BCG schedules report grade ≥3 treatment-related adverse events (TRAEs) of approximately 6.3%, with durable disease control observed in long-term follow-up. At three years, approximately 75% of patients remain event-free, 15% experience high-grade recurrence, and 6% progress to more advanced disease. Among patients with carcinoma in situ (CIS), complete response rates approach 85%, with no deterioration in quality of life reported. These data highlight the strong efficacy and tolerability of intravesical BCG therapy, which also remains relatively inexpensive and widely accessible.1
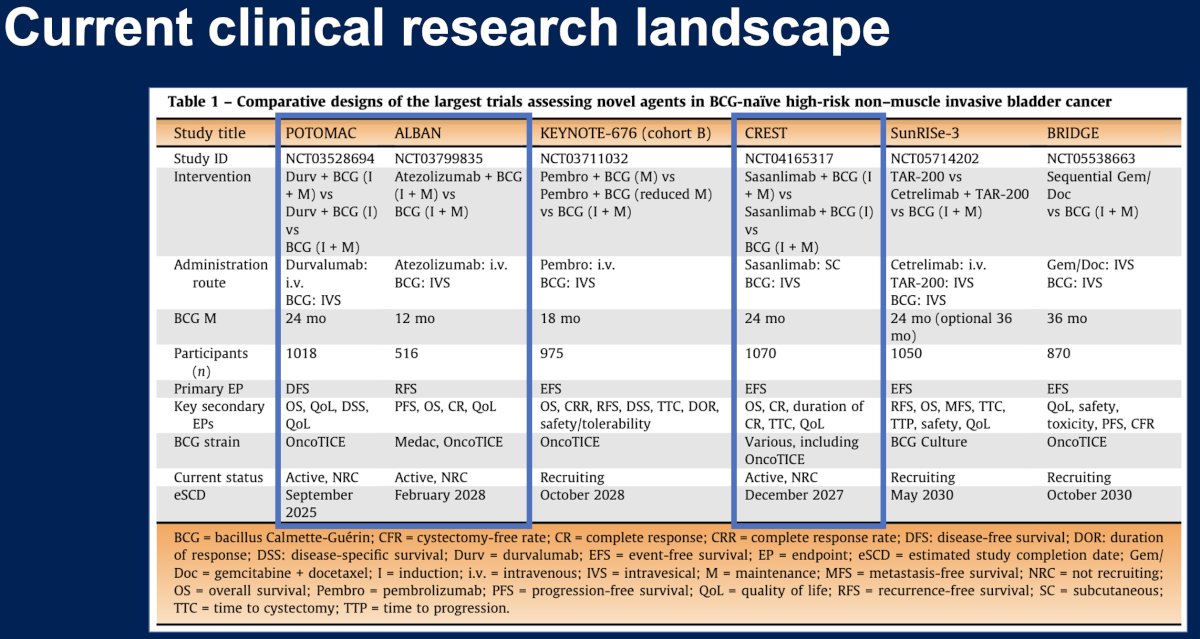
Dr. Guerrero-Ramos next reviewed the contemporary clinical research landscape, evaluating combinations of BCG with systemic immune checkpoint inhibitors.2 These studies seek to improve outcomes by leveraging immune modulation; however, the incremental benefit observed to date appears modest.
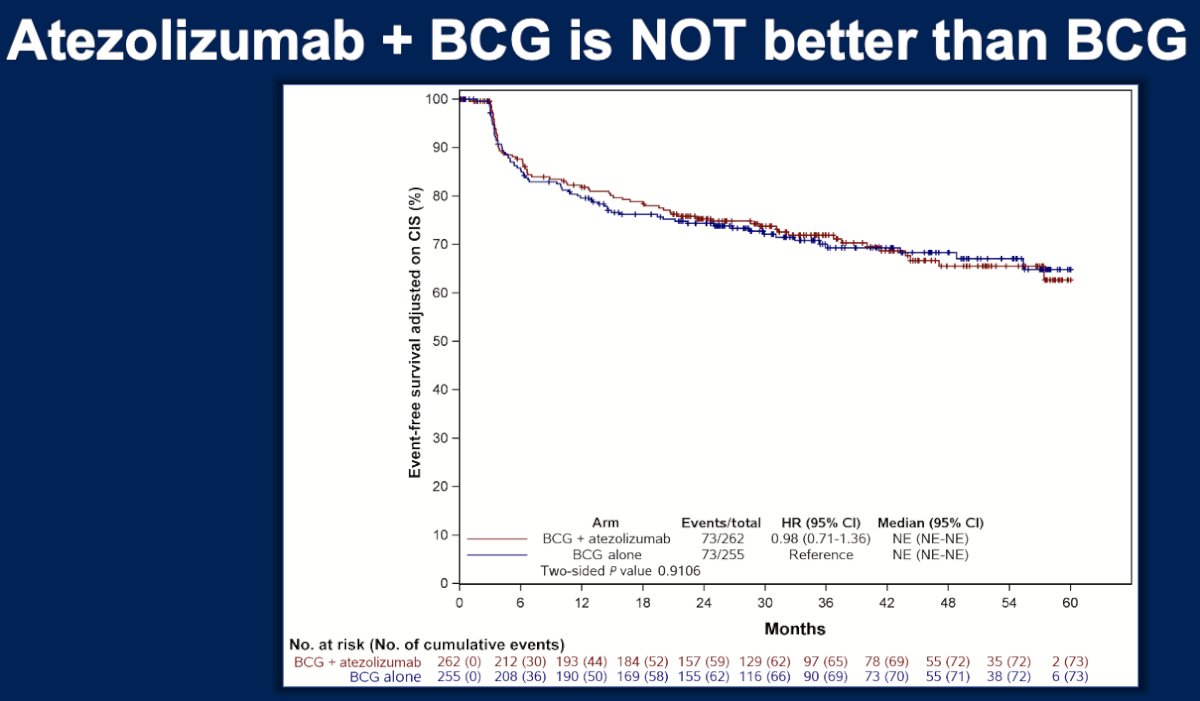
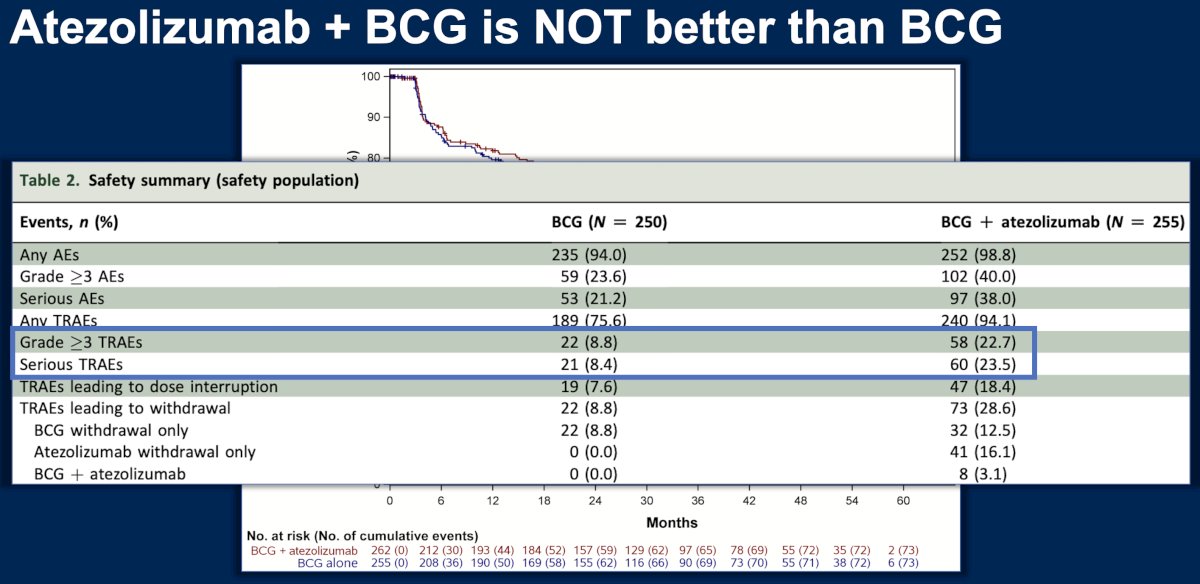
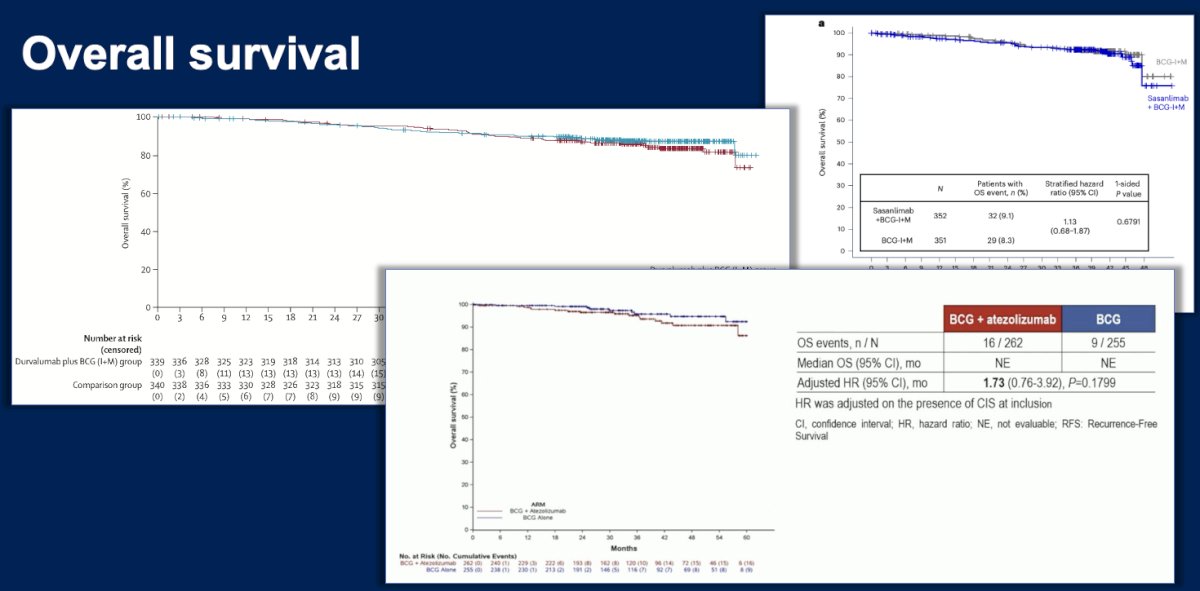
The ALBAN trial evaluated the combination of atezolizumab with BCG. Results presented by Rouprêt and colleagues demonstrated that atezolizumab plus BCG was not superior to BCG alone in HR-NMIBC (EFS HR: 0.98, 95% CI: 0.71–1.36), highlighting that the addition of systemic immunotherapy does not necessarily translate into improved clinical outcomes in this disease state. Furthermore, grade ≥3 (22.7% versus 8.8%) and serious treatment-related adverse events (23.5% versus 8.4%) were more common with BCG + atezolizumab.3
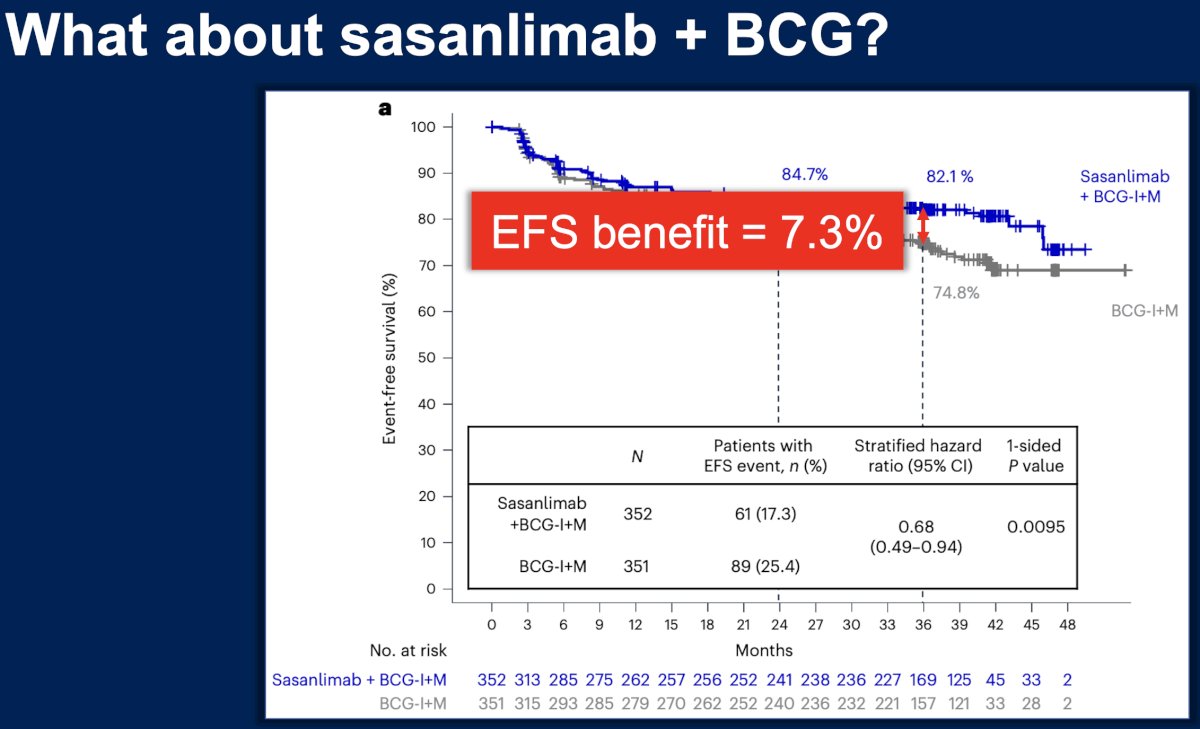
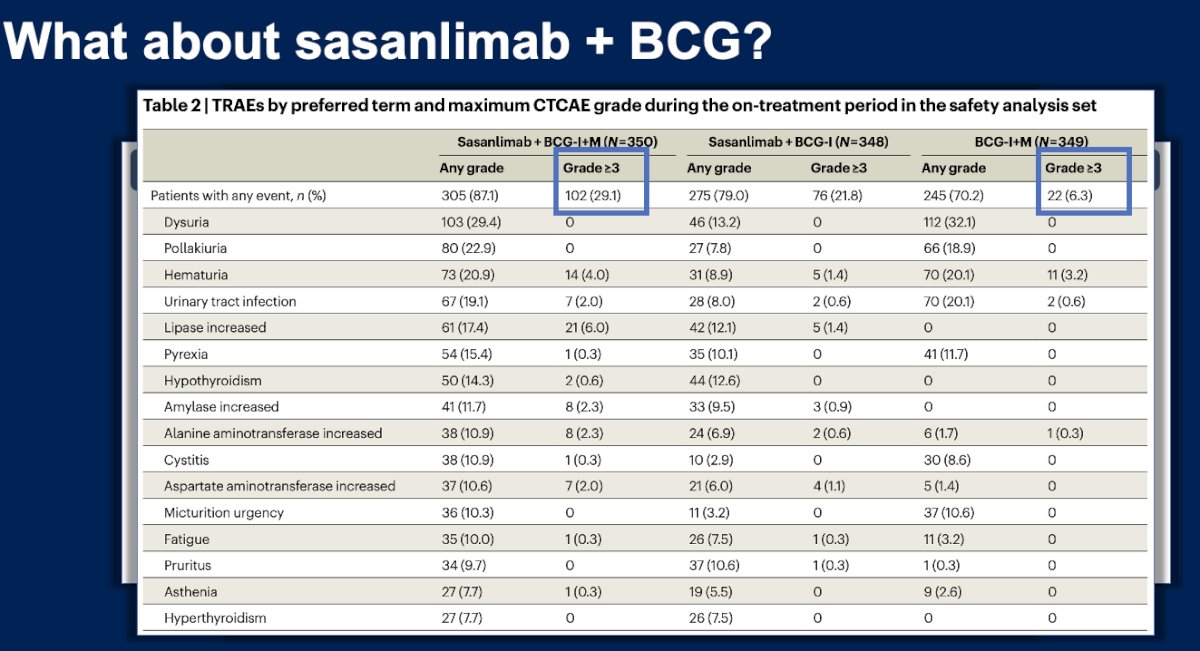
The CREST trial evaluated the PD-1 inhibitor sasanlimab in combination with BCG. In this randomized trial reported by Shore and colleagues, the addition of sasanlimab resulted in an event-free survival (EFS) benefit of approximately 7.3%.4 Although this represented a statistically significant improvement, the absolute magnitude of benefit was relatively modest.
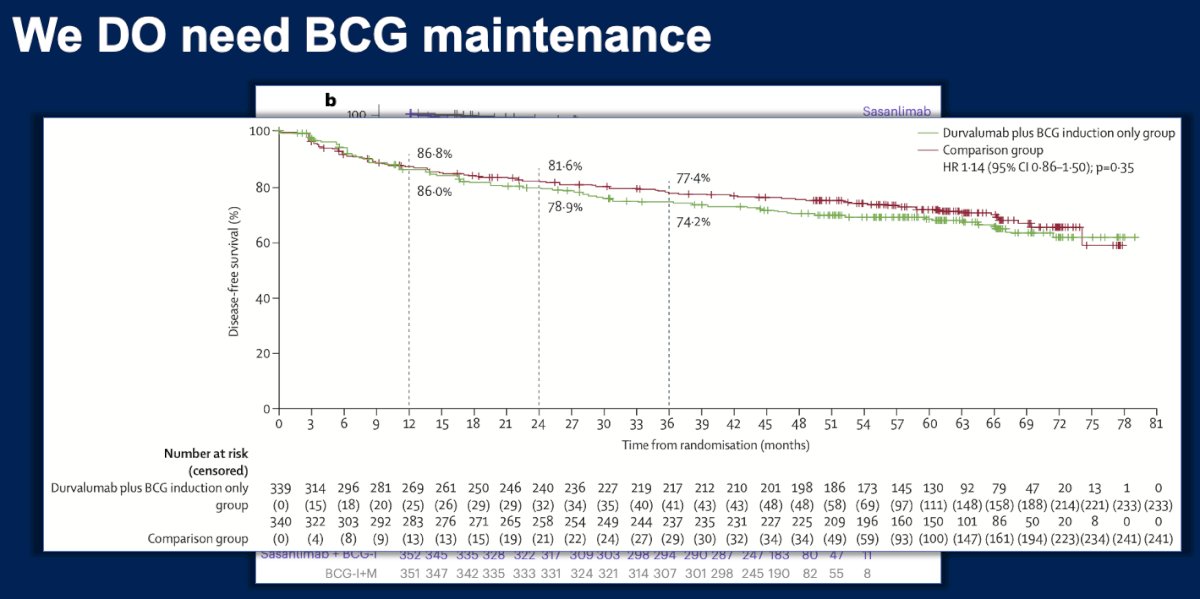
Similarly, the addition of durvalumab to BCG has been evaluated in POTOMAC, reported by De Santis and colleagues. This trial demonstrated a disease-free survival (DFS) benefit of approximately 4.4%, again indicating only a modest improvement with combination therapy.
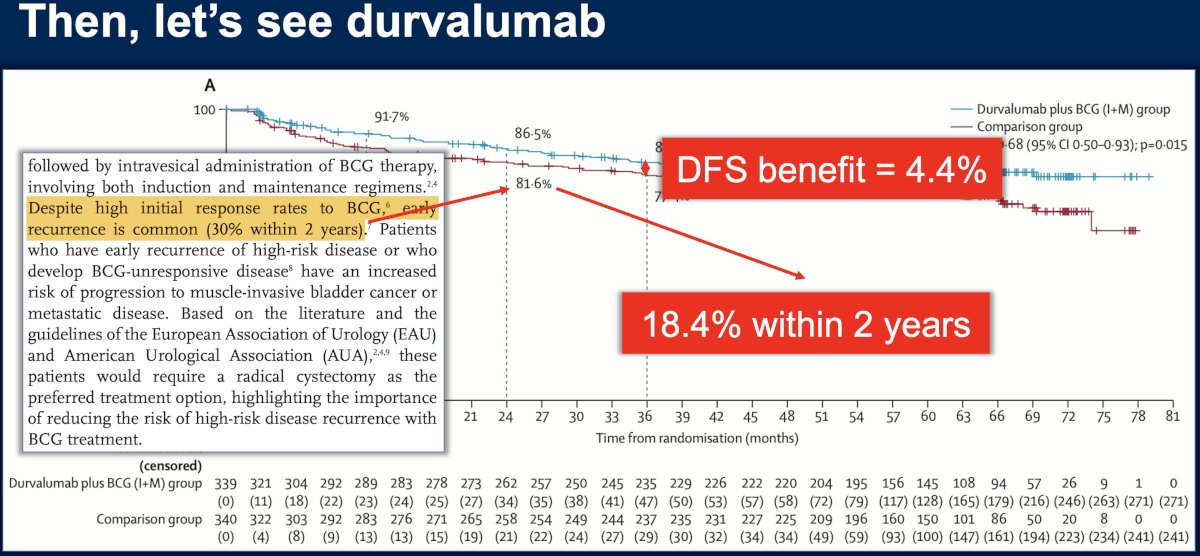
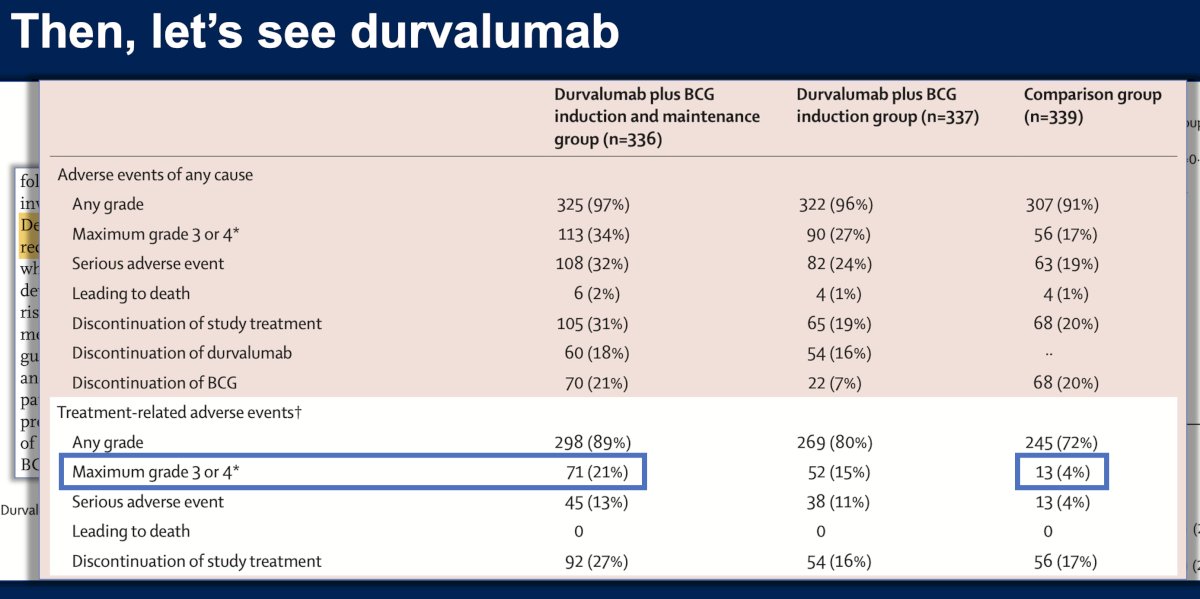
Similar to the other trials, grade 3 or 3 adverse events were more frequent in the combination group (21% versus 4%).5
Taken together, these studies illustrate a consistent pattern: while BCG plus immune checkpoint inhibition may improve certain disease control endpoints, the magnitude of benefit is relatively small, at the cost of increased severe adverse events. In many cases, the primary effect appears to be reduction in high-grade recurrences rather than prevention of disease progression.
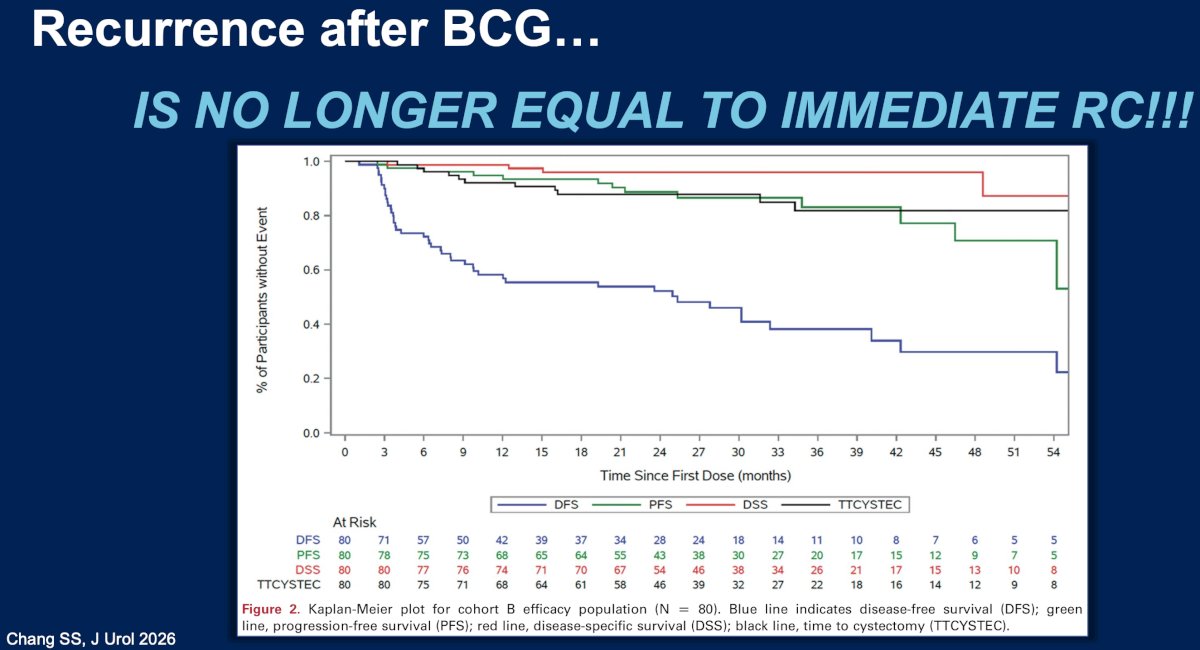
Dr. Guerrero-Ramos then highlighted an important paradigm shift in the management of patients who recur after BCG therapy. Historically, recurrence after BCG often prompted immediate radical cystectomy. However, contemporary management strategies increasingly incorporate bladder-preserving options, particularly for BCG-unresponsive disease.6
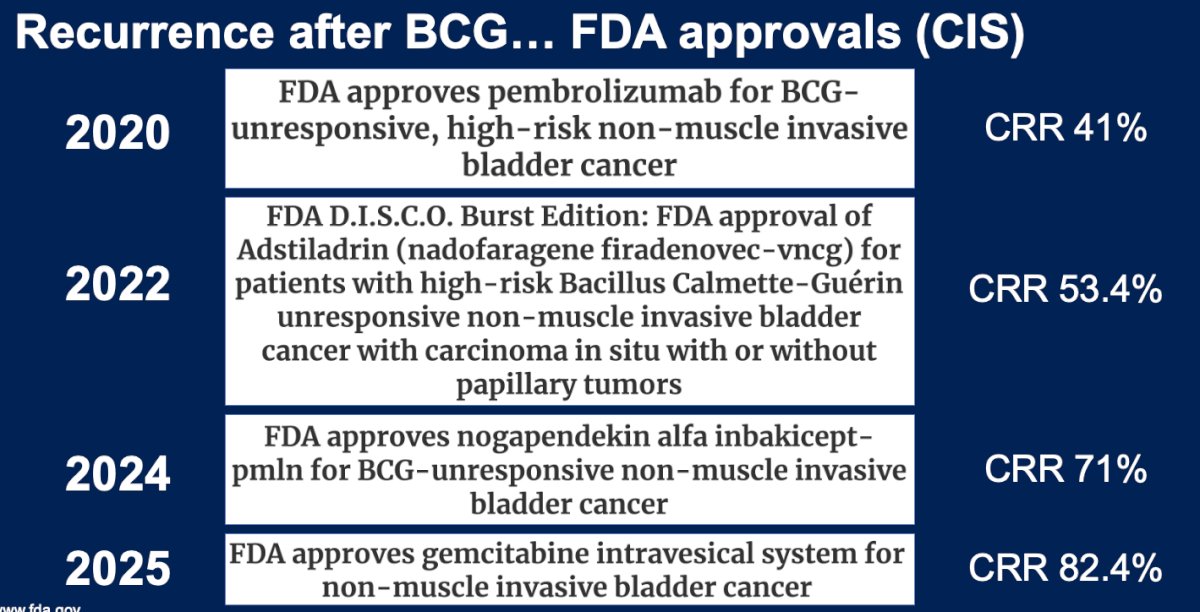
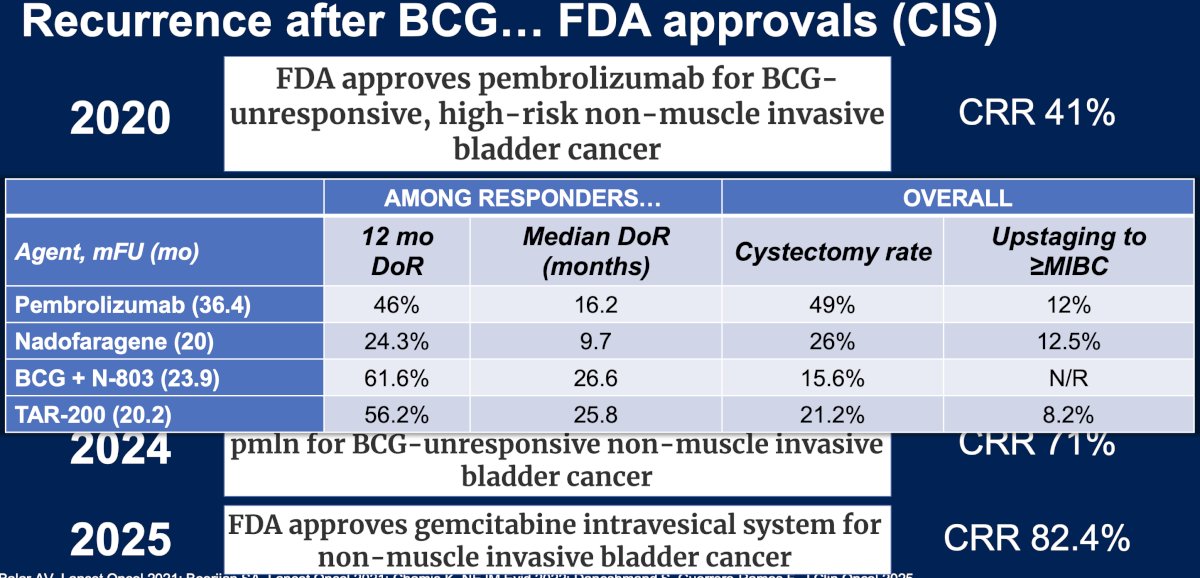
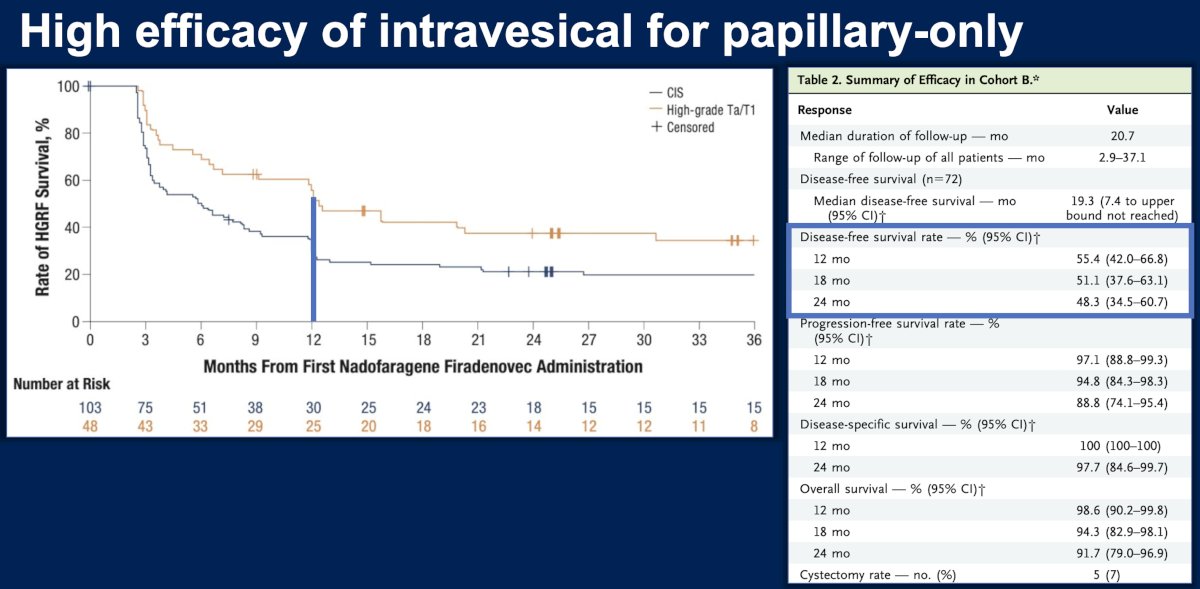
Several intravesical and systemic therapies have now received regulatory approval in this setting. These include pembrolizumab, nadofaragene firadenovec, N-803 plus BCG, and the gemcitabine-releasing intravesical device TAR-200. Reported complete response rates across these agents range from approximately 41% to 82%, depending on the therapy and study population.7-10
Among responders, durable disease control has been observed with encouraging long-term outcomes. For example, pembrolizumab achieved a 12-month duration of response rate of approximately 46% with a median duration of response of 16.2 months. Nadofaragene firadenovec demonstrated a median duration of response of 9.7 months, while N-803 plus BCG achieved a 12-month duration of response rate exceeding 60%. TAR-200 similarly demonstrated durable responses with a median duration of response approaching 26 months.8-10
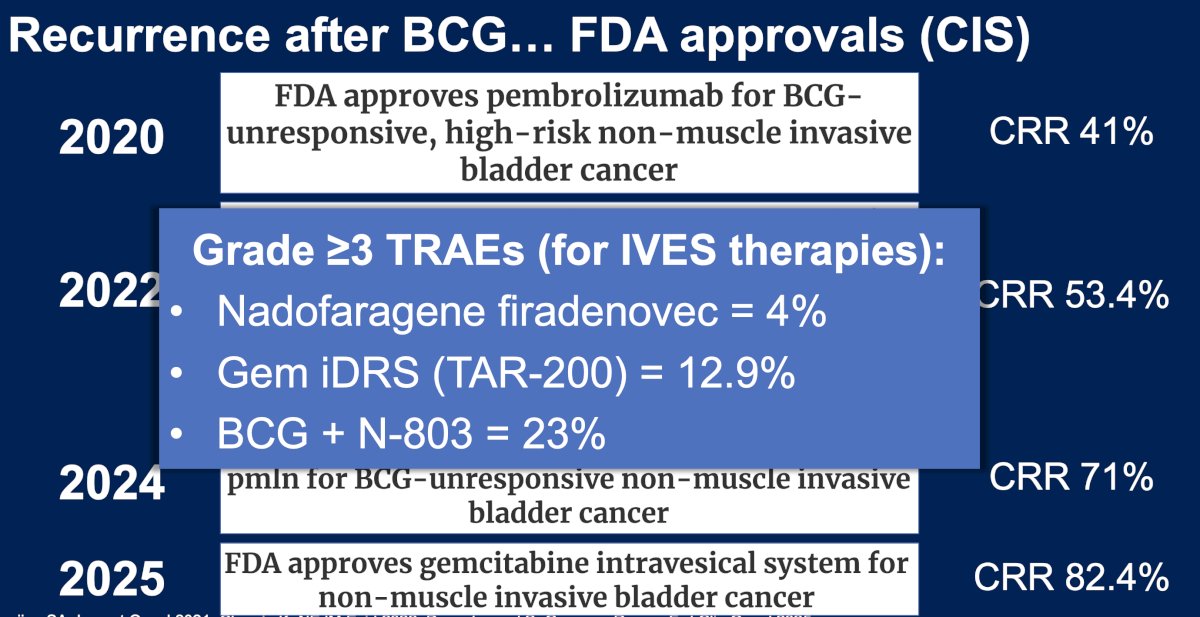
Importantly, the safety profiles of these therapies remain favorable. Rates of grade ≥3 TRAEs are approximately 4% with nadofaragene firadenovec, approximately 12.9% with TAR-200, and approximately 23% with N-803 plus BCG.9,10 These results suggest that effective bladder-preserving salvage therapies are available for patients who recur after BCG, further reducing the urgency to escalate treatment earlier in the disease course.
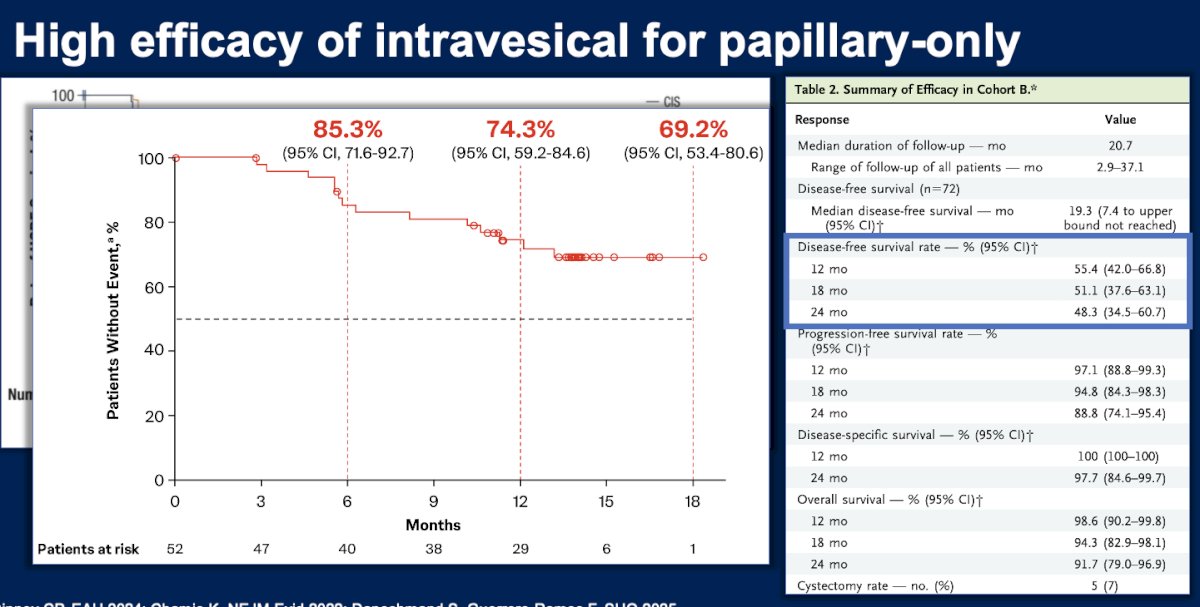
Dr. Guerrero-Ramos also highlighted that intravesical therapies demonstrate particularly strong efficacy in patients with papillary-only disease. Data from studies by Dinney and colleagues and Chamie and colleagues support high response rates in these populations, further reinforcing the role of bladder-preserving intravesical approaches in selected patients.11,12
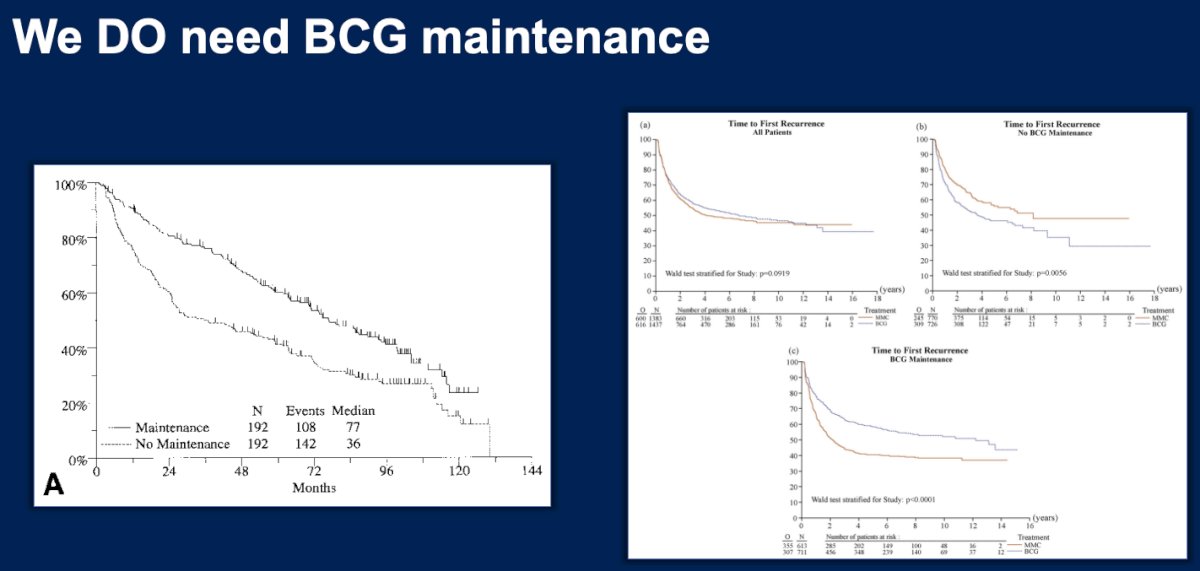
Another key point emphasized was the importance of BCG maintenance therapy. Historical randomized trials conducted by Lamm and colleagues demonstrated that maintenance BCG significantly improves outcomes compared with induction therapy alone.13 Subsequent analyses, including those by Malmström and colleagues, further confirmed the importance of maintenance therapy in optimizing oncologic outcomes.14
Modern observational analyses suggest that outcomes with contemporary BCG therapy may be better than previously appreciated. Matulay and colleagues demonstrated improved recurrence-free survival rates in real-world cohorts treated with optimized BCG protocols.15
When evaluating survival outcomes across modern trials, the addition of immune checkpoint inhibitors to BCG has not yet demonstrated a clear overall survival advantage. This observation further raises questions regarding the clinical value of adding systemic therapy to an already effective intravesical treatment strategy.
Economic considerations also play an important role. Although certain intravesical salvage therapies for BCG-unresponsive disease may have higher individual costs, relatively few patients ultimately require these therapies because most respond to BCG alone. Consequently, the overall cost of a strategy centered on BCG with salvage therapies as needed is likely lower than a universal upfront combination approach incorporating systemic immunotherapy.16
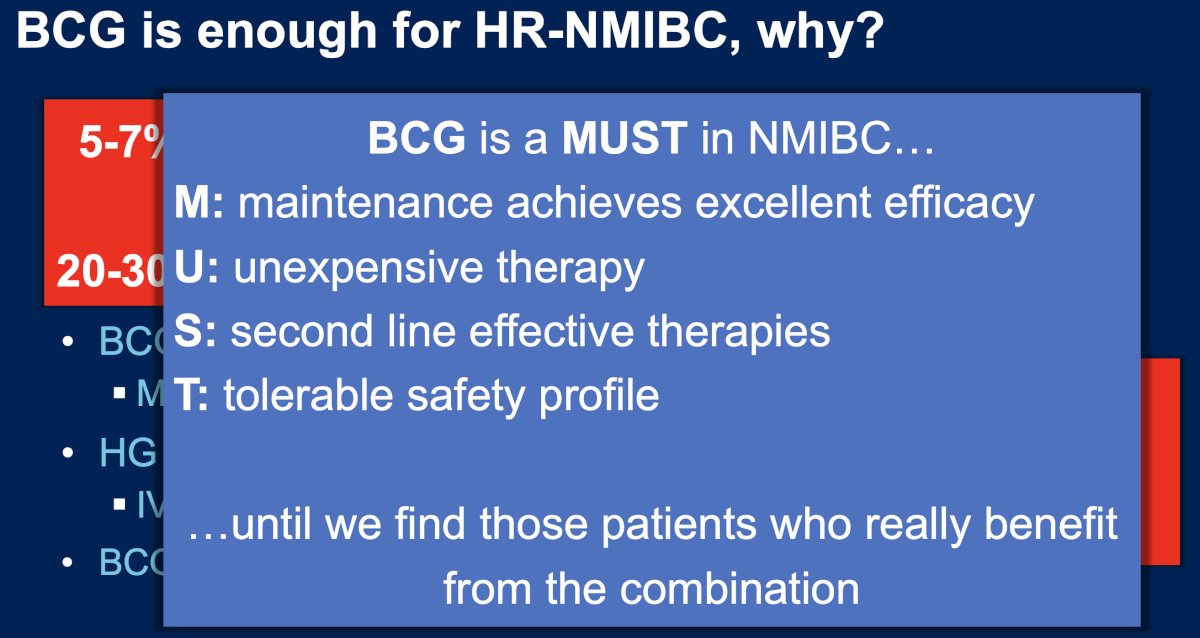
Dr. Guerrero-Ramos summarized the key arguments against routine use of BCG plus immune checkpoint inhibition in HR-NMIBC. First, the efficacy benefits of adding ICIs appears modest, with absolute improvements in EFS or DFS of approximately 5–7%. Second, these modest gains must be weighed against the increased risk of toxicity associated with systemic immunotherapy, where grade ≥3 adverse event rates range from 20–30%.
From a quantitative perspective, the estimated number needed to treat (NNT) to prevent one event is approximately 14–20 patients, whereas the number needed to harm (NNH) is approximately 3–5 patients. This unfavorable balance between benefit and toxicity further supports cautious adoption of combination therapy.
Finally, Dr. Guerrero-Ramos concluded by emphasizing that BCG remains a cornerstone of NMIBC management. He summarized the strengths of BCG using the acronym “MUST”:
M – Maintenance therapy achieves excellent efficacy
U – Unexpensive and widely available therapy
S – Effective second-line treatments exist for recurrence
T – Tolerable safety profile
Accordingly, BCG alone remains sufficient for most patients with HR-NMIBC. The addition of systemic immune checkpoint inhibition should likely be reserved for carefully selected populations once predictive biomarkers are identified that can identify patients most likely to benefit from combination therapy.
Presented by: Felix Guerrero-Ramos, MD, PhD, FEBU, Department of Urology, Hospital Universitario 12 de Octubre, Madrid, Spain
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: Evaluating the Case Against Combining Immune Checkpoint Inhibitors with BCG in Non-Muscle-Invasive Bladder Cancer - Félix Guerrero-Ramos
References:
- Shore ND, Shore N, Shore ND. Intravesical BCG outcomes in high-risk non-muscle-invasive bladder cancer. Nat Med. 2025.
- Guerrero-Ramos F, Guerrero-Ramos F, Guerrero-Ramos F. Current clinical research landscape of BCG plus immunotherapy in non-muscle-invasive bladder cancer. Eur Urol Oncol. 2024.
- Rouprêt M, Rouprêt M, Rouprêt M. Atezolizumab plus bacillus Calmette-Guérin versus bacillus Calmette-Guérin alone in high-risk non-muscle-invasive bladder cancer. Ann Oncol. 2026.
- Shore ND, Shore N, Shore ND. Sasanlimab plus bacillus Calmette-Guérin for high-risk non-muscle-invasive bladder cancer. Nat Med. 2025.
- De Santis M, De Santis M, De Santis M. Durvalumab plus bacillus Calmette-Guérin in high-risk non-muscle-invasive bladder cancer. Lancet. 2025.
- Chang SS, Chang SS, Chang SS. Contemporary management of bacillus Calmette-Guérin recurrence in non-muscle-invasive bladder cancer. J Urol. 2026.
- Balar AV, Kulkarni GS, Uchio EM. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to bacillus Calmette-Guérin. Lancet Oncol. 2021;22:919–930.
- Boorjian SA, Alemozaffar M, Konety BR. Intravesical nadofaragene firadenovec gene therapy for bacillus Calmette-Guérin–unresponsive non-muscle-invasive bladder cancer. Lancet Oncol. 2021;22:107–117.
- Chamie K, Li R, Kader AK. TAR-200 intravesical drug delivery system for non-muscle-invasive bladder cancer: early clinical outcomes. NEJM Evid. 2022;1.
- Daneshmand S, Guerrero-Ramos F, Chamie K. N-803 plus bacillus Calmette-Guérin in bacillus Calmette-Guérin–unresponsive non-muscle-invasive bladder cancer. J Clin Oncol. 2025.
- Dinney CP, Dinney CP, Dinney CP. Intravesical therapy outcomes in papillary non-muscle-invasive bladder cancer. EAU Congress. 2024.
- Chamie K, Li R, Kader AK. Clinical outcomes with intravesical therapies in papillary bladder cancer. NEJM Evid. 2022.
- Lamm DL, Blumenstein BA, Crawford ED. Maintenance bacillus Calmette-Guérin immunotherapy for recurrent Ta, T1 and carcinoma in situ transitional cell carcinoma of the bladder. J Urol. 2000;163:1124–1129.
- Malmström PU, Sylvester RJ, Crawford DE. Long-term outcomes of bacillus Calmette-Guérin therapy for non-muscle-invasive bladder cancer: a meta-analysis of randomized trials. Eur Urol. 2009;56:247–256.
- Matulay JT, Soloway MS, Herr HW. Contemporary outcomes of bacillus Calmette-Guérin therapy for high-risk non-muscle-invasive bladder cancer. J Urol. 2021;205:123–131.
- Bedke J, Guerrero-Ramos F, Bedke J. Economic considerations in intravesical therapy for non-muscle-invasive bladder cancer. Urol Oncol. 2023.