(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a session on integrating emerging evidence into practice for the management of non-muscle invasive bladder cancer (NMIBC) patients. Dr. Noah Hahn presented emerging evidence supporting the integration of immune checkpoint inhibitors (ICI) with intravesical Bacillus Calmette-Guérin (BCG) for the treatment of BCG-naïve high-risk NMIBC (HR-NMIBC). Two central conclusions framed the presentation:
- First, level 1 evidence now supports the addition of immune checkpoint inhibition to intravesical BCG in patients with BCG-naïve HR-NMIBC.
- Second, the addition of ICI to BCG provides meaningful clinical benefit with an acceptable risk profile, particularly among patients with the highest risk of disease progression and metastasis.
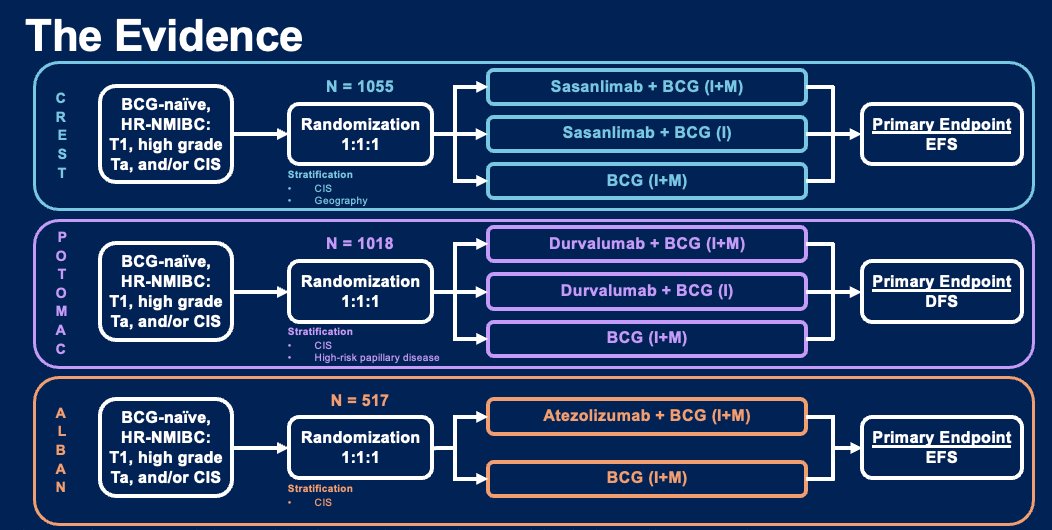
Three large, randomized phase III trials evaluating ICI plus BCG were highlighted: CREST, POTOMAC, and ALBAN.1–4 These trials enrolled patients with BCG-naïve HR-NMIBC, including T1 disease, high-grade Ta tumors, and carcinoma in situ (CIS).
CREST evaluated sasanlimab combined with BCG. Patients were randomized 1:1:1 to:
- Sasanlimab plus BCG induction and maintenance
- Sasanlimab plus BCG induction alone
- BCG induction and maintenance alone
The primary endpoint was event-free survival (EFS), and the study enrolled 1,055 patients.
POTOMAC evaluated durvalumab combined with BCG in a similarly designed randomized 1:1:1 trial with disease-free survival (DFS) as the primary endpoint. This trial enrolled 1,018 patients.
ALBAN evaluated atezolizumab combined with BCG in a randomized trial of 517 patients, with event-free survival as the primary endpoint.
Across these three trials, approximately 2,590 patients were enrolled globally.
Two of the three phase III trials demonstrated statistically significant improvements with the addition of immune checkpoint inhibition.
In the CREST trial, sasanlimab plus BCG induction and maintenance significantly improved event-free survival compared with BCG alone (HR 0.68, 95% CI 0.49–0.94; p=0.0095). This corresponded to an absolute 3-year EFS improvement of 7.3%.3
Similarly, in the POTOMAC trial, durvalumab plus BCG induction and maintenance improved disease-free survival (HR 0.68, 95% CI 0.50–0.93; p=0.0154), corresponding to a 4.4% absolute improvement in 3-year DFS.2
In contrast, the ALBAN trial evaluating atezolizumab plus BCG did not demonstrate an improvement in event-free survival (HR 0.98, 95% CI 0.71–1.36).4
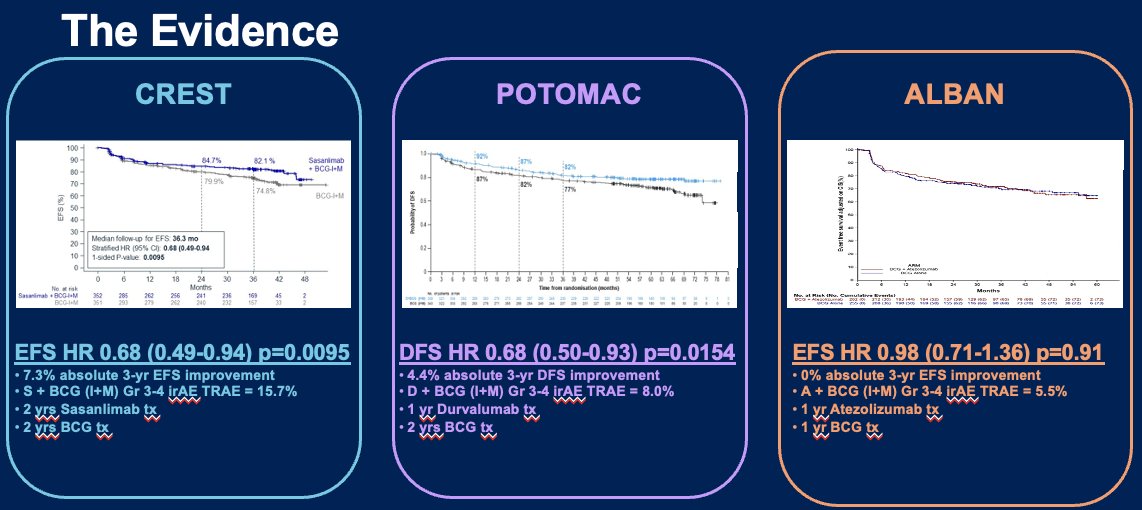
Taken together, these results suggest a modest but consistent improvement in disease-related outcomes with the addition of immune checkpoint inhibition to BCG in BCG-naïve HR-NMIBC, at the cost of increased immune-related adverse events.
Differences in Trial DesignDr. Hahn emphasized that important differences in trial design and patient populations likely explain the discordant results.
CREST and POTOMAC enrolled a “higher-risk” HR-NMIBC population, with approximately 58% of patients presenting with T1 disease. Both trials incorporated adequate BCG induction and maintenance schedules in the control arms.
In contrast, ALBAN enrolled a relatively lower-risk population with only 39% T1 disease and utilized a truncated BCG maintenance schedule. These differences likely contributed to the absence of benefit observed in ALBAN.

Thus, the key clinical question addressed by CREST and POTOMAC—whether the addition of ICI to adequate BCG therapy improves outcomes in higher-risk HR-NMIBC—was answered affirmatively.
Clinical Burden of the Recurrence CycleThe presentation next addressed the clinical burden associated with the “endless recurrence cycle” in HR-NMIBC. Patients frequently undergo repeated cystoscopy, biopsies, and transurethral resections (TURBT) as part of disease monitoring and management following recurrence.
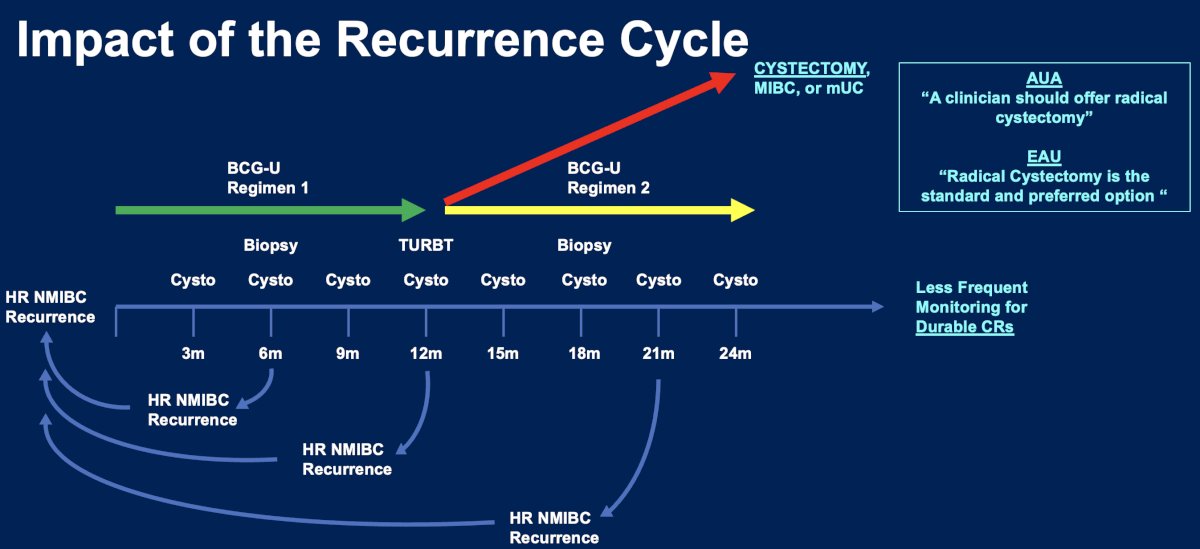
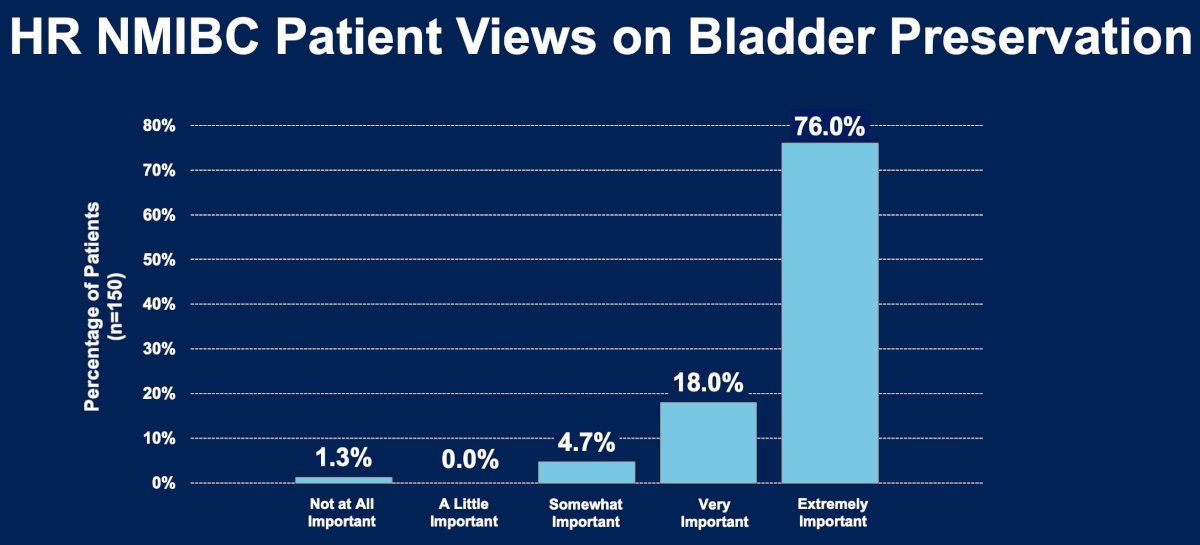
Guidelines from both the American Urological Association and European Association of Urology recommend radical cystectomy for BCG-unresponsive disease.5,6 However, many patients strongly prioritize bladder preservation. A survey of HR-NMIBC patients demonstrated that bladder preservation is considered extremely important by the majority of patients, underscoring the need for effective bladder-sparing strategies.7
Several treatments for BCG-unresponsive NMIBC have been developed, including intravesical gemcitabine-docetaxel, nadofaragene firadenovec, nogapendekin alfa inbakicept (NAI), gemcitabine intravesical systems, and cretostimogene grenadenorepvec.
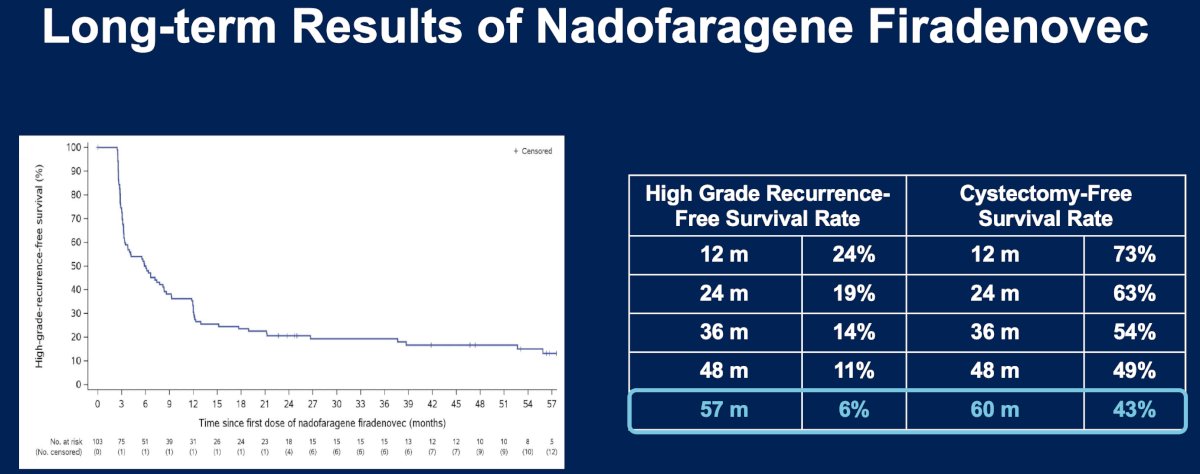
Although initial complete response (CR) rates can be encouraging, these therapies frequently demonstrate declining durability over time. For example, nadofaragene firadenovec demonstrated a CR rate of approximately 53%, but a 12-month CR rate of only 24.3%.8 Long-term follow-up data show that high-grade recurrence-free survival declines progressively, reaching approximately 6% by five years.11
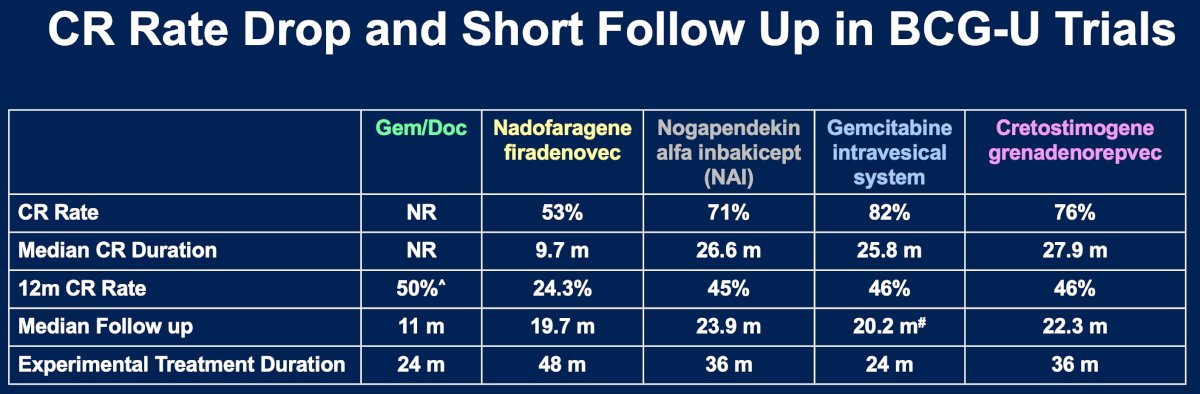
These findings highlight the limited curative potential of currently available bladder-preserving strategies once BCG-unresponsive disease develops.
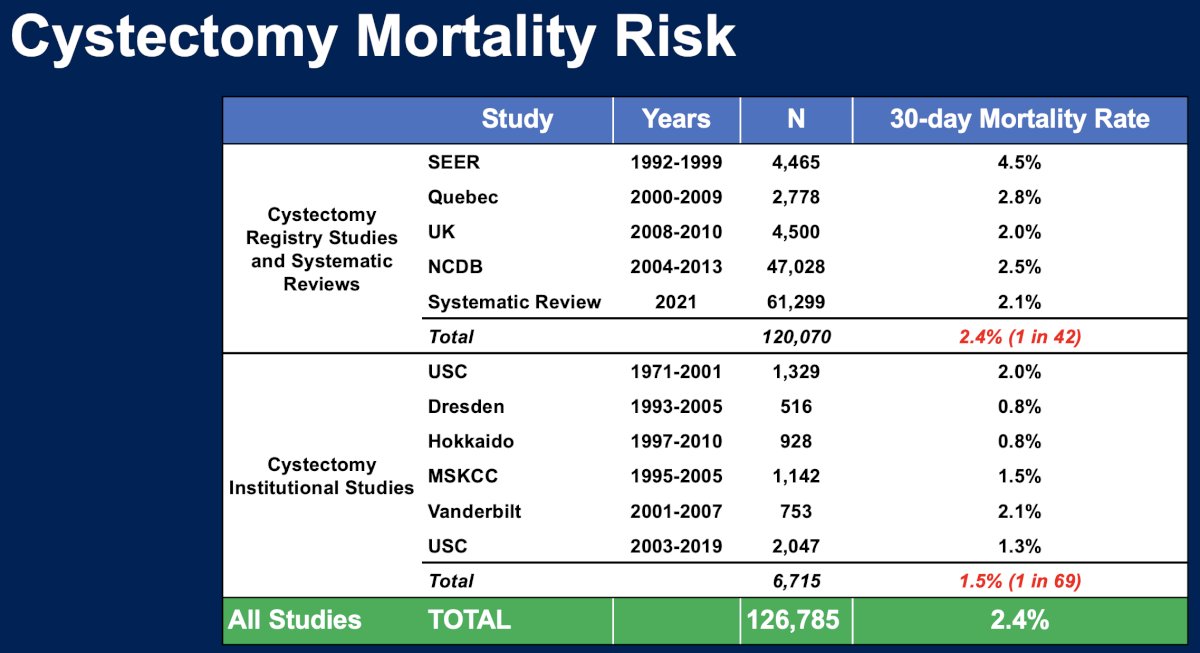
Radical cystectomy remains the gold standard for patients with BCG-unresponsive disease, but it carries meaningful perioperative risks.
Across large registry and systematic review datasets including more than 120,000 patients, the 30-day mortality rate following cystectomy is approximately 2.4%, corresponding to roughly one death per 42 patients.12–16 Institutional series report somewhat lower rates but still demonstrate measurable perioperative risk.
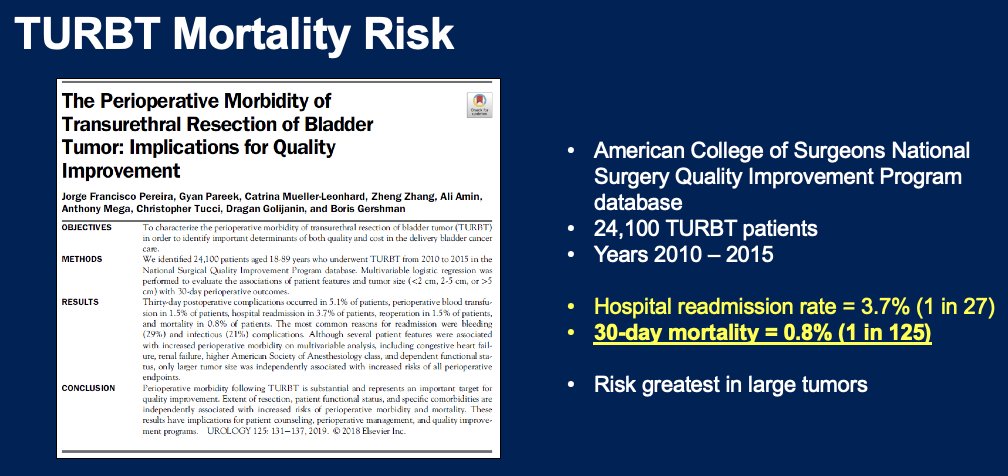
Even transurethral resection procedures carry risk. Analysis of the American College of Surgeons NSQIP database including over 24,000 TURBT procedures demonstrated a 30-day mortality rate of 0.8% and a hospital readmission rate of 3.7%.17
These data emphasize the importance of therapies that can reduce recurrence and delay progression while preserving bladder function.
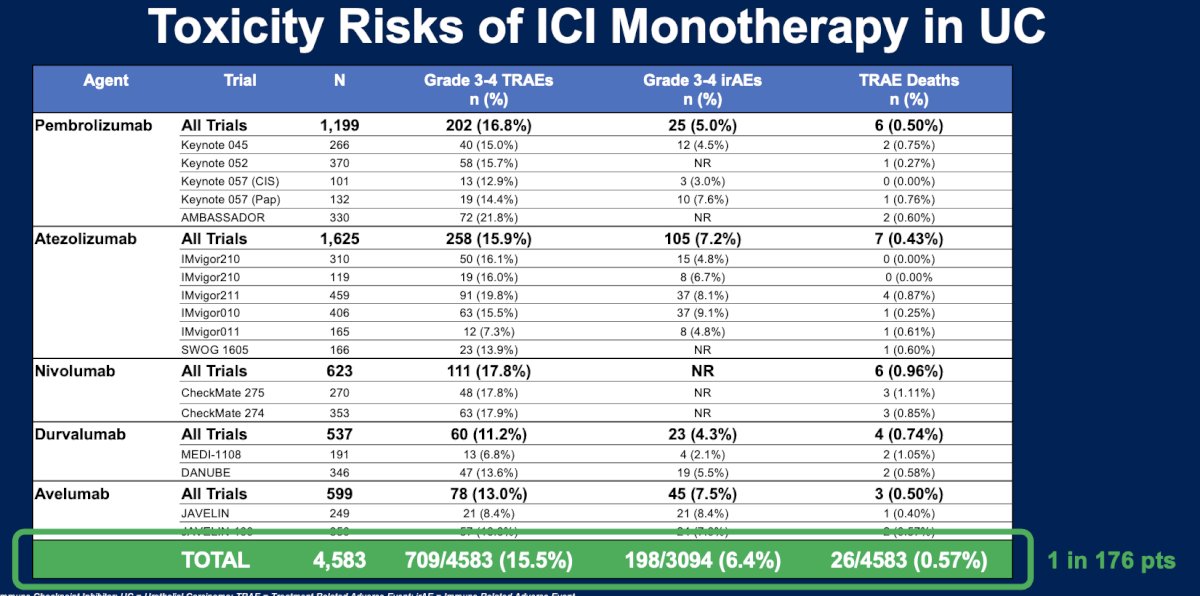
Safety of Immune Checkpoint InhibitorsThe toxicity profile of immune checkpoint inhibitors in urothelial carcinoma has been extensively characterized.
Across multiple trials involving more than 4,500 patients treated with pembrolizumab, atezolizumab, nivolumab, durvalumab, or avelumab, grade 3–4 treatment-related adverse events occurred in approximately 15.5% of patients, and immune-related adverse events occurred in approximately 6.4%. Treatment-related mortality was rare, occurring in roughly 0.57% of patients (approximately 1 in 176).18–22
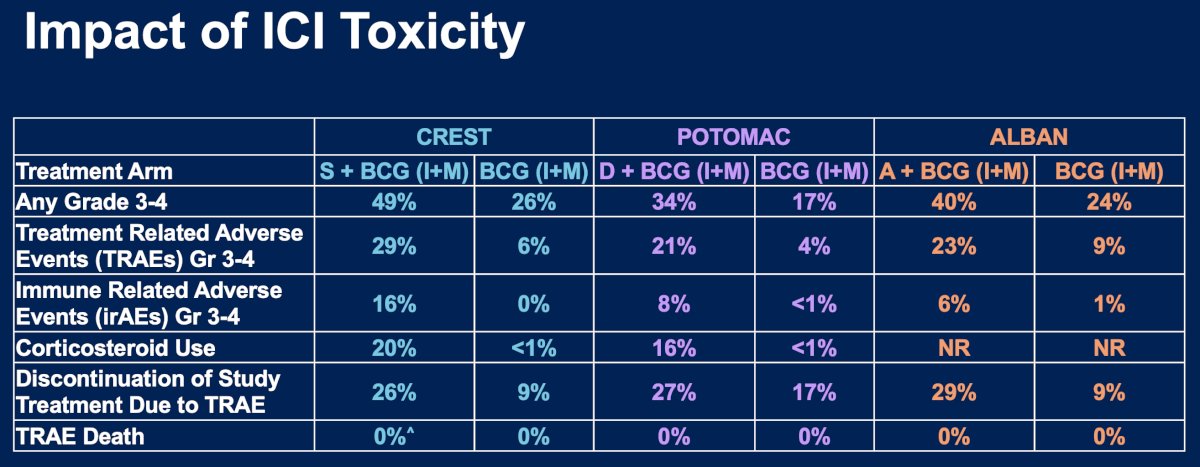
When immune checkpoint inhibition was added to BCG in the CREST, POTOMAC, and ALBAN trials, higher rates of grade 3–4 adverse events were observed compared with BCG alone. However, treatment-related mortality remained extremely rare, and the safety profile was consistent with that observed for ICI monotherapy.
Subgroup analyses from the randomized trials suggest that the benefit of ICI plus BCG may be greatest among patients with the highest-risk disease.
In CREST, patients with T1 tumors experienced improved outcomes with sasanlimab plus BCG compared with BCG alone (HR 0.63).3 Similarly, in POTOMAC, patients with high-risk papillary disease derived substantial benefit from durvalumab plus BCG (HR 0.54).2
In contrast, ALBAN—which enrolled a lower-risk population—did not demonstrate meaningful benefit from atezolizumab plus BCG.
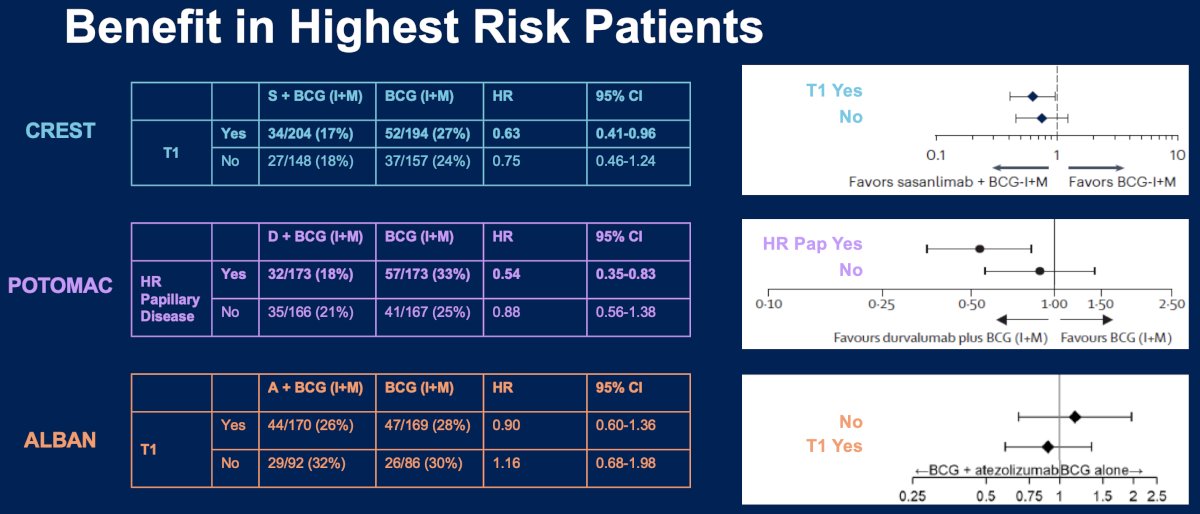
These findings suggest that patient selection will be critical in optimizing the clinical use of ICI-BCG combinations.
Value Proposition of ICI + BCGDr. Hahn concluded by summarizing the clinical rationale for combining immune checkpoint inhibitors with intravesical BCG in HR-NMIBC:
- HR NMIBC recurrences significantly impact patient lives – “The Endless Recurrence Cycle”
- Patients uniformly prioritize bladder preservation strategies
- BCG-unresponsive options have yet to demonstrate durable cures once treatment is stopped
- The toxicities observed when ICI is added to BCG (I+M) mirror the consistent and established safety profile of ICI monotherapy
- The benefit of adding ICI to BCG (I+M) is greatest in BCG-naïve NMIBC patients with the “highest risk” disease
Presented by: Noah M. Hahn, MD, Associate Professor of Medicine, Department of Oncology and Urology, Johns Hopkins University School of Medicine, Baltimore, MD, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- Shore ND, Lerner SP, Chamie K, et al. Sasanlimab plus bacillus Calmette–Guérin in patients with BCG-naïve high-risk non–muscle-invasive bladder cancer (CREST): A randomized phase 3 trial. Nat Med. 2025;31:2806–2814.
- De Santis M, Powles T, Balar AV, et al. Durvalumab plus bacillus Calmette–Guérin for BCG-naïve high-risk non–muscle-invasive bladder cancer (POTOMAC): Results from a randomized phase 3 study. Lancet. 2025;406:2221–2234.
- Shore ND, Lerner SP, Bivalacqua TJ, et al. CREST trial: Sasanlimab combined with bacillus Calmette–Guérin in BCG-naïve high-risk non–muscle-invasive bladder cancer. Presented at the American Urological Association Annual Meeting. 2025.
- Roupret M, Powles T, Balar AV, et al. Atezolizumab plus bacillus Calmette–Guérin for high-risk non–muscle-invasive bladder cancer: Results from the ALBAN randomized trial. Ann Oncol. 2026;37:44–52.
- Holzbeierlein JM, Boorjian SA, Bivalacqua TJ, et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline amendment 2024. J Urol. 2024;211:533–538.
- Babjuk M, Burger M, Capoun O, et al. European Association of Urology guidelines on non-muscle-invasive bladder cancer (Ta, T1, and carcinoma in situ). Eur Urol. 2022;81:75–94.
- Kopenhafer L, Chamie K, Kamat AM, et al. Patient perspectives on bladder preservation and treatment priorities in high-risk non-muscle-invasive bladder cancer. Urol Oncol. 2024;42:70.e1–70.e10.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A phase 3 trial. Lancet Oncol. 2021;22:107–117.
- Steinberg RL, Thomas LJ, Brooks NA, et al. Multi-institution evaluation of sequential intravesical gemcitabine and docetaxel as salvage therapy for non-muscle-invasive bladder cancer. J Urol. 2020;203:902–909.
- Chamie K, Chang SS, Boorjian SA, et al. Nogapendekin alfa inbakicept for BCG-unresponsive non-muscle-invasive bladder cancer: Results from a multicenter clinical study. NEJM Evid. 2022;2:1–11.
- Narayan VM, Shore ND, Boorjian SA, et al. Long-term outcomes following intravesical nadofaragene firadenovec therapy in patients with BCG-unresponsive non-muscle-invasive bladder cancer. J Urol. 2024;212:74–86.
- Quek ML, Stein JP, Nichols PW, et al. Perioperative mortality and morbidity after radical cystectomy for bladder cancer in a contemporary series. J Urol. 2006;175:886–889.
- Hollenbeck BK, Miller DC, Taub DA, et al. Mortality following radical cystectomy: National patterns and predictors of perioperative outcomes. Urology. 2007;69:871–875.
- Hounsome LS, Verne J, McGrath JS, et al. Trends in radical cystectomy outcomes and perioperative mortality for bladder cancer in England. Eur Urol. 2015;67:1056–1062.
- Novotny V, Hakenberg OW, Wiessner D, et al. Perioperative mortality and complications after radical cystectomy for bladder cancer: A population-based analysis. Eur Urol. 2007;51:397–402.