(UroToday.com) The 2026 ASCO GU Annual Symposium featured a prostate and urothelial cancers poster session. Dr. Ali Raza Khaki presented an analysis evaluating quality-of-care (QoC) measures among Medicare-insured patients with recurrent, papillary-only bacillus Calmette–Guérin (BCG)–experienced high-risk non–muscle invasive bladder cancer (HR-NMIBC).
HR-NMIBC is associated with a high disease burden and substantial likelihood of recurrence and progression, requiring intensive surveillance and management through multiple interventions.1,2 Patients who experience disease recurrence after treatment with bacillus Calmette–Guérin (BCG) frequently face additional treatment decisions and may require further bladder-directed therapies or radical cystectomy.3-5 Due to the high disease burden, the National Comprehensive Cancer Network (NCCN) and the American Urologic Association (AUA) Quality (AQUA) Registry have developed several quality-of-care (QoC) measures aimed at improving patient outcomes.6,7 However, real-world data evaluating QoC measures among patients with recurrent, papillary-only HR-NMIBC, particularly those who are BCG-experienced, remain limited.
The objective of this study was to characterize QoC measures among Medicare-insured patients in the United States with HR-NMIBC with papillary-only recurrence who were BCG-experienced and had disease recurrence.
To address this question, the investigators conducted a retrospective study using the Surveillance, Epidemiology, and End Results (SEER)–Medicare database. This dataset links the SEER cancer registry with Medicare claims data and captures cancer incidence, demographic data, tumor characteristics, and healthcare utilization. Data were de-identified and complied with the Health Insurance Portability and Accountability Act (HIPAA) regulations.
The study design and cohort identification are summarized in Figure 1. The index date was defined as the date of HR-NMIBC diagnosis. Baseline information was obtained during the 12-month period of continuous enrollment prior to the index date, while the observation period extended from the index date until death or the end of follow-up.
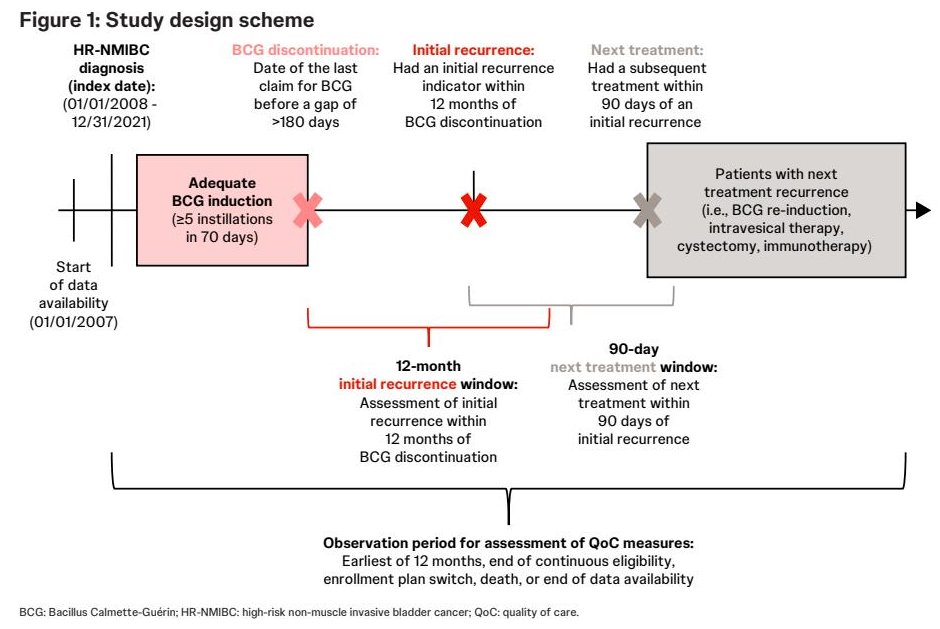
Patients were included if they were ≥65 years of age with HR-NMIBC with papillary-only recurrence who experienced disease recurrence within 12 months after BCG induction therapy. BCG-experienced patients were defined as those who had received adequate induction BCG therapy prior to recurrence. Recurrent disease was defined as recurrence occurring between 12 months and two years following adequate BCG induction therapy.
Subsequent BCG-related treatment was defined as treatment observed within 90 days of disease recurrence and included intravesical therapy, cystectomy, immunotherapy, radiation therapy, or systemic therapy. Monitoring, treatment, and healthcare services-related QoC measures were assessed during the observation period. Results were reported descriptively using means, standard deviations, and medians for continuous variables, and frequencies and proportions for categorical variables.
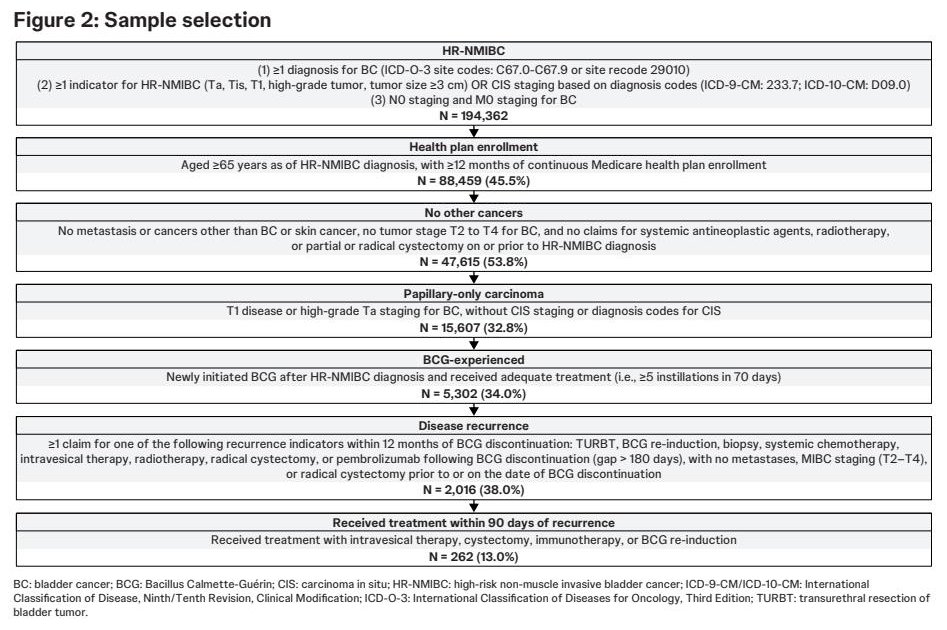
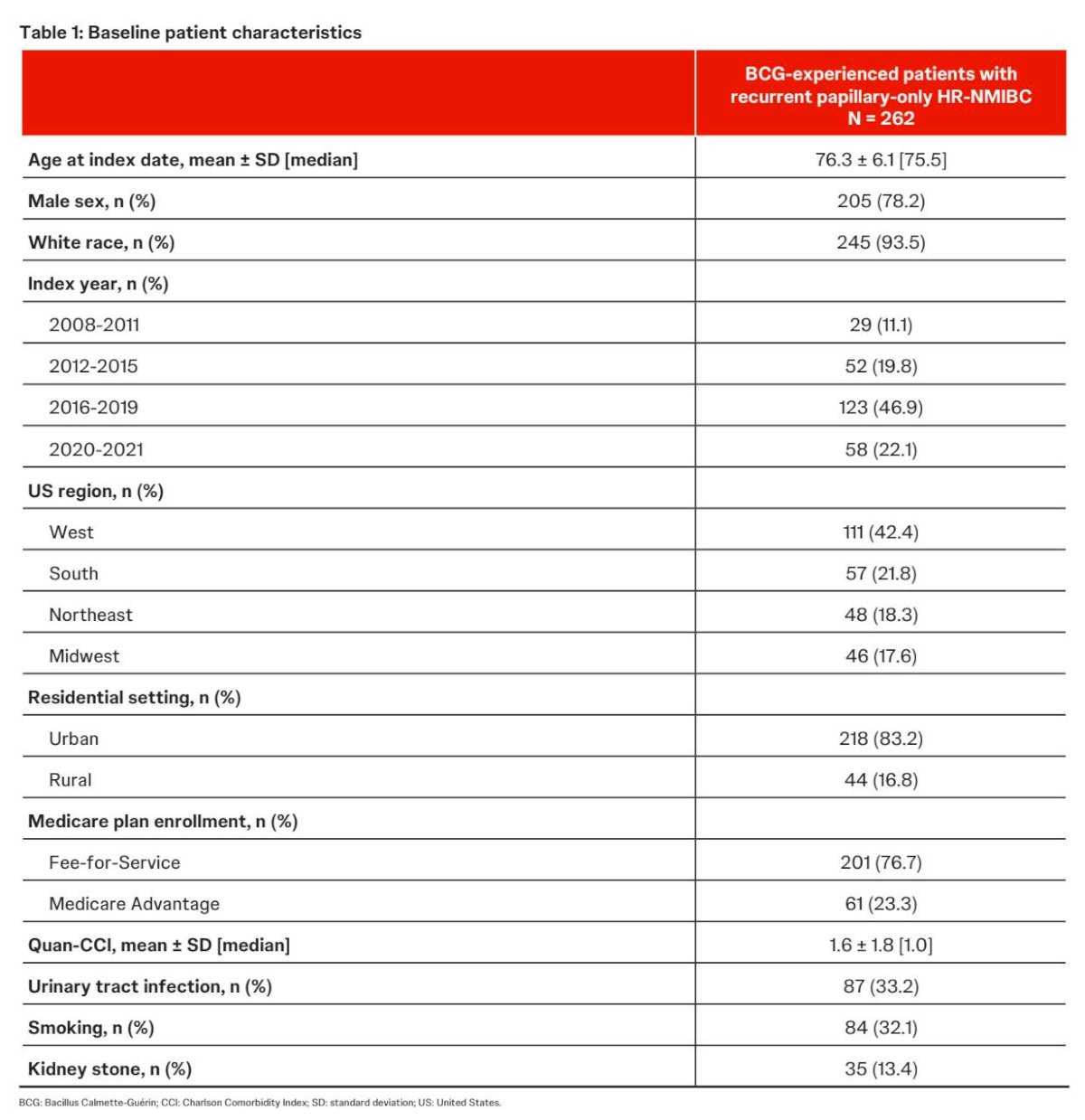
Overall, 262 BCG-experienced patients with HR-NMIBC with papillary-only carcinoma who received treatment within 90 days of disease recurrence were included. The mean age of the cohort was 76 years, 78% were male, and 94% were White. Most patients resided in urban settings. The cohort included patients diagnosed between 2008 and 2021, with representation across U.S. geographic regions including the West, South, Northeast, and Midwest.
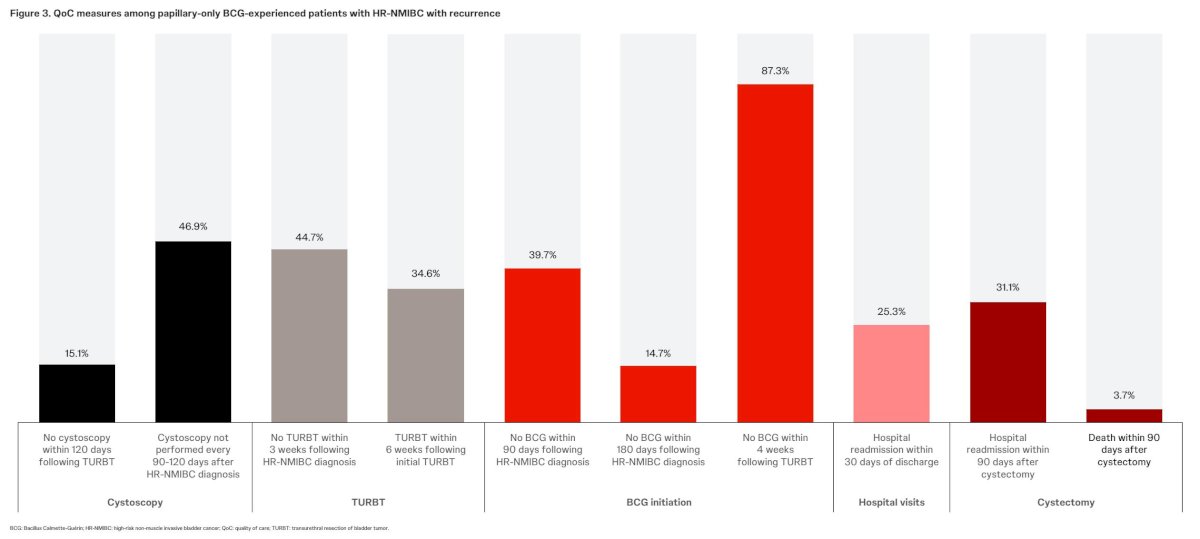
Quality-of-care metrics were evaluated across several domains including cystoscopic surveillance, procedural interventions, intravesical therapy utilization, and hospital utilization.
Among patients undergoing transurethral resection of bladder tumor (TURBT), 15.1% did not undergo cystoscopy within 120 days following TURBT. Regular cystoscopic surveillance every three months following HR-NMIBC diagnosis occurred in 46.9% of patients.
Assessment of repeat TURBT demonstrated additional variability in adherence to QoC measures. Among patients undergoing TURBT, 44.7% did not undergo repeat TURBT within six weeks following HR-NMIBC diagnosis. Similarly, 34.6% of patients did not undergo repeat TURBT within six weeks following their initial TURBT procedure.
QoC metrics related to intravesical therapy demonstrated additional gaps in care. Among patients with HR-NMIBC, 39.7% did not receive BCG therapy within 90 days following diagnosis, while 14.7% did not receive BCG therapy within 180 days following diagnosis.
Hospital utilization outcomes were also evaluated. Hospital readmission within 30 days of discharge occurred in 25.3% of patients. Hospital readmission within 90 days after cystectomy occurred in 31.1% of patients, while mortality within 90 days following cystectomy was observed in 3.7% of patients.
Taken together, these findings highlight important gaps in quality-of-care measures among Medicare-insured patients with recurrent papillary-only HR-NMIBC who are BCG-experienced. Less than half of patients consistently received recommended surveillance and treatment measures within guideline-recommended timeframes.
The investigators concluded that significant gaps in care persist for BCG-experienced patients with recurrent papillary-only HR-NMIBC, particularly in monitoring, treatment delivery, and healthcare services received. More consistent assessment of QoC measures for patients with HR-NMIBC could help address these gaps in care and improve both short- and long-term patient outcomes.
Presented by: Ali Raza Khaki, MD, Clinical Assistant Professor, Medical Oncologist, Department of Medicine, Stanford University School of Medicine, Palo Alto, CA, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- Holzbeierlein JM, Castle EP, Thrasher JB, et al. Quality of care for non–muscle-invasive bladder cancer: adherence to guideline-recommended surveillance and treatment. J Urol. 2024;211(4):533–538.
- Longoni M, Necchi A, Moschini M, et al. Bacillus Calmette–Guérin–unresponsive non–muscle-invasive bladder cancer: definitions, clinical outcomes, and evolving treatment strategies. Eur Urol Oncol. 2025;8(5):1375–1392.
- Tan WS, Rodney S, Lamb B, et al. Management of Bacillus Calmette–Guérin–unresponsive non–muscle-invasive bladder cancer: contemporary treatment strategies and emerging therapies. Eur Urol Open Sci. 2023;53:16–22.
- Kulkarni GS, Klaassen Z, Zlotta AR, et al. Contemporary management of Bacillus Calmette–Guérin–unresponsive non–muscle-invasive bladder cancer. Clin Genitourin Cancer. 2025;23(3):102313.
- Li R, Black PC, Kamat AM, et al. Emerging intravesical therapies for Bacillus Calmette–Guérin–unresponsive non–muscle-invasive bladder cancer. Eur Urol. 2020;78(3):387–399.
- Shelton JB, McKiernan JM, Bivalacqua TJ, et al. Contemporary management of Bacillus Calmette–Guérin–unresponsive non–muscle-invasive bladder cancer in clinical practice. Urol Pract. 2021;8(2):209–216.
- D’Amico TA, Chen RC, Kutikov A, et al. National Comprehensive Cancer Network guidelines insights: bladder cancer, version updates and management recommendations. J Natl Compr Canc Netw. 2020;18(3):250–259.