(UroToday.com) The 2026 ASCO GU Annual Symposium featured a prostate and urothelial cancers poster session. Dr. Cindy Jiang presented results from the UNITE study evaluating outcomes with second-line therapies following first-line enfortumab vedotin plus pembrolizumab (EVP) in patients with advanced urothelial carcinoma (aUC).
EVP has significantly shifted the treatment paradigm for aUC and is now the preferred first-line therapy. Despite these advances, approximately 10% of patients experience progression as their best response, and roughly 63% develop disease progression by 24 months. Outcomes with subsequent therapies following EVP are not well defined and warrant further evaluation.
The investigators conducted a multi-institutional retrospective cohort study as part of the UNITE dataset. The study included patients who received systemic therapy for advanced urothelial carcinoma and specifically included patients who received at least one cycle of first-line EV followed by second-line treatment. Median progression-free survival (PFS) and overall survival (OS) were estimated using Kaplan–Meier methodology from both the start of EVP and the start of second-line therapy. Median follow-up from EVP initiation and from second-line therapy initiation was calculated using the reverse Kaplan–Meier method.
Overall response rate (ORR) was investigator-assessed using RECIST v1.1 criteria. Odds of response and survival outcomes for each second-line therapy were compared with platinum-based chemotherapy using univariable logistic regression analyses. Limitations of the analysis included its retrospective nature, lack of central radiographic review, potential selection bias, and unmeasured confounding.
A total of 377 patients initially received first-line EVP. Among these, 115 remained on first-line therapy at the time of analysis, 58 progressed without receiving second-line therapy, and 20 had unknown subsequent treatment status. A subset of patients discontinued therapy for intolerance, were lost to follow-up, or transitioned to consolidation strategies. Ultimately, 68 patients received second-line therapy following EVP, and 53 patients with evaluable data were included in the second-line outcomes analysis.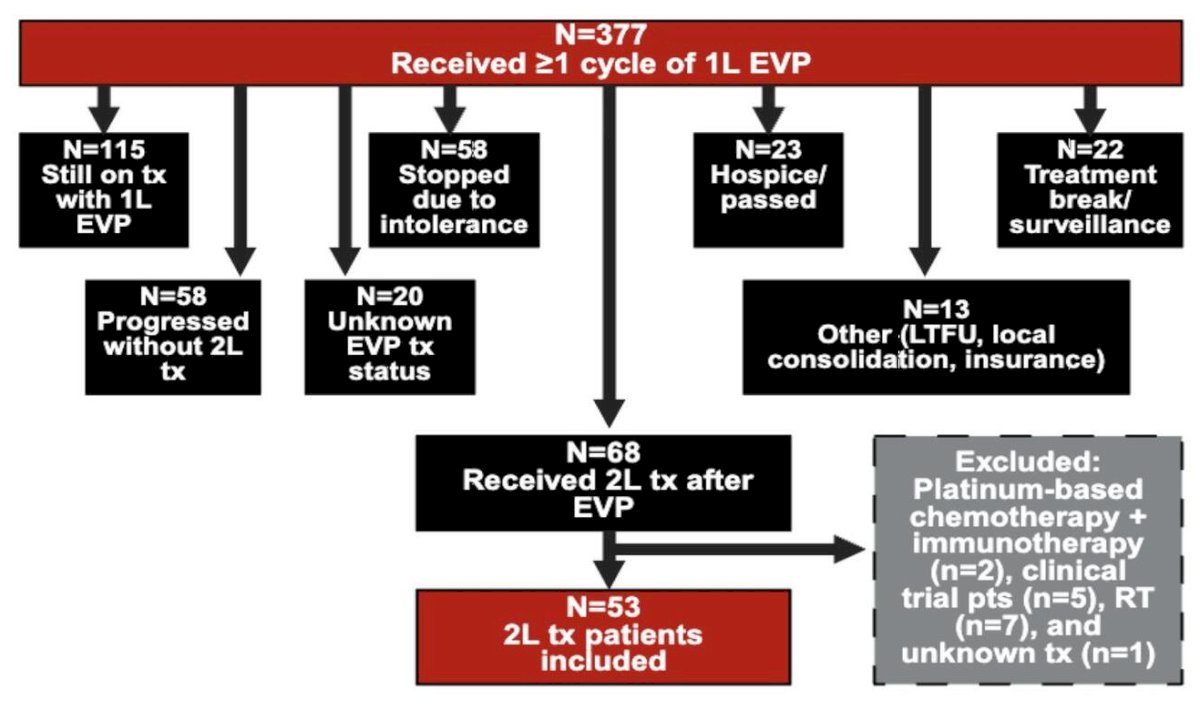
Baseline clinical characteristics of the 53 patients receiving second-line therapy were reported. The median age was 71 years (range 46–96), and the majority were male (83%). Most patients were White (79%), followed by Black patients (4%), with a small proportion categorized as other or unknown race. With respect to primary tumor location, most tumors originated in the bladder (68%), followed by upper tract tumors (28%). Histologically, 57% of tumors were pure urothelial carcinoma, while the remainder demonstrated mixed urothelial or variant histologies.
Clinical characteristics at EVP initiation were also reported. The median body mass index was 26 kg/m². Most patients did not have diabetes mellitus (83%), and the majority had no prior neuropathy (75%). ECOG performance status at EVP initiation was 0 in 37% of patients and 1 in 53%.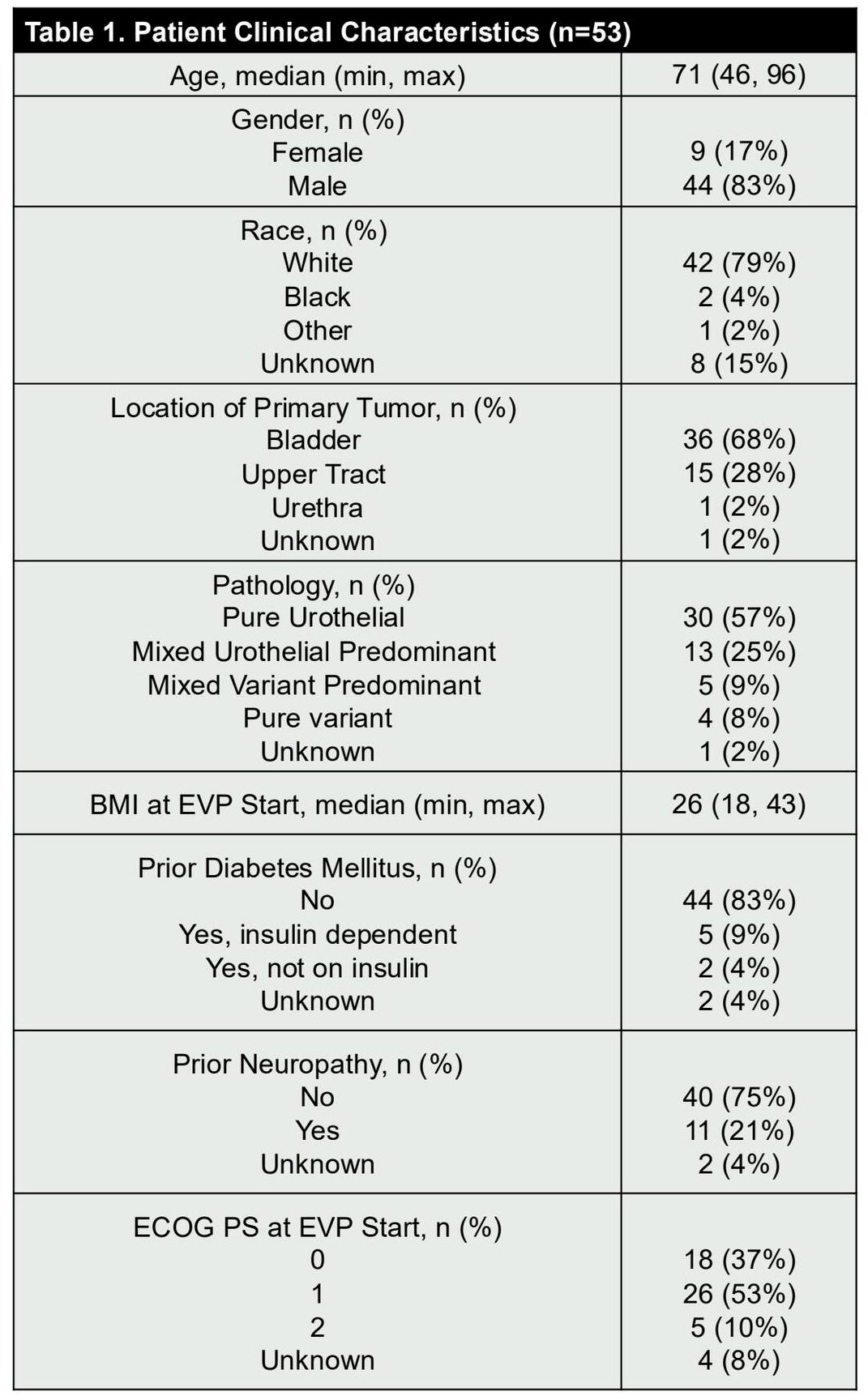
Outcomes with first-line EVP were also summarized. Median follow-up from EVP initiation was 18 months (95% CI 14.5–20.5). The best overall response rate to first-line EVP was 45%, including 3 complete responses and 21 partial responses. Median progression-free survival with EVP was 5.5 months (95% CI 4.4–7.1), and median overall survival from EVP initiation was 19.8 months (95% CI 18.2–not reached).
Subsequent treatment patterns following progression on EVP demonstrated substantial heterogeneity. The most commonly administered second-line therapy was platinum-based chemotherapy (n=24). Other therapies included sacituzumab govitecan (n=14), erdafitinib (n=7), trastuzumab deruxtecan (n=6), taxane-based chemotherapy (n=2), and T-DXd–based regimens in a small number of patients. These treatment patterns illustrate the diverse strategies used in clinical practice following progression on EVP.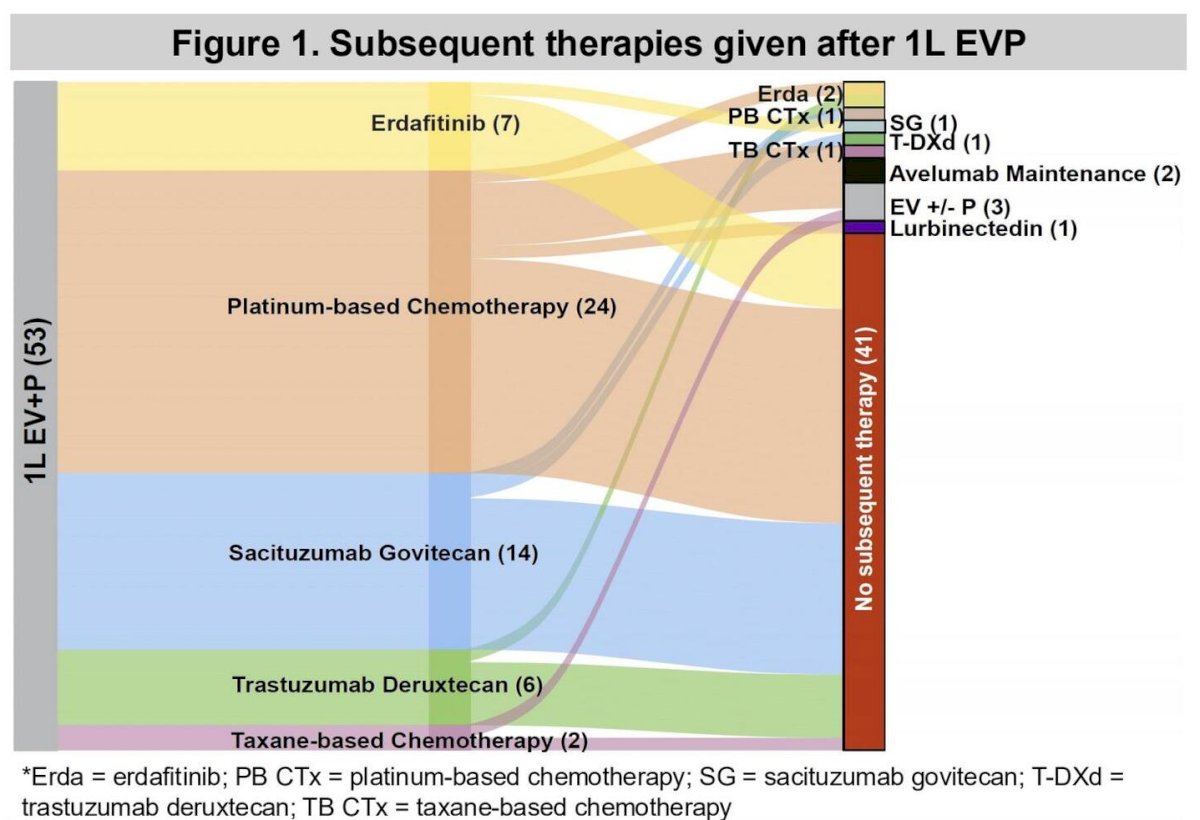
Among patients receiving second-line therapy, the median follow-up time from initiation of second-line treatment was 10.13 months (95% CI 5.79–13.35). The best overall response rate to second-line therapy was 24%, including two complete responses and six partial responses.
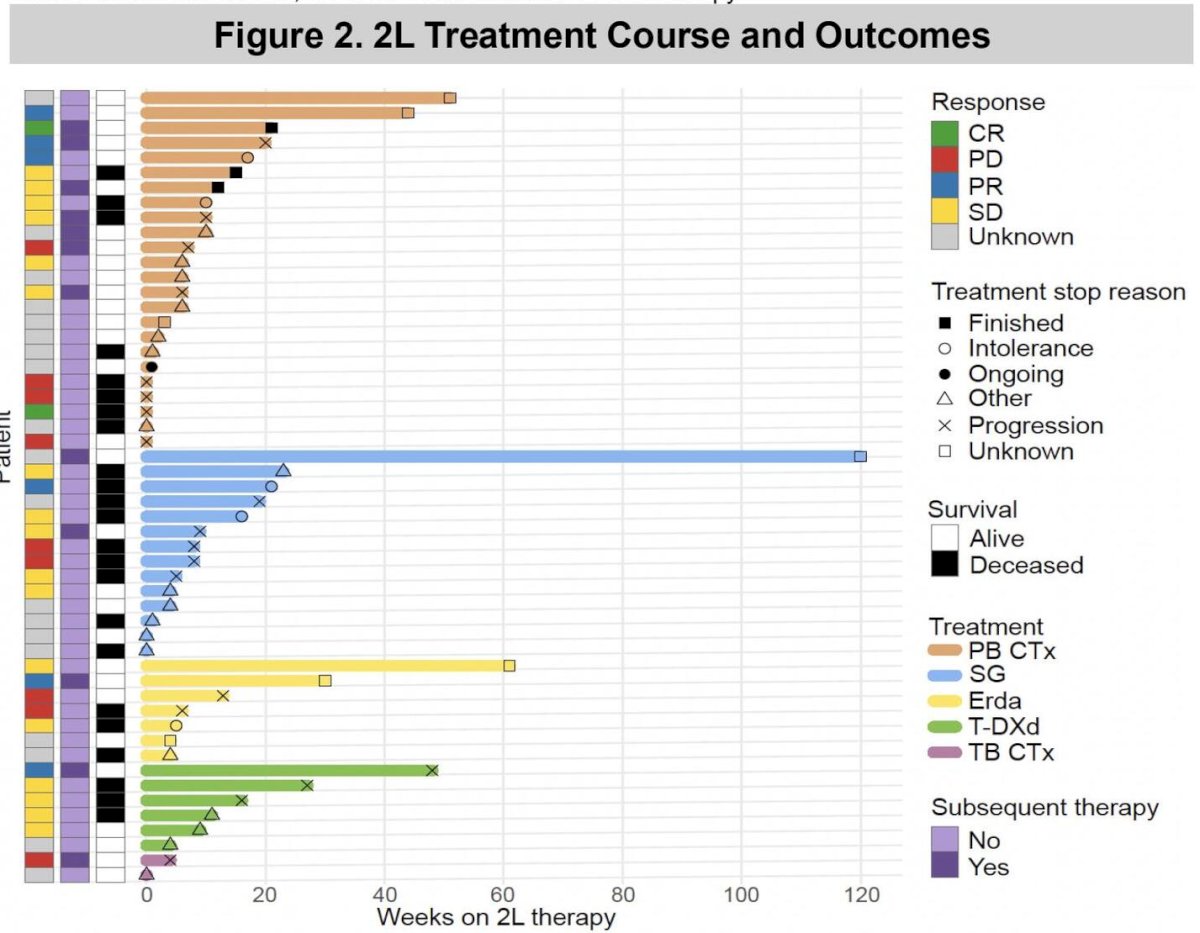
Median progression-free survival with second-line therapy was 2.76 months (95% CI 1.84–6.21). Median overall survival from the start of second-line therapy was 8.98 months (95% CI 5.98–not available).
Comparative analyses suggested no clear survival advantage for non–platinum-based therapies compared with platinum chemotherapy, although sample sizes were small. For example, sacituzumab govitecan demonstrated an ORR of 13%, whereas erdafitinib demonstrated an ORR of 20%. Progression-free and overall survival outcomes were similarly modest across treatment categories.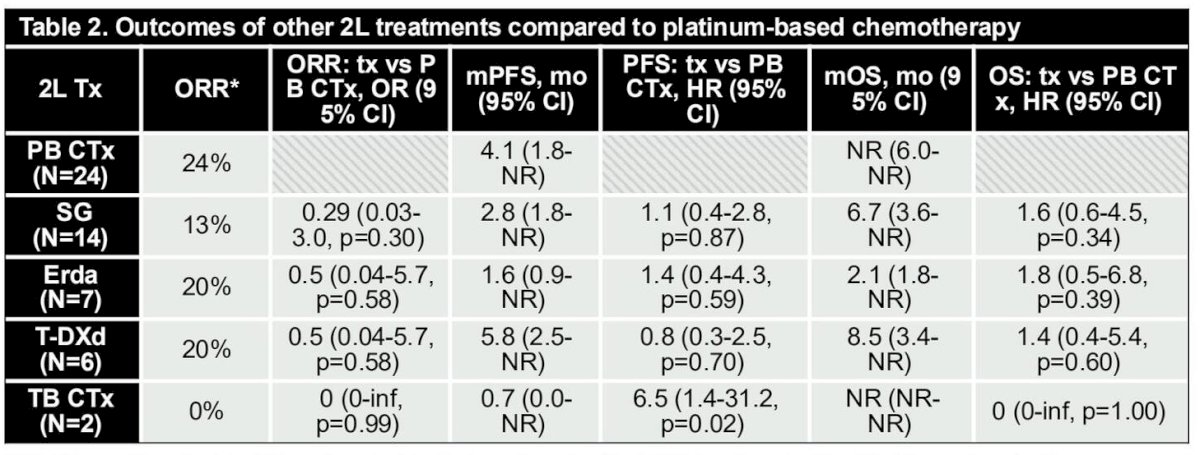
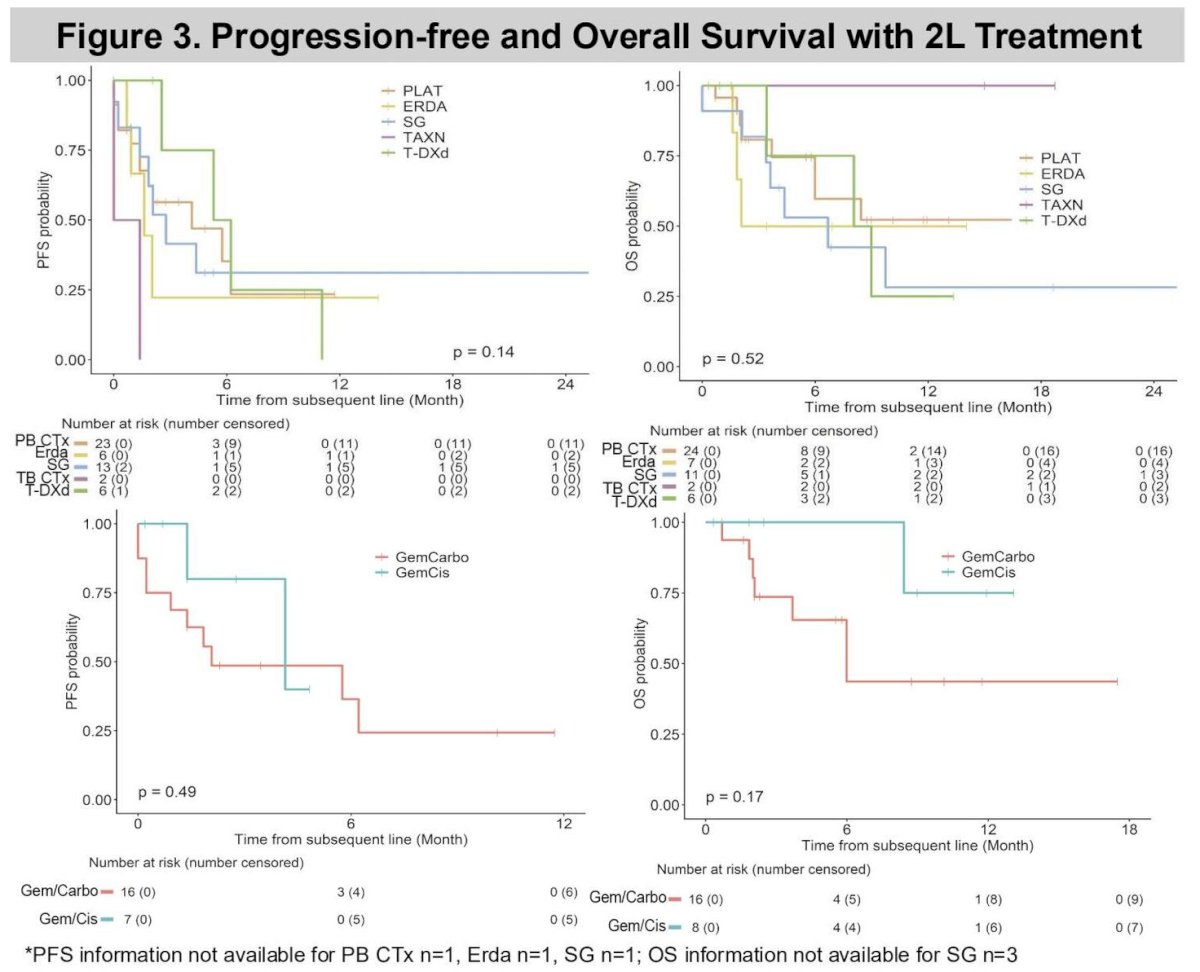
Kaplan–Meier analyses of progression-free survival and overall survival by second-line treatment type demonstrated overlapping survival curves, further reflecting the limited durability of currently available therapies in the post-EVP setting.
Overall, the investigators concluded that modest response rates and relatively short survival outcomes are observed with currently available second-line therapies following EVP in patients with advanced urothelial carcinoma. Platinum-based chemotherapy represented the most commonly used second-line therapy in this cohort. These findings highlight the need for additional systemic therapy development in the post-EVP treatment setting.
The authors emphasized that larger cohorts will be required to better define potential differences between cisplatin- versus carboplatin-based regimens and other therapies in this setting. The results are hypothesis-generating and may inform prognostic estimates as well as the design of future clinical trials evaluating therapies following progression on EVP.
Presented by: Cindy Y. Jiang, MD, The University of Texas MD Anderson Cancer Center, Houston, TX, USA