(UroToday.com) The 2026 ASCO GU Annual Symposium featured a prostate and urothelial cancers poster session. Dr. Emily Smyth presented a real-world analysis evaluating patterns and disparities in FGFR3 genomic testing among patients with locally advanced or metastatic urothelial carcinoma (LA/mUC) in the United States.
FGFR3 genetic alterations occur in 15–20% of patients with LA/mUC, and treatment guidelines recommend biomarker-directed therapy for patients with one or more prior lines of treatment. Genomic testing for FGFR3 in the United States is recommended at the time of LA/mUC diagnosis; however, real-world adherence to these recommendations and potential disparities in testing remain poorly understood.
To evaluate these patterns, the investigators conducted a retrospective analysis using the Flatiron Health Bladder Panoramic Dataset, which includes longitudinal, de-identified electronic health record data from both community and academic oncology practices across the United States from January 1, 2022, through May 31, 2025.
Key inclusion criteria included a diagnosis of LA/mUC between January 2022 and March 2025, pathology consistent with urothelial carcinoma, and at least two clinic visits on or after January 1, 2015. The frequency and timing of FGFR3 testing were summarized, and comparisons between patient groups were assessed using Fisher’s exact test or Chi-squared tests for categorical variables and t-tests for continuous variables. Multivariable logistic regression was used to evaluate associations between testing and patient characteristics, disease characteristics, and treatment setting (academic versus community practice). The proportion of patients with FGFR3 alterations—excluding variants of unknown significance and amplifications—as well as erdafitinib use were also reported.
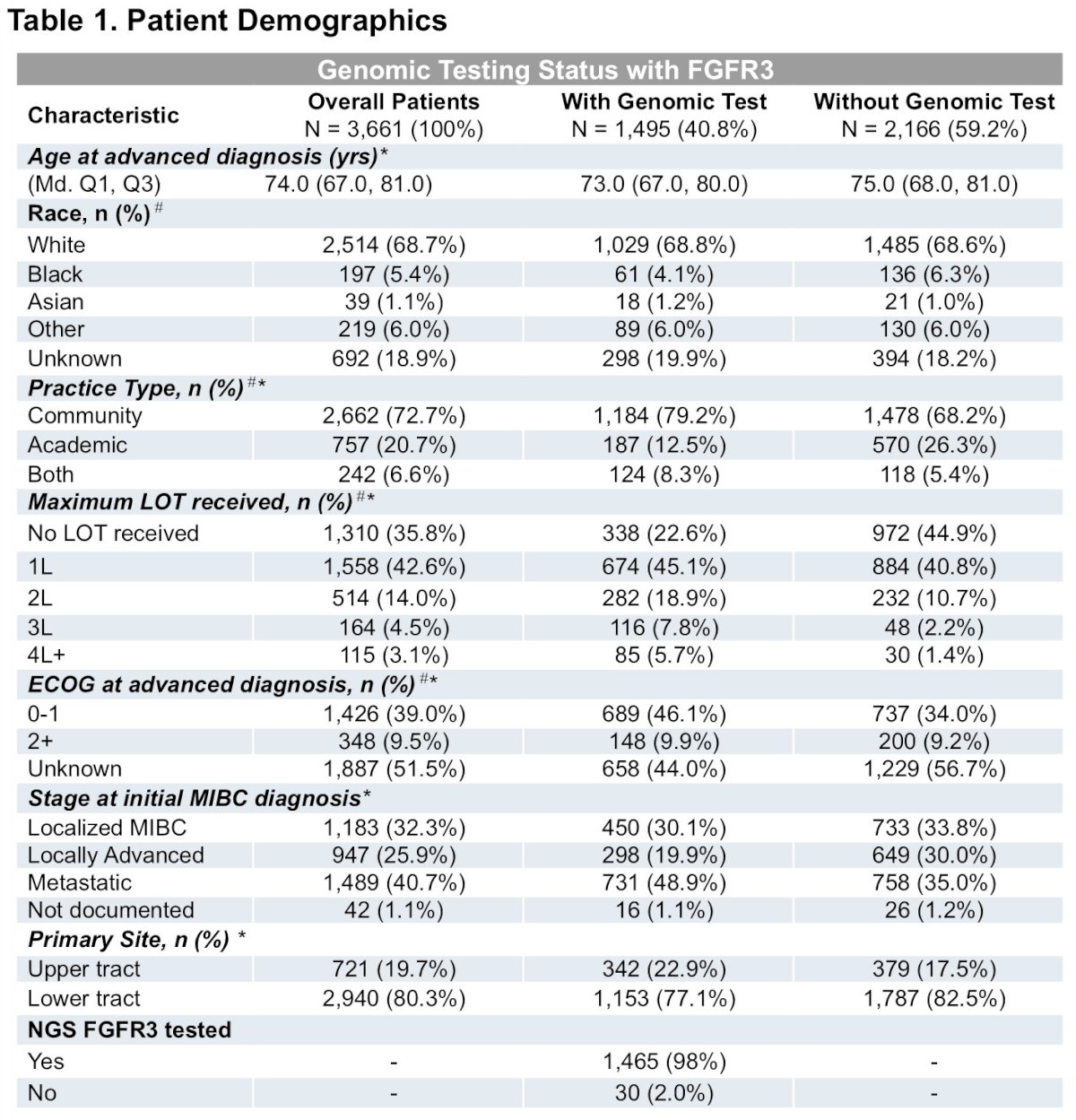
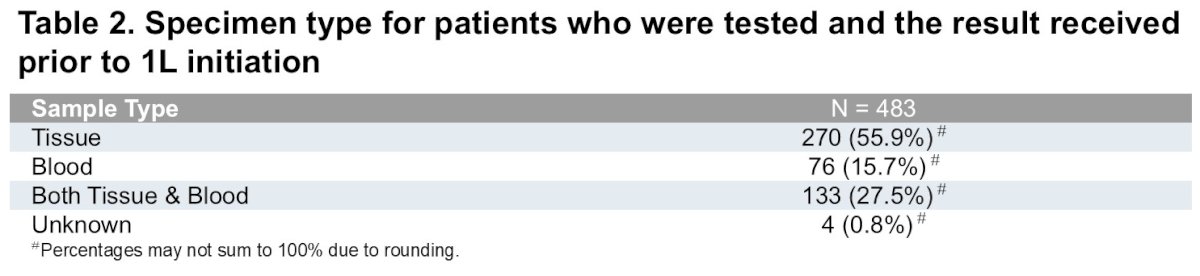
A total of 3,661 patients with LA/mUC were included in the analysis. Among these patients, 1,495 (40.8%) underwent FGFR3 testing at any point during their disease course. Of those tested with conclusive results, 19% were found to harbor FGFR3 alterations. FGFR3 positivity was more frequently observed among patients with upper tract primary tumors compared with lower tract tumors (26.5% versus 16.2%).
Baseline patient demographics demonstrated several differences between patients who underwent genomic testing and those who did not. Patients receiving testing were more likely to be treated in academic centers, receive later lines of therapy, and undergo genomic profiling in the context of broader precision oncology care. Conversely, patients without genomic testing were more frequently treated in community practices and were more likely to receive no systemic therapy or earlier-line treatment only.
Testing patterns varied substantially according to treatment timing. Overall, less than 30% of patients were tested prior to initiation of first-line systemic therapy. Specifically, testing rates prior to treatment initiation were 27.6% before first-line therapy, 51.2% before second-line therapy, 65.2% before third-line therapy, and 71.3% before fourth-line therapy. Among patients tested prior to first-line therapy, the median time from testing to treatment initiation was 17 days (range −483 to 648 days). Both tissue-based and blood-based testing modalities were utilized to enable biomarker testing prior to treatment initiation.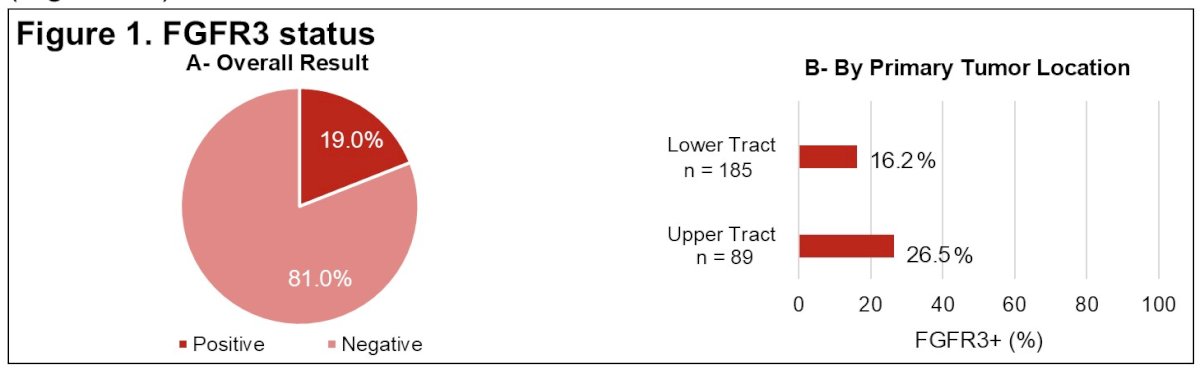
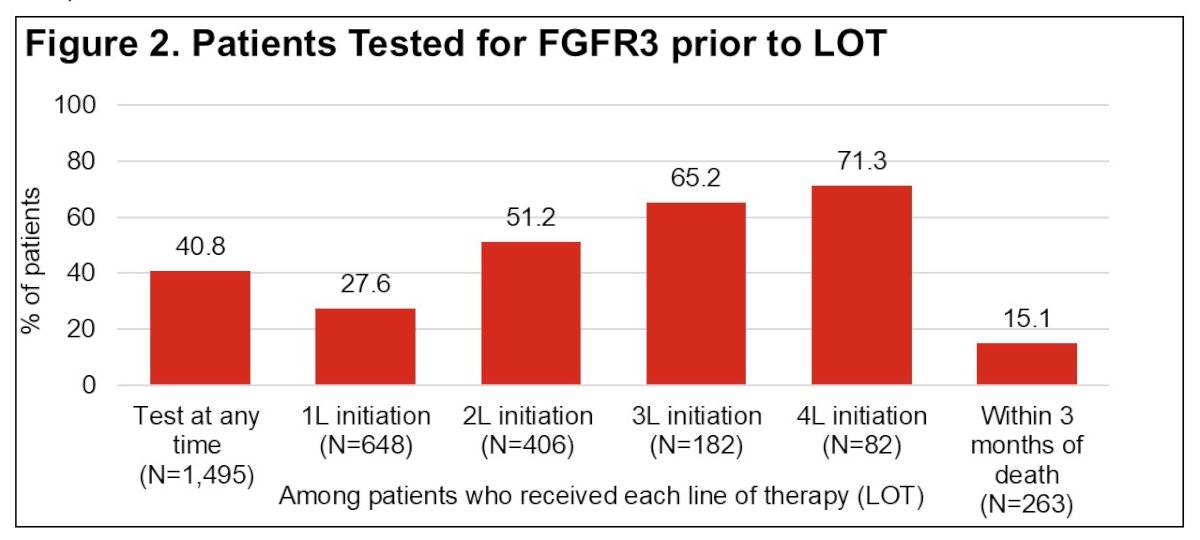
Specimen source among patients tested prior to first-line therapy included tumor tissue in 55.9% of cases, blood-based assays in 15.7%, both tissue and blood in 27.5%, and unknown sources in approximately 0.8%.
Temporal trends demonstrated a gradual decline in testing frequency over time. The proportion of patients undergoing FGFR3 testing at any time during their disease course decreased from 45.2% in 2022 to 34.3% in 2025. Similarly, the proportion of patients tested prior to first-line therapy decreased modestly during the same period.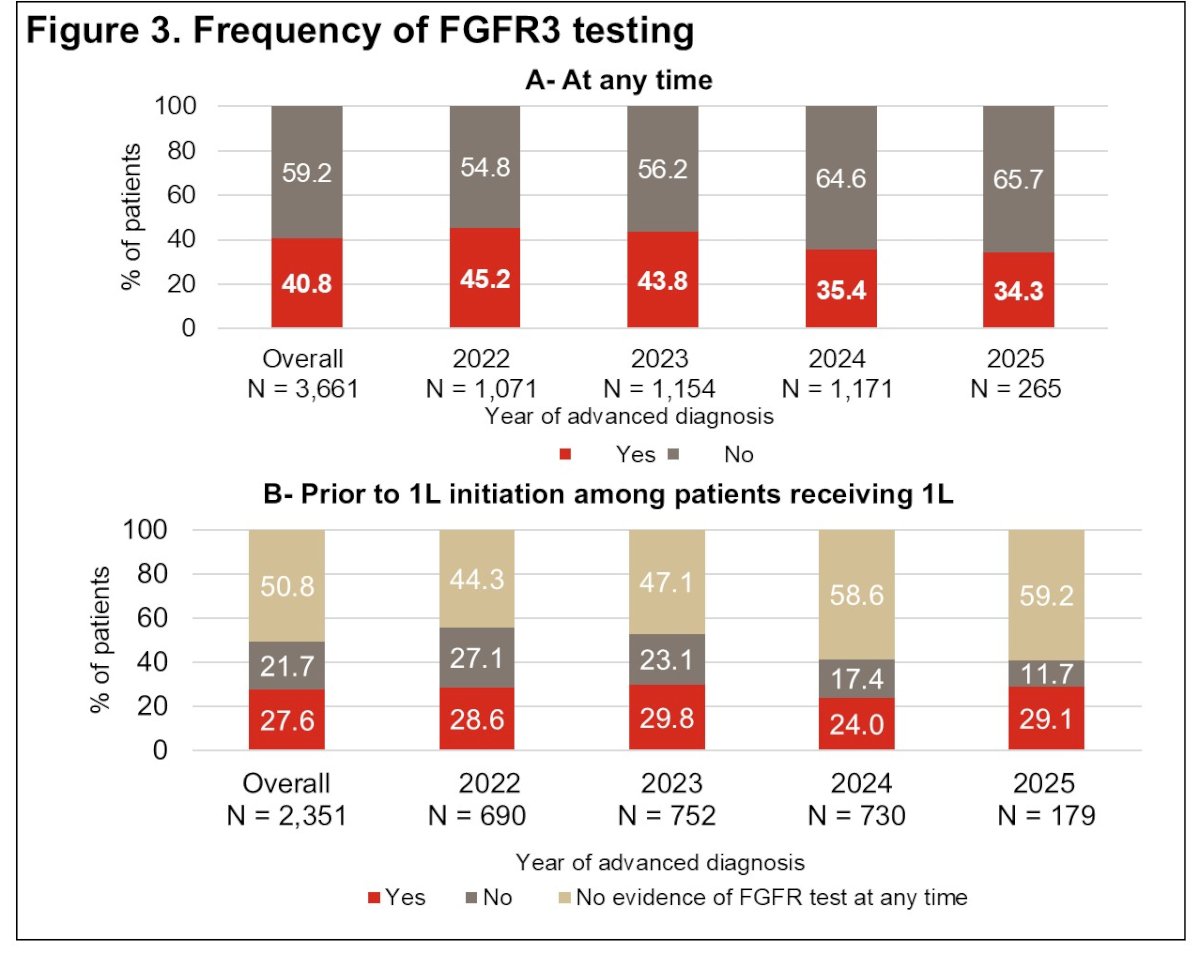
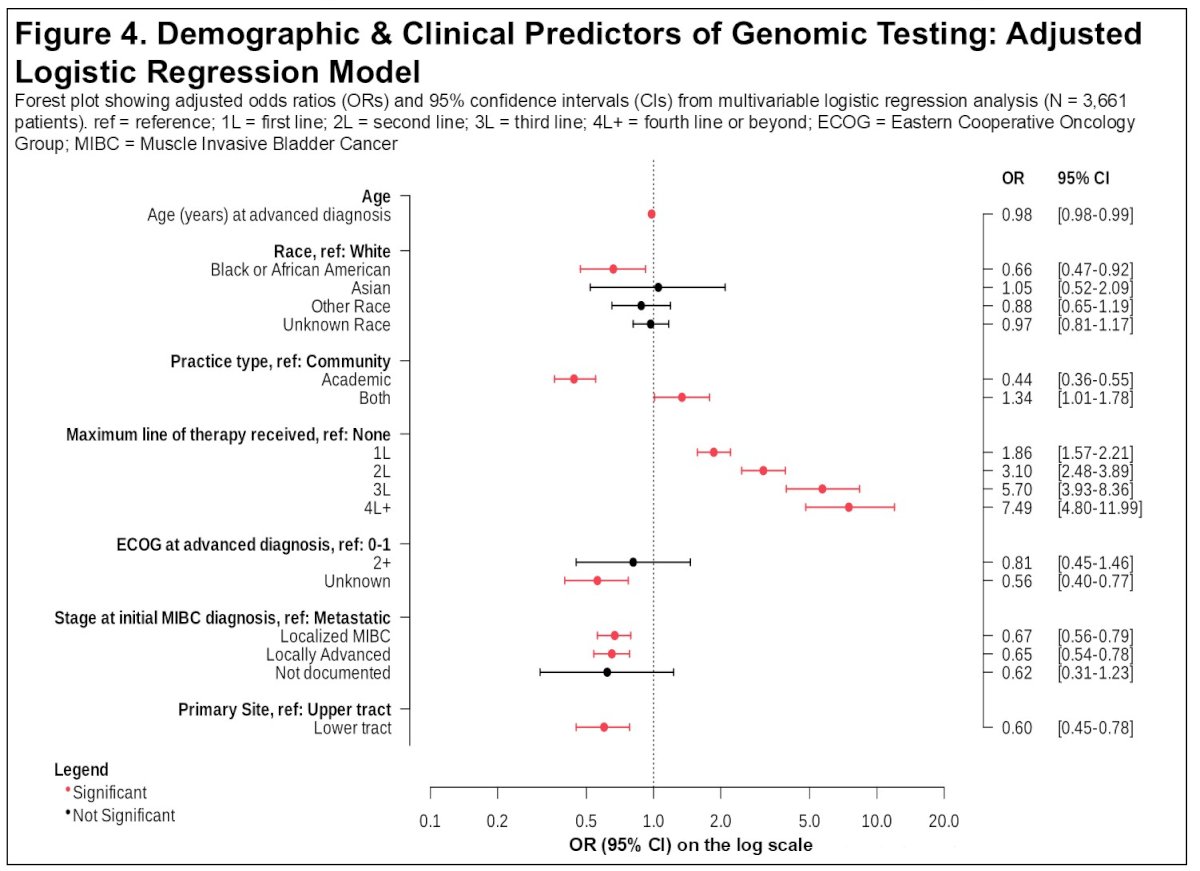
Multivariable logistic regression analysis identified several factors associated with lower odds of FGFR3 testing. Increasing age was associated with decreased likelihood of testing (odds ratio approximately 0.98 per year increase). Black population was associated with significantly lower odds of testing compared with White patients (OR approximately 0.66). Patients with lower tract primary tumors were also less likely to undergo genomic testing compared with those with upper tract disease (OR approximately 0.50). Additionally, patients treated in academic settings were more likely to receive FGFR3 testing compared with those treated in community practices.
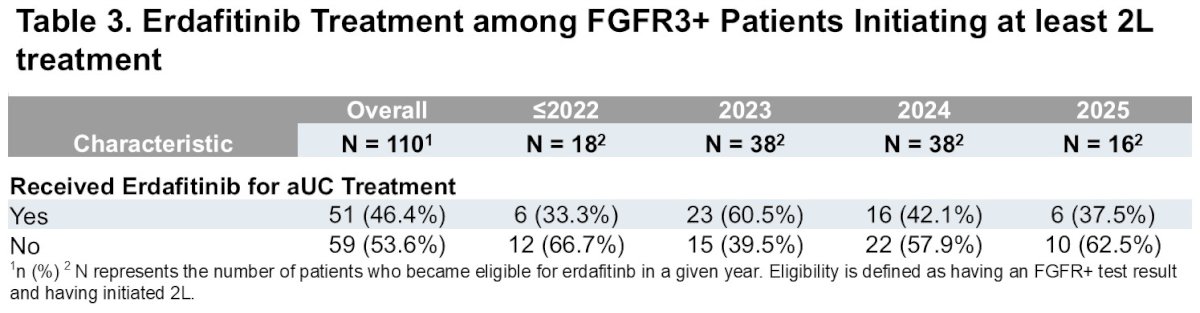
Despite the availability of targeted therapy for FGFR3-altered disease, treatment uptake remained limited. Among patients with FGFR3 alterations initiating second-line or later therapy and therefore eligible for targeted therapy, fewer than half ultimately received erdafitinib. Overall, 51 patients (46.4%) received erdafitinib, whereas 59 patients (53.6%) did not. Use of erdafitinib varied across calendar years but consistently remained below 50%.
These findings highlight important real-world gaps in biomarker-driven care for patients with urothelial carcinoma. In this large cohort of patients with LA/mUC, fewer than half underwent FGFR3 genomic testing, and less than one-third were tested prior to initiation of first-line therapy. Given that FGFR3 alterations represent an important and actionable oncogenic driver, these findings suggest missed opportunities for precision oncology.
The investigators note that several disparities in testing were observed. Patients who were Black, older, or had lower tract primary tumors were less likely to be tested, suggesting potential inequities in biomarker evaluation. Differences were also observed between academic and community practice settings, reflecting variability in genomic testing infrastructure and clinical workflows.
Importantly, even among patients who were eligible to receive targeted therapy, fewer than half ultimately received erdafitinib, suggesting additional barriers to precision treatment beyond testing alone.
The authors conclude that focused efforts are needed to improve adherence to biomarker testing guidelines, particularly prior to first-line treatment initiation, and to address disparities across patient populations and treatment settings. Improving access to genomic testing and targeted therapy may help maximize the benefits of precision oncology in urothelial carcinoma.
Presented by: Emily Nash Smyth, PharmD, Eli Lilly and Company, Indianapolis, USA