(UroToday.com) The 2026 ASCO GU Annual Symposium featured a prostate and urothelial cancers poster session. Dr. Georges Gebrael presented results evaluating real-world treatment approaches and outcomes in this evolving therapeutic landscape.
The landmark EV-302 trial demonstrated that the combination of enfortumab vedotin and pembrolizumab (EV+pembro) nearly doubled median overall survival (OS) and progression-free survival (PFS) compared with platinum-based chemotherapy, regardless of cisplatin eligibility.1 NCCN guidelines recommend biomarker-directed therapies, gemcitabine with cisplatin, gemcitabine with carboplatin, or dose-dense methotrexate, vinblastine, adriamycin, cisplatin (ddMVAC) chemotherapy with growth factor support as preferred options following progression on EV+pembro. However, data guiding treatment selection after progression on EV+pembro remains limited. Accordingly, this study aimed to characterize treatment patterns and outcomes in the second-line setting following first-line EV+pembro, addressing a gap in evidence and informing future therapeutic strategies.
Patient-level data were obtained using the US-based electronic health record–derived deidentified Flatiron Health Research Database. Patients were eligible if they had a diagnosis of advanced urothelial carcinoma (aUC), received first-ly546yine EV+pembro, and had documented second-line systemic therapy data available. Second-line treatment regimens were categorized into four groups based on the predominant systemic agent or combination received: (1) cisplatin-based therapy, (2) carboplatin-based therapy, (3) EV rechallenge, and (4) other therapies (including targeted therapies, non–platinum-based chemotherapy, immunotherapy rechallenge, or other non-approved agents).
The primary outcome was real-world overall survival (rwOS), defined as the time from initiation of second-line therapy to death from any cause. The secondary outcome was real-world time to next therapy (rwTTNT), defined as the time from initiation of second-line therapy to initiation of third-line therapy or death, whichever occurred first.
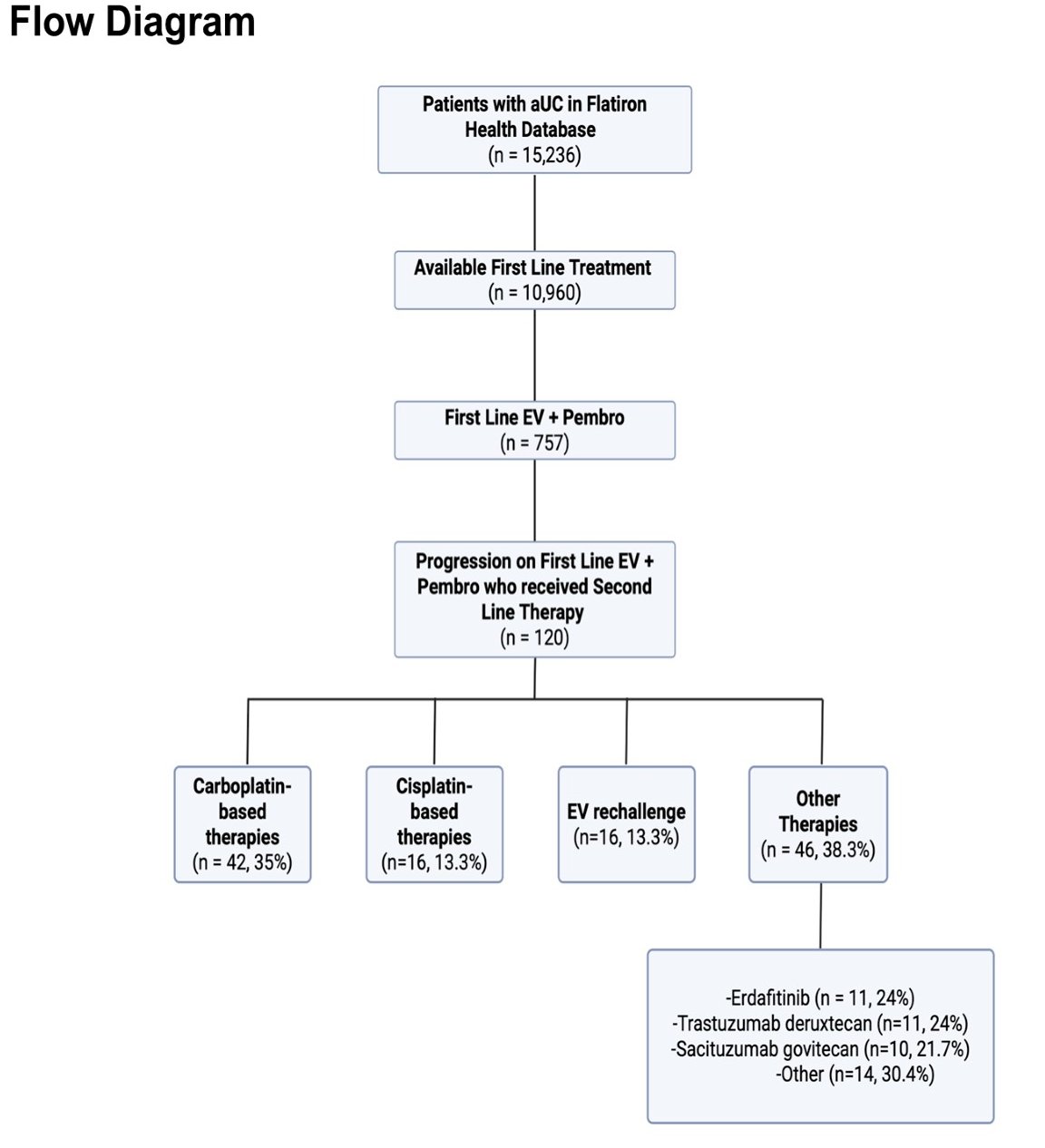
The study cohort was identified through a structured flow diagram beginning with patients with urothelial carcinoma in the Flatiron database (n=6,236), of whom 1,560 had available first-line treatment data. Among these, 120 patients had progression on first-line EV+pembro and received second-line therapy. Treatment distribution included carboplatin-based therapy (n=42), cisplatin-based therapy (n=16), EV rechallenge (n=16), and other therapies (n=46). Within the “other therapies” category, commonly used regimens included erdafitinib, trastuzumab deruxtecan, and sacituzumab govitecan.
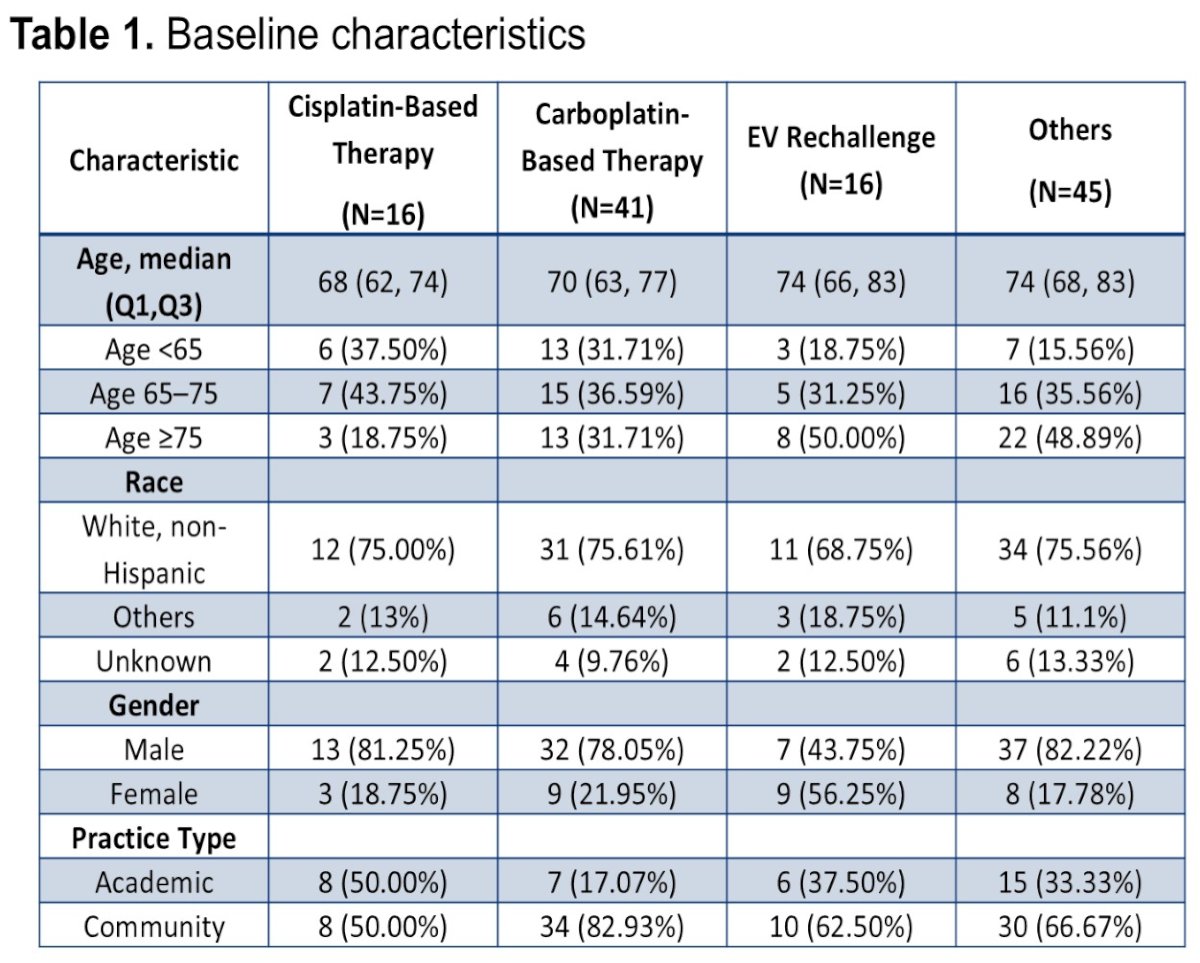
Baseline characteristics varied modestly across treatment groups. Median age ranged from 68 to 74 years depending on treatment category. Patients receiving carboplatin-based therapy had a median age of 70 years, while those receiving EV rechallenge had a median age of 74 years. The majority of patients across groups were male, reflecting the epidemiology of urothelial carcinoma. Most patients were White, and the majority were treated in community practice settings rather than academic centers.
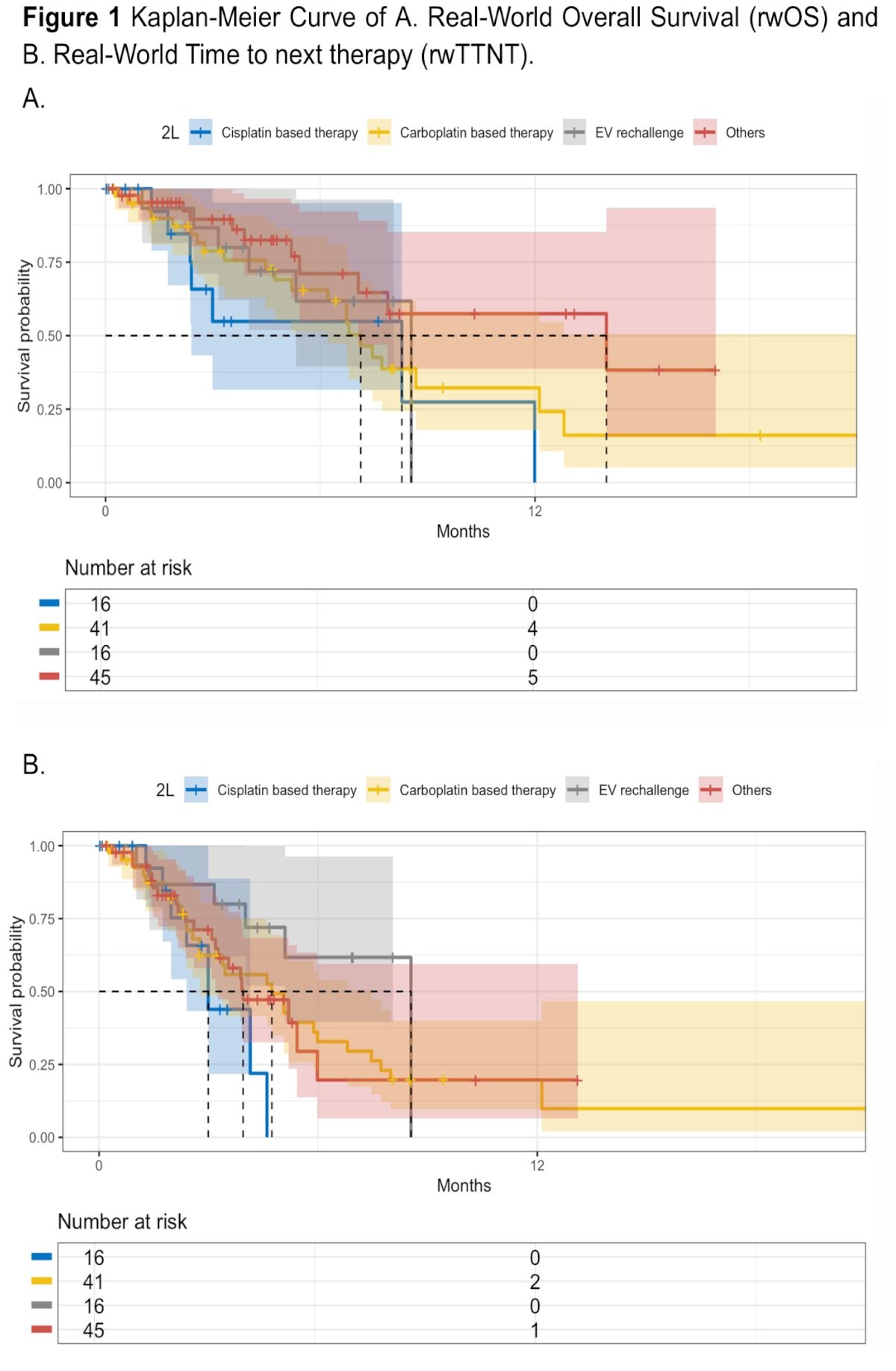
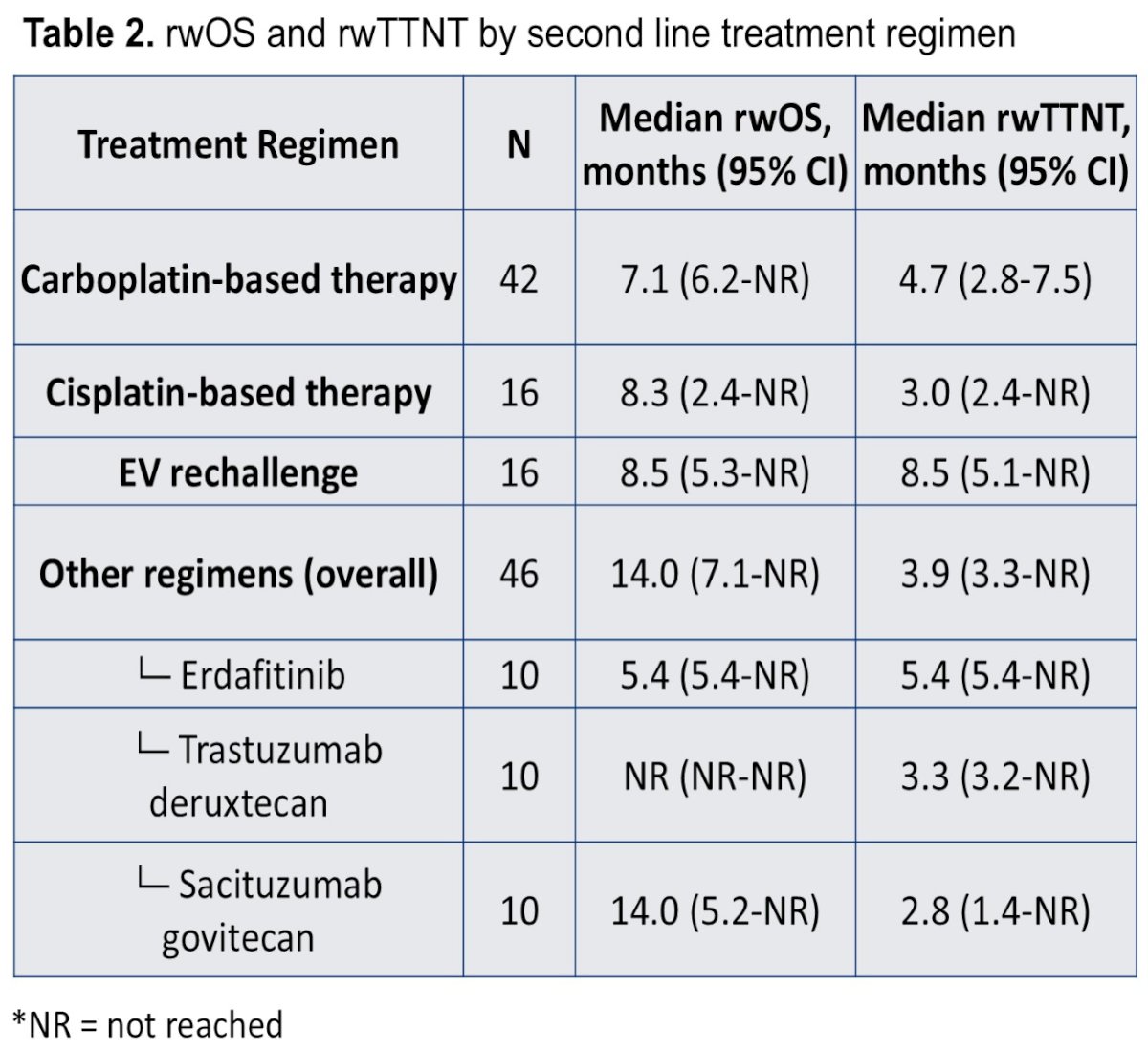
Kaplan–Meier analyses evaluated both real-world overall survival and real-world time to next therapy according to second-line treatment class. Median rwOS varied across treatment categories. Patients receiving carboplatin-based therapy had a median rwOS of 7.1 months, whereas those receiving cisplatin-based therapy had a median rwOS of 8.3 months. EV rechallenge demonstrated a median rwOS of 8.5 months. The longest median rwOS was observed in the heterogeneous “other regimens” category at 14.0 months, though this group included multiple targeted and antibody-drug conjugate therapies.
Real-world time to next therapy (rwTTNT) similarly demonstrated modest outcomes across treatment groups. Median rwTTNT was 4.7 months for carboplatin-based therapy, 3.0 months for cisplatin-based therapy, and 8.5 months for EV rechallenge. Among other regimens, rwTTNT was 3.9 months overall. Within targeted therapy subgroups, erdafitinib demonstrated a median rwTTNT of 5.4 months, trastuzumab deruxtecan 3.3 months, and sacituzumab govitecan 2.8 months.
Dr. Gebrael concluded as follows:
- This is the largest real-world study to date evaluating treatment patterns and outcomes with various second-line therapies after progression on first-line EV+pembro in aUC.
- Platinum-based therapies and targeted therapies are the most common second-line therapies.
- Median rwOS and rwTTNT were modest across all treatment groups.
- These findings highlight the limited efficacy of current second-line treatment options in the post EV+pembro setting, reveal the substantial heterogeneity of treatment patterns in clinical practice, and underscore the urgent need for development of novel therapies and sequencing studies in this setting.
- These results also provide survival estimates for future trial design and patient counseling.
Presented by: Georges Gebrael, MD, Resident Physician, Department of Internal Medicine, University of Utah, Salt Lake City, UT, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Reference:
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin plus pembrolizumab in previously untreated advanced urothelial cancer. N Engl J Med. 2024;390:875-888.