(UroToday.com) The 2026 ASCO GU Annual Symposium featured a prostate and urothelial cancers poster session. Dr. Pedro Barata presented an analysis evaluating survival outcomes among patients with metastatic bladder cancer in the United States using population-level data from the Surveillance, Epidemiology, and End Results (SEER) program.
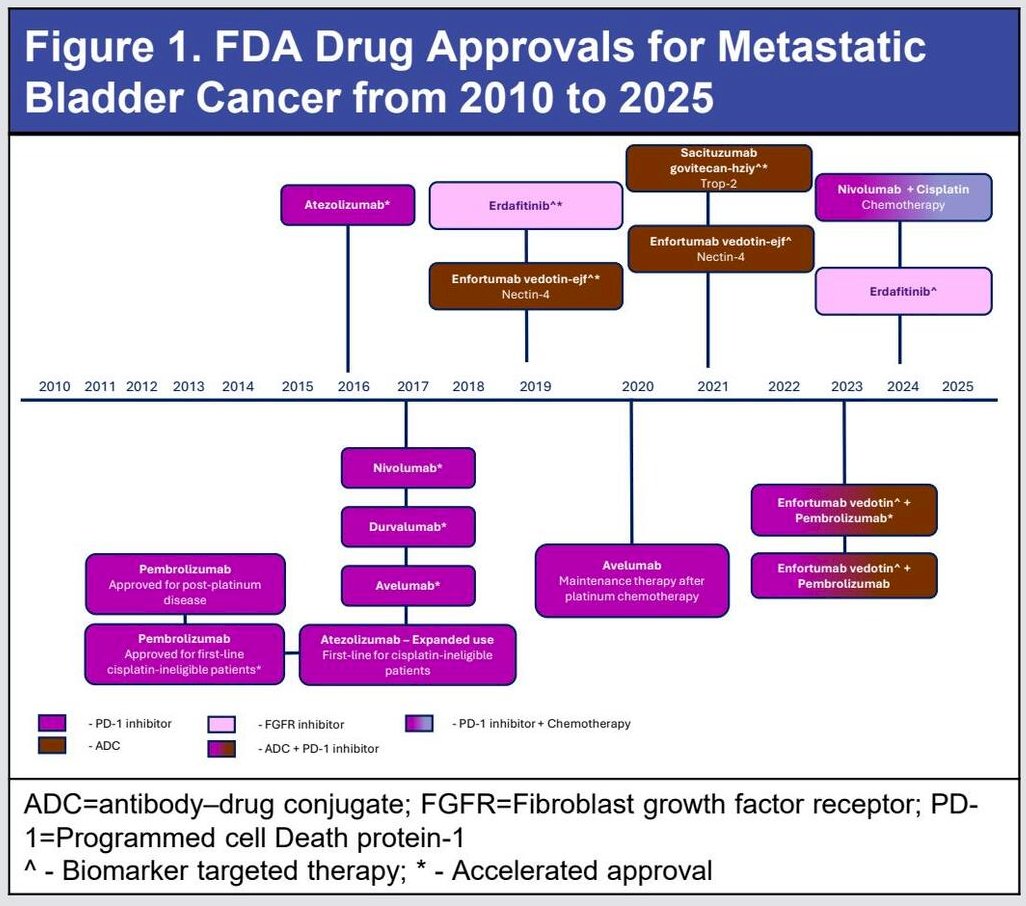
Bladder cancer is the 10th leading cause of cancer-related death in the United States.1 Over the past 15 years, multiple agents have been approved for the treatment of metastatic bladder cancer in the United States. However, the real-world impact of these therapies on survival outcomes remains incompletely characterized. The investigators therefore sought to evaluate overall survival trends and predictors of survival among patients diagnosed with metastatic bladder cancer in the United States.
This study was designed as a non-interventional retrospective cohort analysis using the SEER database. SEER collects cancer incidence and survival data from population-based cancer registries and includes routinely captured information on patient demographics, tumor characteristics, and follow-up for vital status.2 Data included in this analysis were derived from 22 geographic regions representing approximately 48% of the United States population.
Eligible patients were adults aged ≥18 years with primary diagnoses of bladder cancer between 2010 and 2021 and distant metastatic disease at presentation based on SEER staging definitions. Exclusion criteria included cases where bladder cancer was not the primary tumor, missing staging information, lack of follow-up data after diagnosis, or uncertain diagnostic data.
The investigators evaluated overall survival (OS) and bladder cancer–specific survival (CSS). OS was defined as the time from initial diagnosis of bladder cancer to death from any cause, with patients censored at last follow-up if death was not recorded. Bladder cancer–specific survival was determined using SEER cause-of-death classifications to distinguish cancer-related deaths from other causes. CSS was defined as the time from diagnosis to bladder cancer–specific death or last follow-up. Median survival and five-year survival rates were estimated. Predictors of survival were evaluated using multivariable Cox proportional hazards models adjusting for demographic and clinical covariates.
Relative survival estimates were also calculated, defined as the ratio of observed survival among cancer patients to the expected survival of a comparable general population cohort without cancer. Expected survival estimates were derived from U.S. life tables available through the National Center for Health Statistics and incorporated within SEER analytic tools.
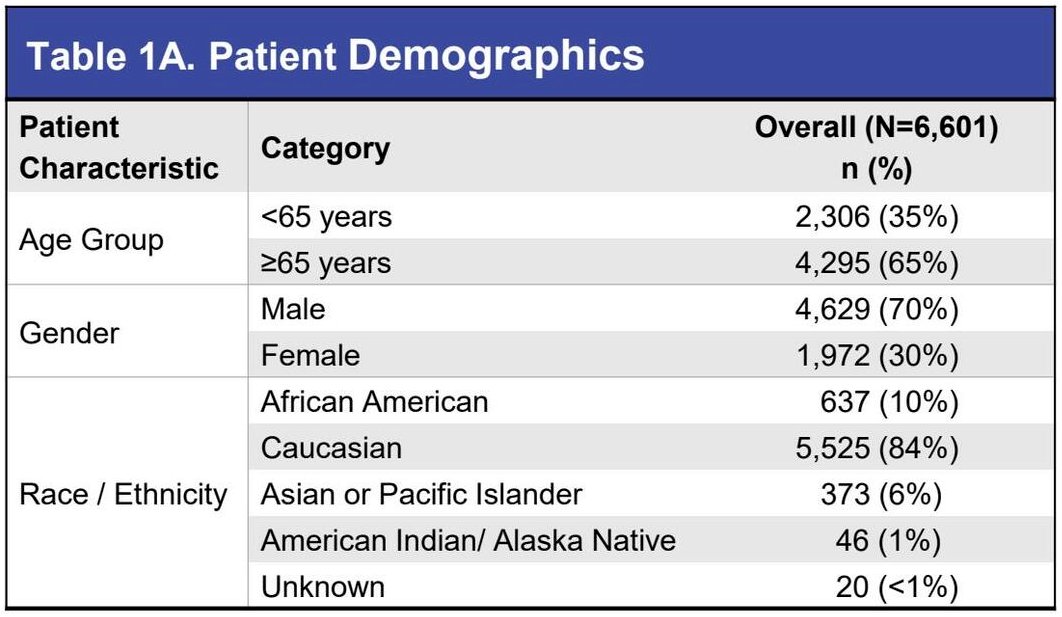
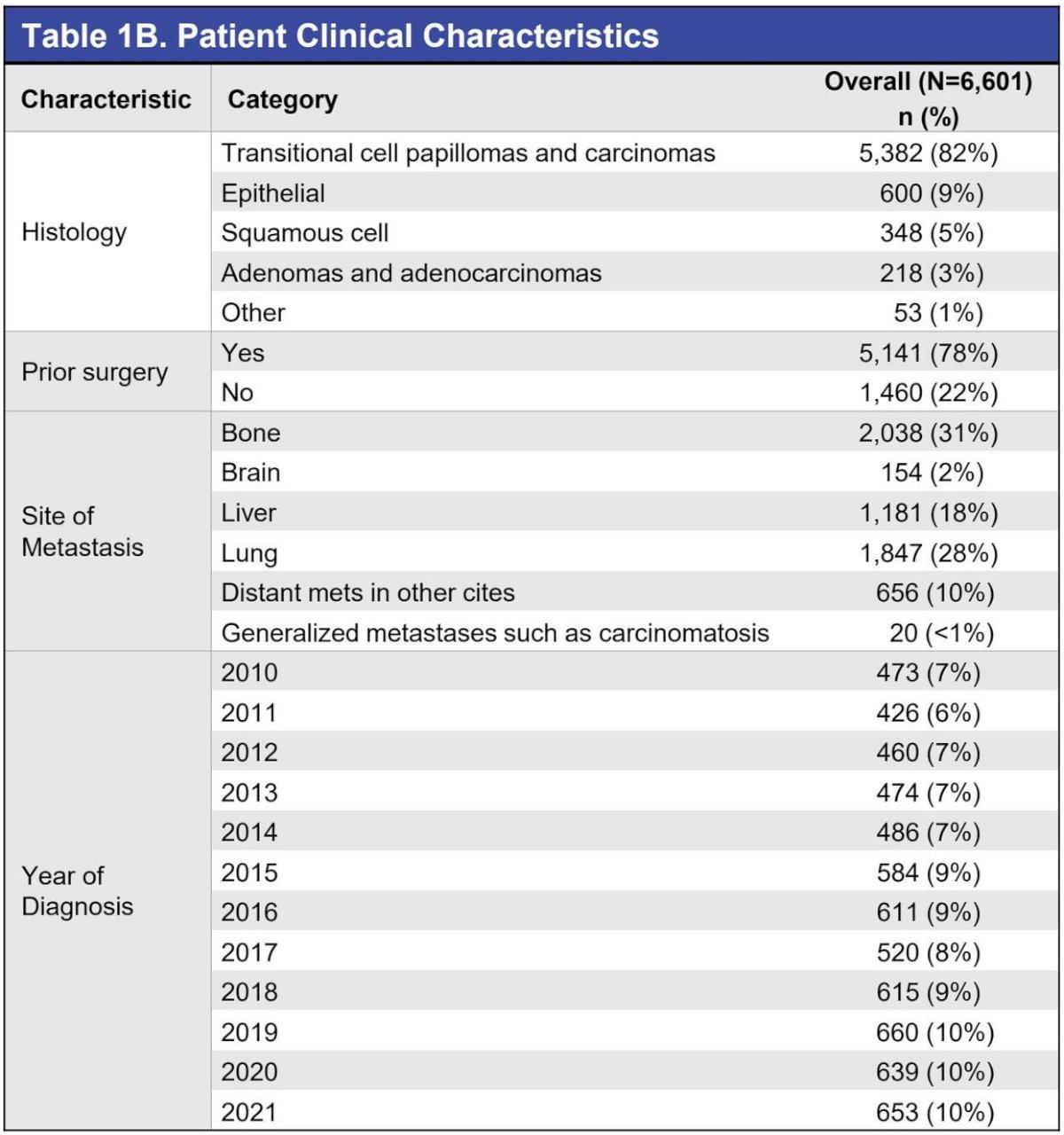
The analytic cohort included 6,601 patients diagnosed with metastatic bladder cancer. The majority of patients (65%) were aged ≥65 years at diagnosis, with a mean age of 69 years. Approximately 70% of the cohort were male. Most tumors were transitional cell carcinomas (82%), with smaller proportions representing squamous cell carcinoma, adenocarcinoma, and other histologic subtypes.
Metastatic disease sites included bone (31%), lung (28%), liver (18%), and brain (2%). Approximately 10% of patients presented with distant metastases involving other locations, and 7% had generalized metastatic disease including carcinomatosis. Prior bladder surgery had been performed in 78% of patients.
Across the overall cohort, the median overall survival was 7 months. The estimated five-year OS rate was 7%. Median bladder cancer–specific survival was 8 months, with a five-year CSS rate of 10%.
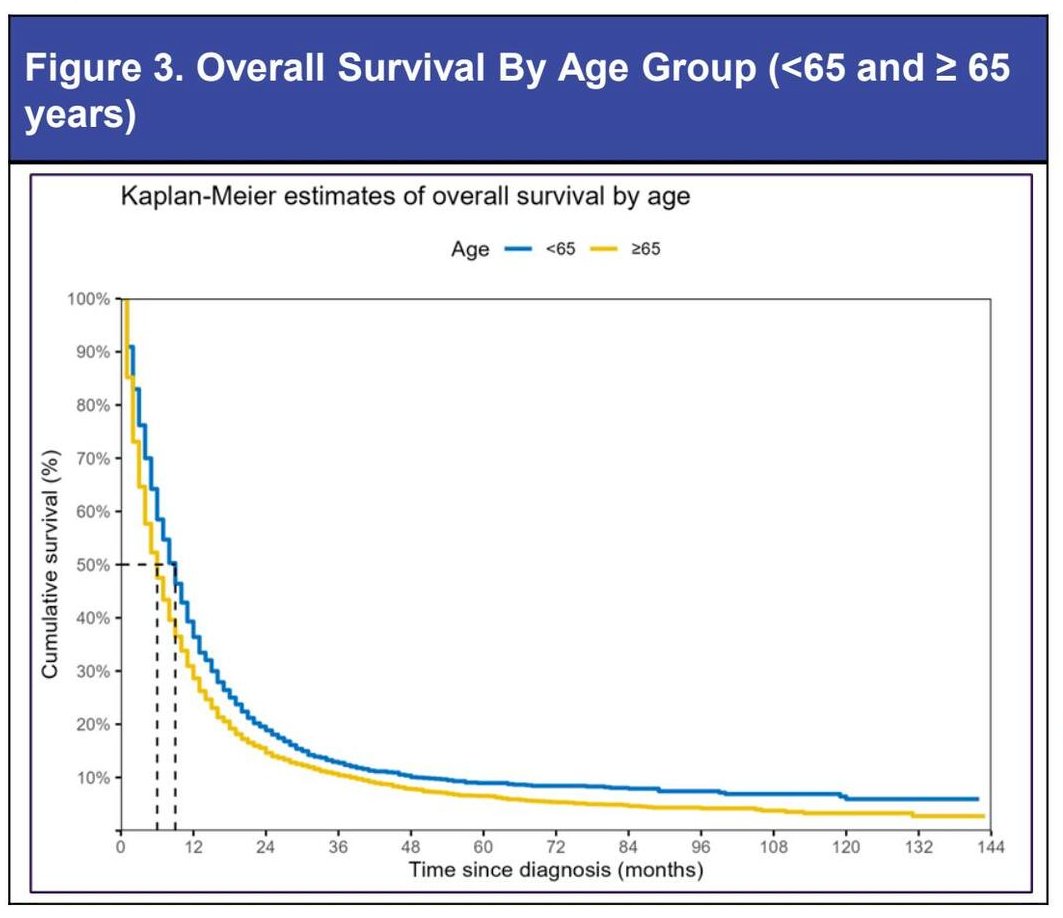
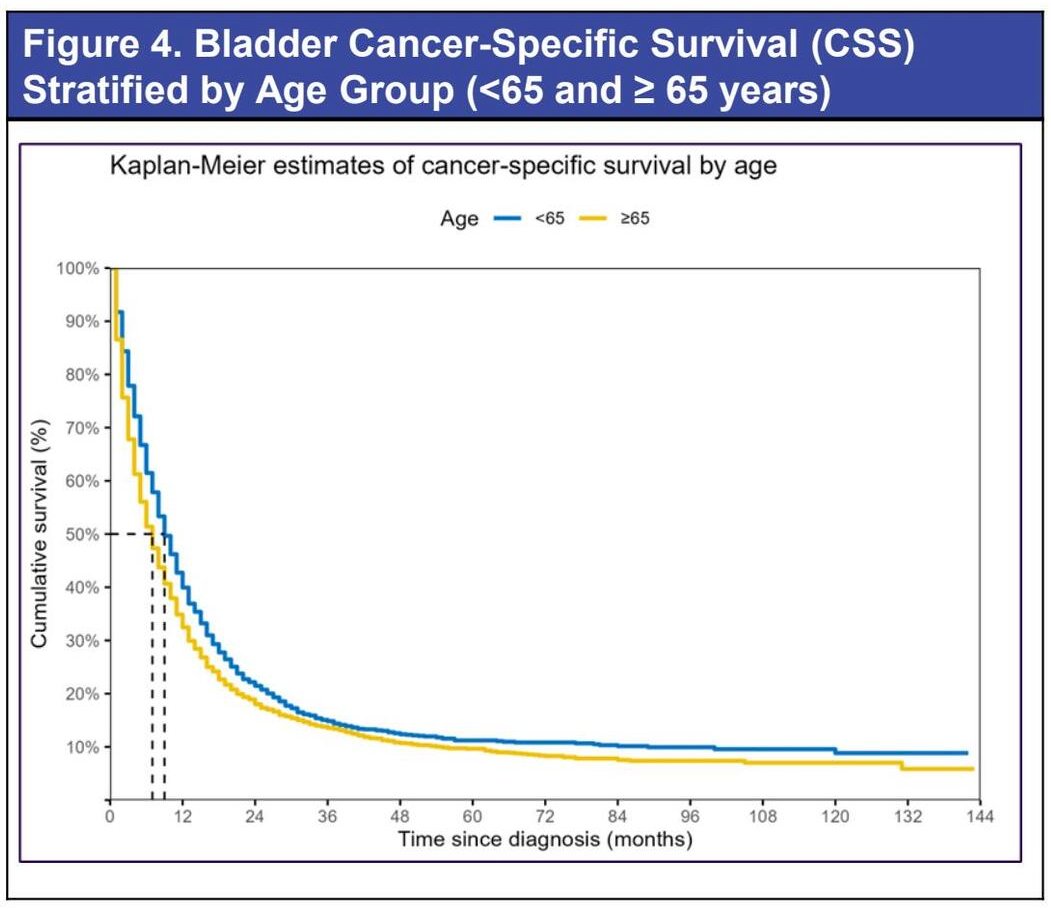
Age-specific analyses demonstrated meaningful differences in survival outcomes. Among patients younger than 65 years (n=2,306), the median OS and CSS were both 9 months, with corresponding five-year survival rates of 9% and 11%, respectively. In contrast, among patients aged ≥65 years (n=4,295), the median OS was 6 months, and the median CSS was 7 months, with five-year survival rates of 7% and 10%.
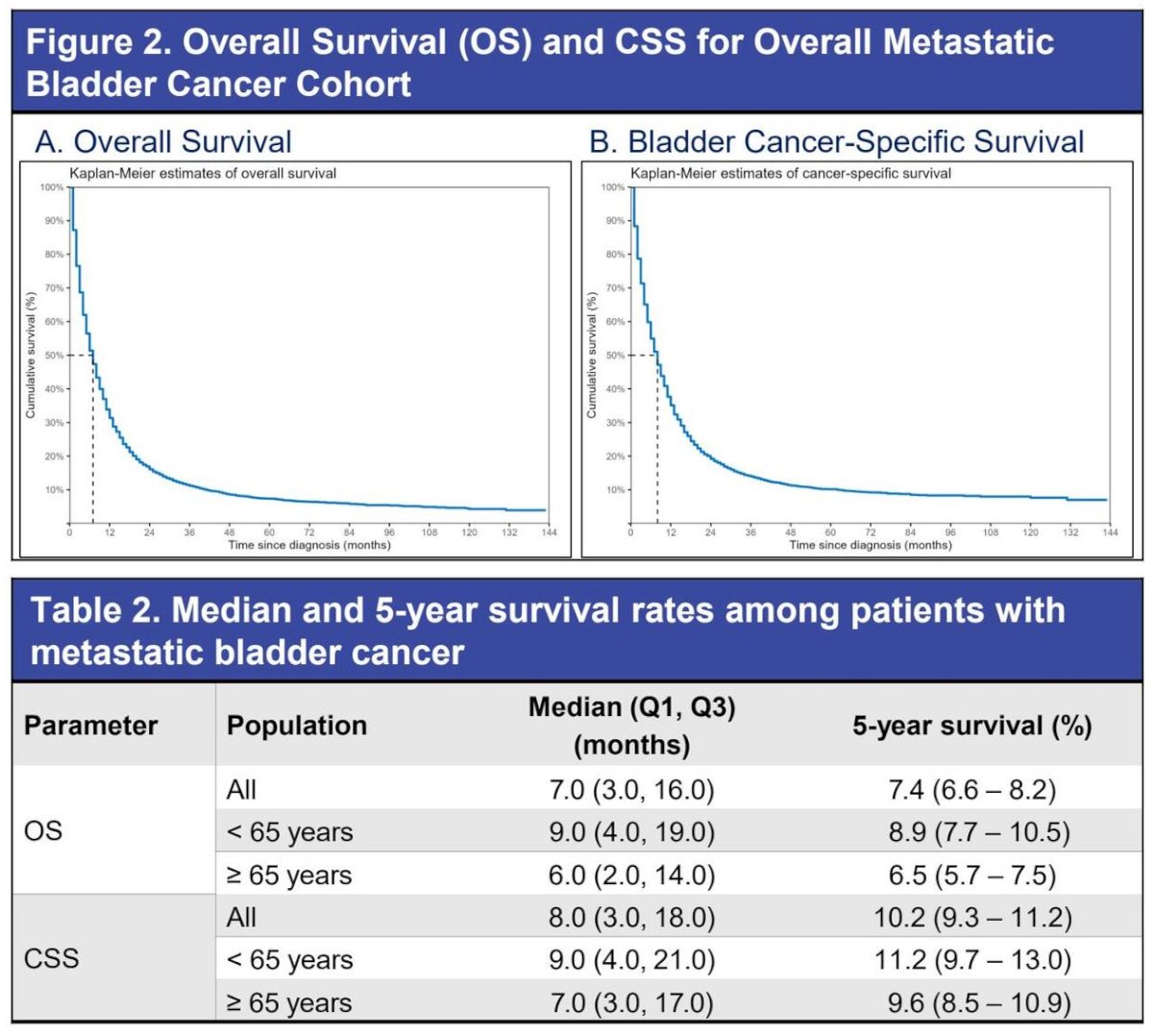
Kaplan–Meier survival curves demonstrated rapid early mortality following diagnosis, with the steepest decline occurring during the first 12–18 months after diagnosis. Survival curves plateaued thereafter, reflecting the small proportion of long-term survivors.
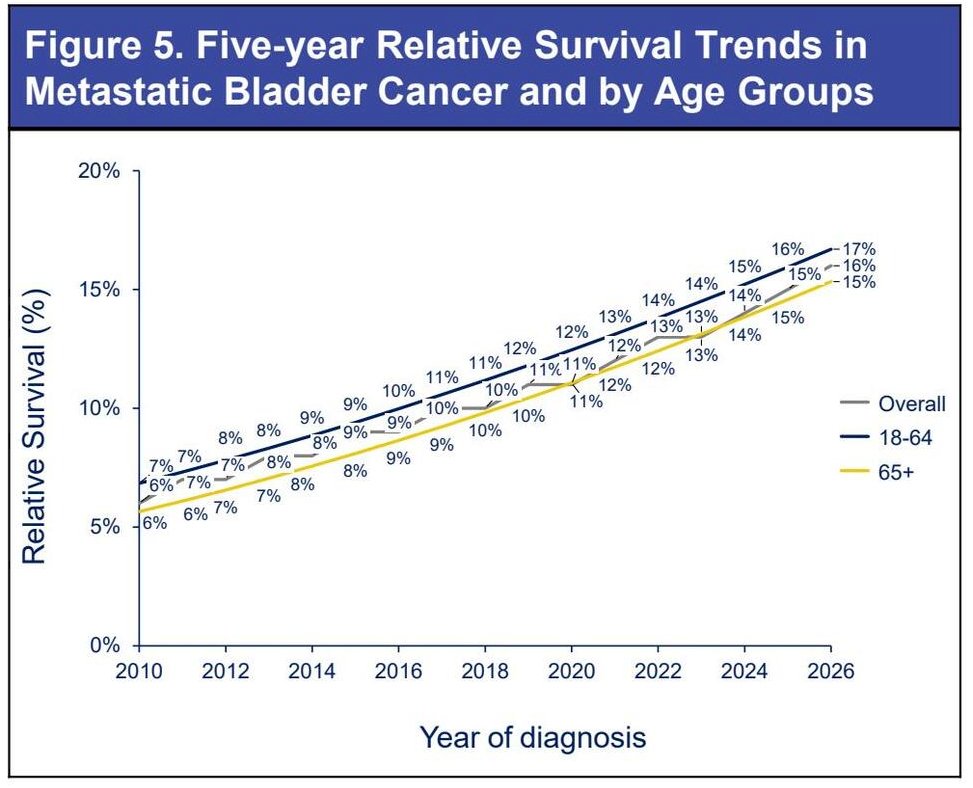
Temporal trends in relative survival were also evaluated. Five-year relative survival improved modestly over the study period, increasing from approximately 6% among patients diagnosed in 2010 to approximately 9% among those diagnosed in 2015 and reaching approximately 12% among patients diagnosed in 2021. These findings suggest incremental survival gains over time, potentially reflecting the introduction of novel systemic therapies for metastatic bladder cancer.
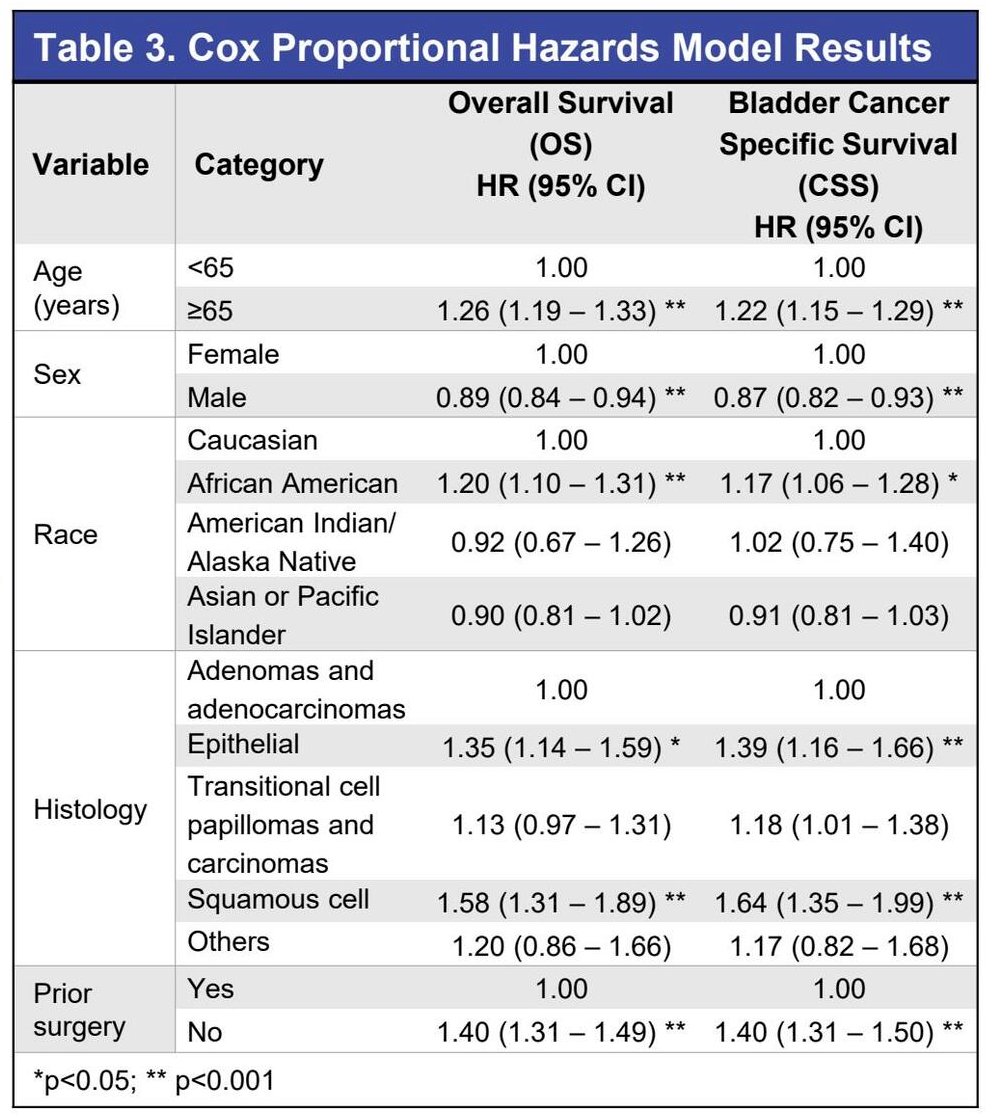
Multivariable Cox proportional hazards modeling identified several independent predictors of both OS and CSS.
Older age (≥65 years) was significantly associated with worse outcomes. Compared with patients <65 years, those ≥65 had inferior OS (HR 1.26, 95% CI 1.19–1.33) and CSS (HR 1.22, 95% CI 1.15–1.29), confirming the adverse prognostic impact of age in metastatic bladder cancer.
Sex also demonstrated a statistically significant association with survival. Female sex was associated with modestly improved outcomes compared with males, with lower risk of death for OS (HR 0.89, 95% CI 0.84–0.94) and CSS (HR 0.87, 95% CI 0.82–0.93).
Race was independently associated with survival differences. African American patients had worse outcomes compared with Caucasian patients for OS (HR 1.20, 95% CI 1.10–1.31) and CSS (HR 1.17, 95% CI 1.06–1.28). In contrast, Asian/Pacific Islander patients had improved OS (HR 0.92, 95% CI 0.67–1.26) and CSS (HR 0.91, 95% CI 0.81–1.03), although the confidence intervals for OS crossed unity.
Histology was also prognostic. Compared with adenocarcinoma (reference), epithelial histology was associated with worse OS (HR 1.35, 95% CI 1.14–1.59) and CSS (HR 1.39, 95% CI 1.16–1.66). Transitional cell carcinoma demonstrated similar adverse associations for OS (HR 1.13, 95% CI 0.97–1.31) and CSS (HR 1.18, 95% CI 1.01–1.38), while squamous cell carcinoma conferred even greater risk for OS (HR 1.58, 95% CI 1.31–1.89) and CSS (HR 1.64, 95% CI 1.35–1.99).
Importantly, absence of prior bladder surgery was strongly associated with worse survival. Patients without prior surgery had significantly higher risk of death for both OS (HR 1.40, 95% CI 1.31–1.49) and CSS (HR 1.40, 95% CI 1.31–1.50), suggesting that surgical history may serve as a surrogate for disease biology, patient selection, or earlier-stage disease at initial presentation.
Dr. Barata acknowledged the following study limitations:
- Detailed information on treatment and related dosing is not available within SEER.
- Observed survival trends might not reflect recently approved treatments for metastatic bladder cancer.
He concluded as follows:
- Gains in long-term survival suggest incremental benefits from newer therapies. While clinically meaningful strides have been made in the treatment of metastatic bladder cancer over the past decade, there remains opportunity to further advance treatment.
- Continued development of novel agents, especially for subgroups with poor prognosis, is needed to achieve more meaningful improvements
Presented by: Pedro C. Barata, MD, MSc, Associate Professor at University Hospitals Seidman Cancer Center, Cleveland, OH
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.