(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Steffen Rausch discussing pathological outcomes and disease-free survival in KEYNOTE-905, assessing neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab in participants with muscle-invasive bladder cancer who are cisplatin-ineligible.
The phase 3 KEYNOTE-905/EV-303 study previously showed significantly improved event-free survival, overall survival, and pathological complete response rate with neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab added to radical cystectomy with pelvic lymph node dissection in patients with muscle-invasive bladder cancer who were cisplatin-ineligible. At ASCO GU 2026, Dr. Rausch and colleagues reported pathological outcomes and disease-free survival in this study.
Patients with T2-T4aN0M0 or T1-T4aN1M0 muscle-invasive bladder cancer ineligible for or declining cisplatin were randomized 1:1 to enfortumab vedotin + pembrolizumab (3 cycles neoadjuvant enfortumab vedotin 1.25 mg/kg on day 1 and 8 + pembrolizumab 200 mg on day 1, radical cystectomy + pelvic lymph node dissection, and adjuvant 6 cycles enfortumab vedotin + 14 cycles pembrolizumab) versus control (radical cystectomy + pelvic lymph node dissection only):
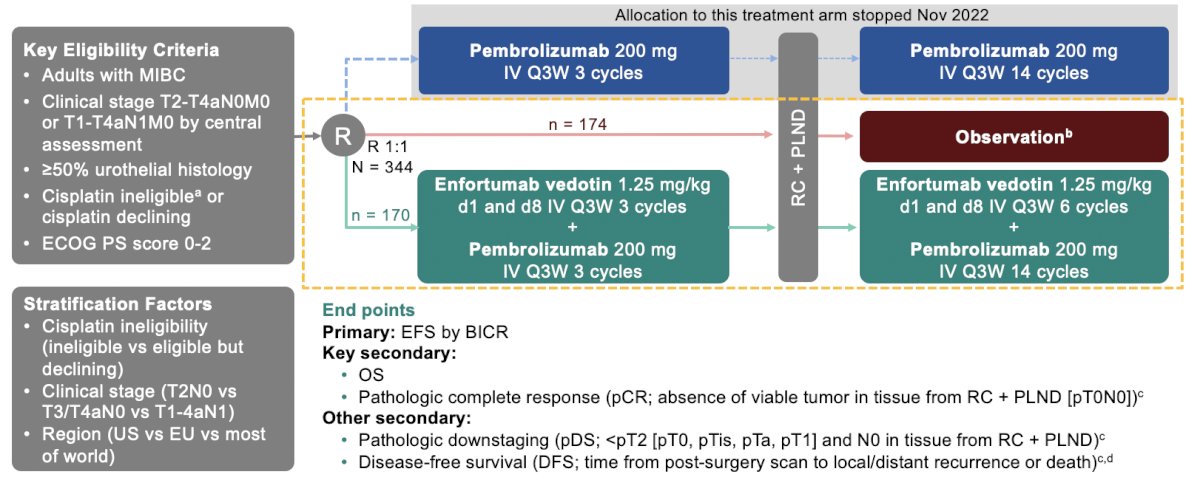
Pathological complete response (absence of viable tumor in tissue from radical cystectomy + pelvic lymph node dissection [pT0N0]) rate was a key secondary endpoint, and pathological downstaging (< pT2 [pT0, pTis, pTa, pT1] and N0) rate and disease free survival (time from post-surgery scan to local/distant recurrence or death) were secondary endpoints, all assessed by central pathology review or blinded independent central review. Patients were considered disease-free after radical cystectomy + pelvic lymph node dissection for disease-free survival analysis if they had a complete resection (no gross residual disease) and no evidence of disease on a post-surgery scan.
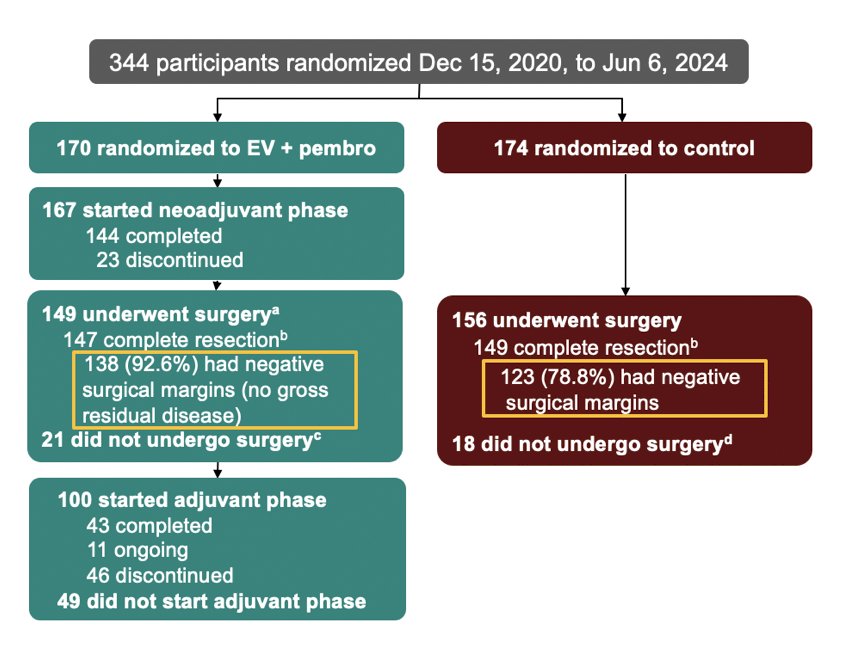
As of June 6, 2025, the median follow-up was 25.6 months (range: 11.8–53.7). In the enfortumab vedotin + pembrolizumab versus control arms, 149/170 patients (87.6%) and 156/174 (89.7%) underwent surgery, 147/149 (98.7%) and 149/156 (95.5%) had complete resection, and 138/149 (92.6%) and 123/156 (78.8%) had negative surgical margins:
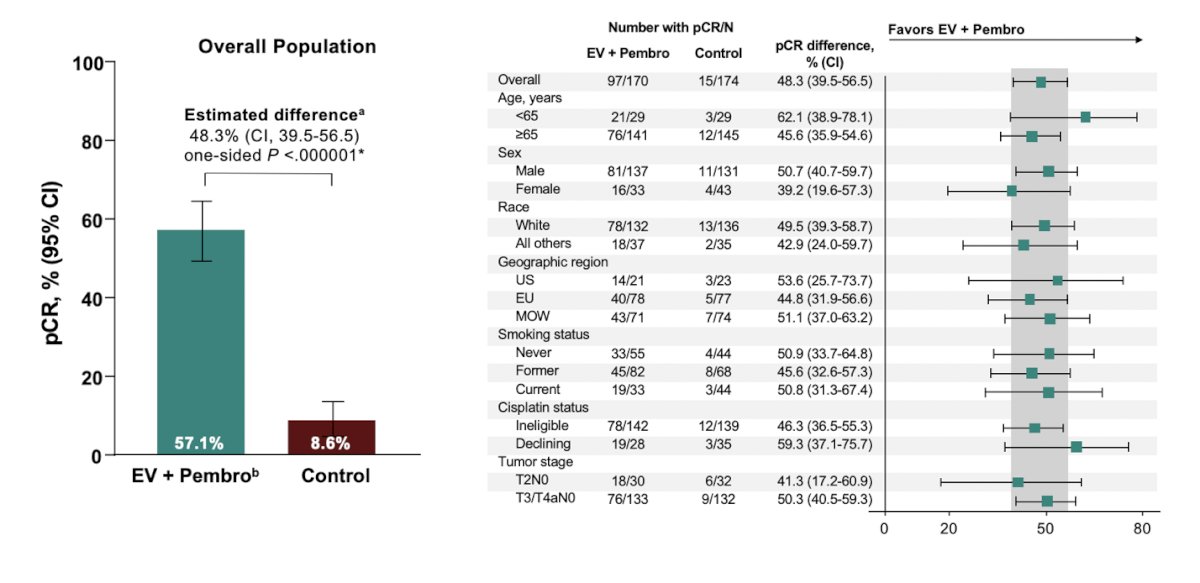
The previously reported pathological complete response rate for all patients in the enfortumab vedotin + pembrolizumab versus control arms was 57.1% versus 8.6%, respectively, with an estimated difference of 48.3% (95% CI 39.5–56.5; p < 0.001):
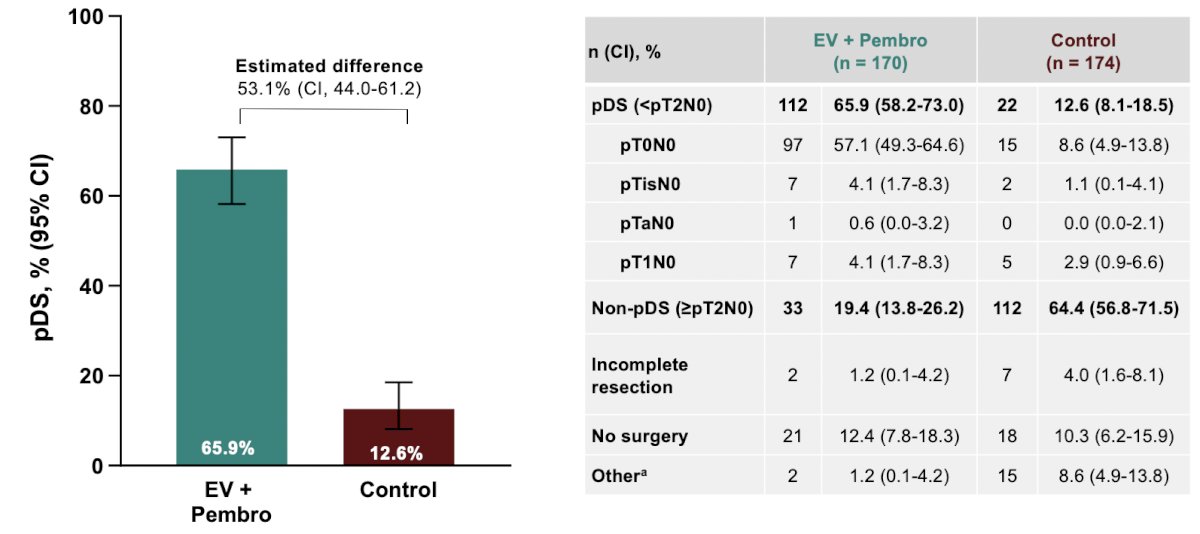
Pathological downstaging rate was higher with enfortumab vedotin + pembrolizumab versus control (65.9% versus 12.6%; estimated difference 53.1%; 95% CI 44.0–61.2):
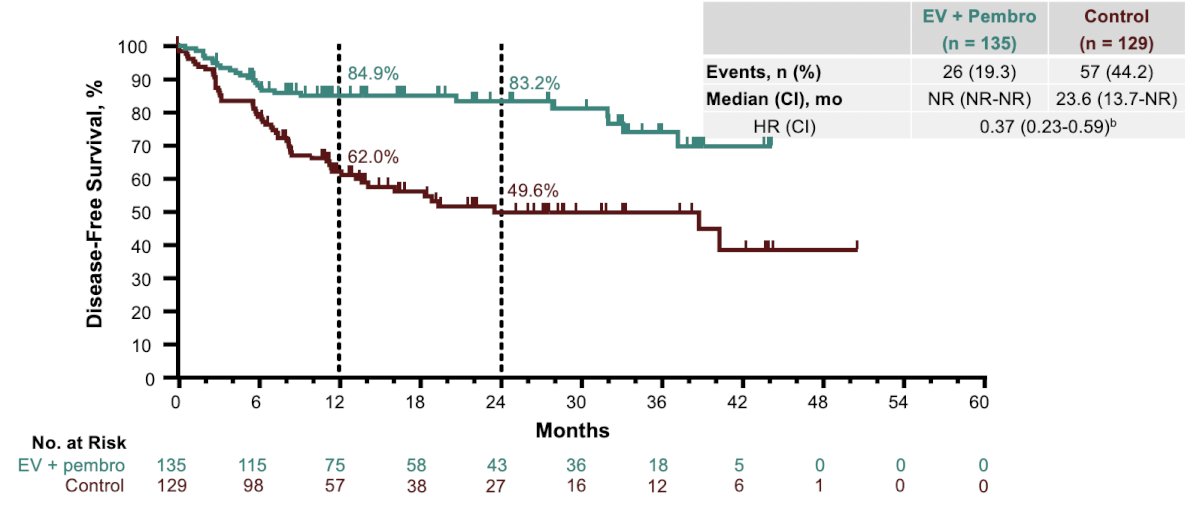
Among patients evaluated for disease-free survival (n = 135 in enfortumab vedotin + pembrolizumab arm; n = 129 in control arm), the median disease-free survival was not reached versus 23.6 months (HR 0.37, 95% CI 0.23–0.59):
Additionally, the disease-free survival benefits were noted across all subgroups:

Dr. Rausch concluded his presentation discussing pathological outcomes and disease-free survival in KEYNOTE-905 with the following take-home points:
- Pathological outcomes and disease-free survival favored neoadjuvant-adjuvant enfortumab vedotin + pembrolizumab and radical cystectomy + pelvic lymph node dissection compared with radical cystectomy + pelvic lymph node dissection alone, supporting the primary results of KEYNOTE-905
- Negative surgical margins: 92.6% versus 78.8%
- Pathological complete response rate: 57.1% versus 8.6%; estimated difference 48.3% (95% CI 39.5-56.5; p < 0.001), generally consistent across subgroups
- Pathological downstaging rate: 65.9% versus 12.6%; estimated difference 53.1%; (95% CI, 44.0-61.2)
- Disease-free survival: median disease-free survival was not reached versus 23.6 months (HR 0.37, 95% CI 0.23-0.59)
- Per previous reports, the safety profile of neoadjuvant-adjuvant enfortumab vedotin + pembrolizumab was manageable and consistent with that of this regimen in the locally advanced/metastatic urothelial carcinoma setting
- These findings further establish neoadjuvant-adjuvant enfortumab vedotin + pembrolizumab as a standard-of-care treatment option for patients with muscle-invasive bladder cancer who are cisplatin ineligible, addressing a key unmet clinical need
KEYNOTE-905 was published in the New England Journal of Medicine several days ago.
Presented by: Steffen Rausch, MD, Eberhard-Karls-University, Tuebingen, Germany