(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Xinan Sheng discussing updated results from the phase II RC48-C017 trial assessing neoadjuvant treatment with disitamab vedotin + perioperative toripalimab in patients with HER2-expressing muscle-invasive bladder cancer. Disitamab vedotin (a HER2-targeted antibody-drug conjugate with monomethyl auristatin E as the payload) in combination with toripalimab (a PD-1 inhibitor) has demonstrated significant and clinically meaningful improvement in both progression-free survival and overall survival in patients with untreated, HER2-expressing, advanced urothelial cancer in the phase III RC48-C016 study.1
However, its efficacy in the early-stage disease setting is not fully explored. The single-arm phase II RC48-C017 trial evaluated the efficacy and safety of the combination of disitamab vedotin and toripalimab in patients with HER2-expressing muscle-invasive bladder cancer in the perioperative setting. The previous analysis showed a pathological complete response rate of 63.6% in the surgical patients, and manageable safety (ASCO GU 2025). At ASCO GU 2026, Dr. Sheng and colleagues reported updated results with a longer follow-up (data cutoff: August 14, 2025), including event-free survival, overall survival, and safety.
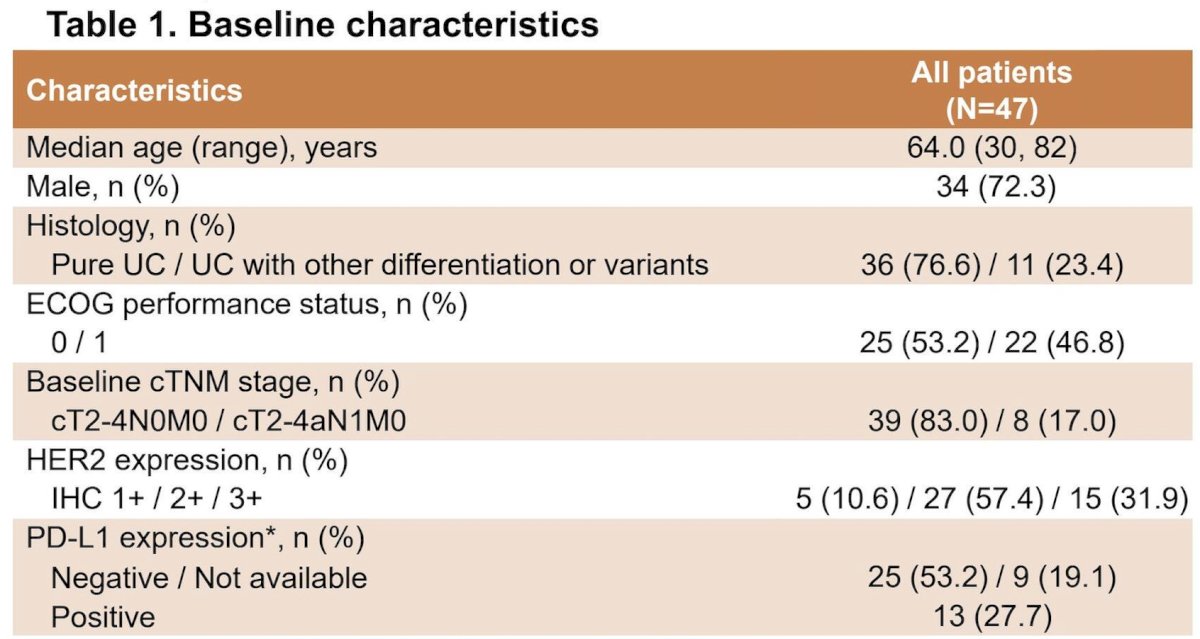
This study enrolled patients with previously untreated muscle-invasive bladder cancer (cT2-4aN0-1M0) with locally confirmed HER2 expression (defined as immunohistochemistry [IHC] ≥1+). All patients must be eligible for and plan to undergo curative-intent radical cystectomy and pelvic lymph node dissection. Eligible patients received 6 cycles of disitamab vedotin (2 mg/kg, once every 2 weeks [Q2W]) plus toripalimab (3 mg/kg Q2W) at the neoadjuvant phase. After radical cystectomy and pelvic lymph node dissection, patients received 20 cycles of adjuvant toripalimab (3 mg/kg Q2W):
![This study enrolled patients with previously untreated muscle-invasive bladder cancer (cT2-4aN0-1M0) with locally confirmed HER2 expression (defined as immunohistochemistry [IHC] ≥1+). All patients must be eligible for and plan to undergo curative-intent radical cystectomy and pelvic lymph node dissection. Eligible patients received 6 cycles of disitamab vedotin (2 mg/kg, once every 2 weeks [Q2W]) plus toripalimab (3 mg/kg Q2W) at the neoadjuvant phase. After radical cystectomy and pelvic lymph node dissection, patients received 20 cycles of adjuvant toripalimab (3 mg/kg Q2W):](/images/com-doc-importer/248-asco-gu-2026/asco-gu-2026-neoadjuvant-treatment-with-disitamab-vedotin-perioperative-toripalimab-in-patients-with-her2-expressing-mibc-in-the-phase-ii-rc48-c017-trial-updated-results/image-0.jpg)
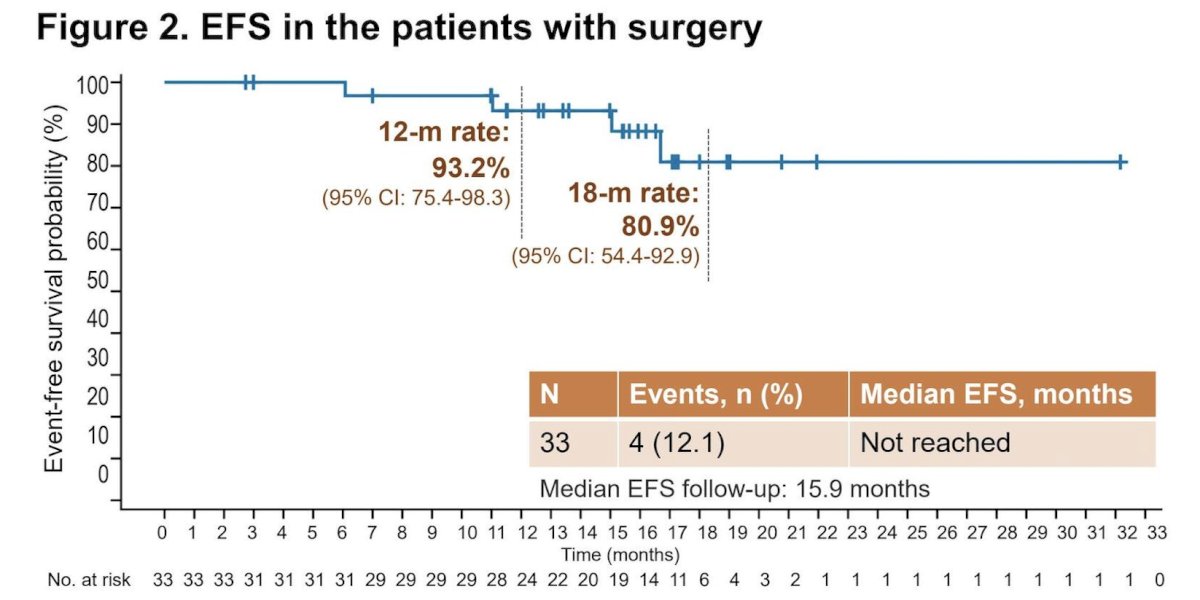
A total of 47 patients were enrolled and treated, with the majority (83.0%) at T2-4N0M0 stage. Radical cystectomy and pelvic lymph node dissection were performed in 33 patients. As of data cutoff, the median follow-up was 26.4 (95% CI: 24.4-28.2) months:
The median event-free survival was not reached. At 12 and 18 months, the event-free survival rate was 93.2% (95% CI: 75.4-98.3) and 80.9% (54.4-92.9), respectively, in patients who underwent surgery:
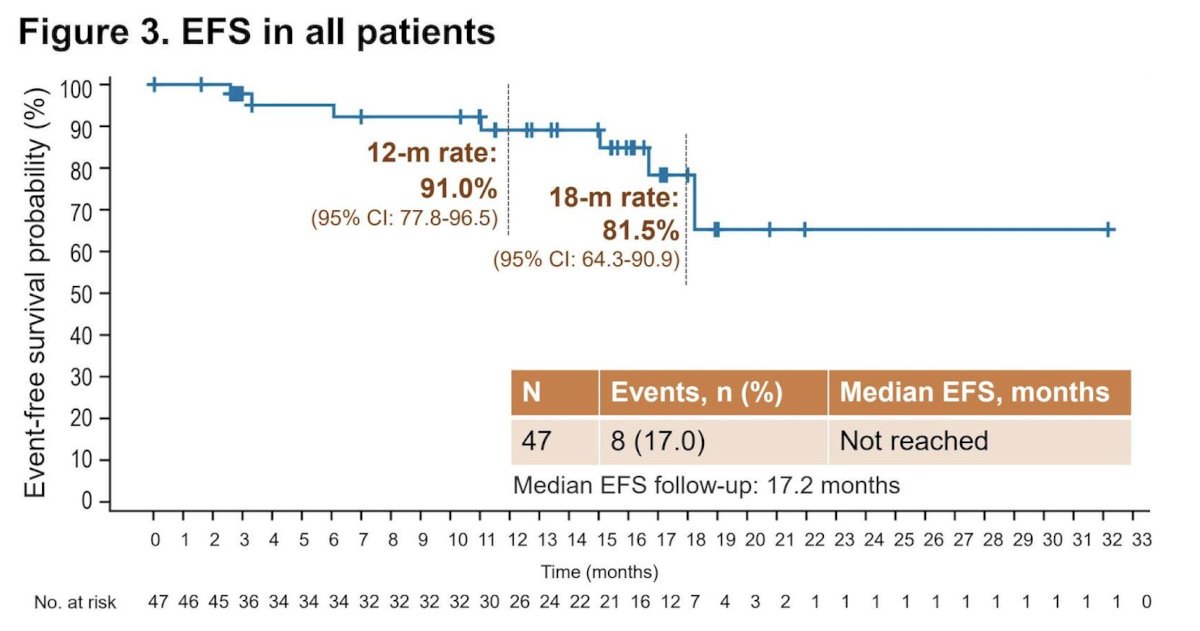
At 12 and 18 months, the event-free survival rate was 91.0% (77.8-96.5) and 81.5% (64.3-90.9), respectively, in all patients:
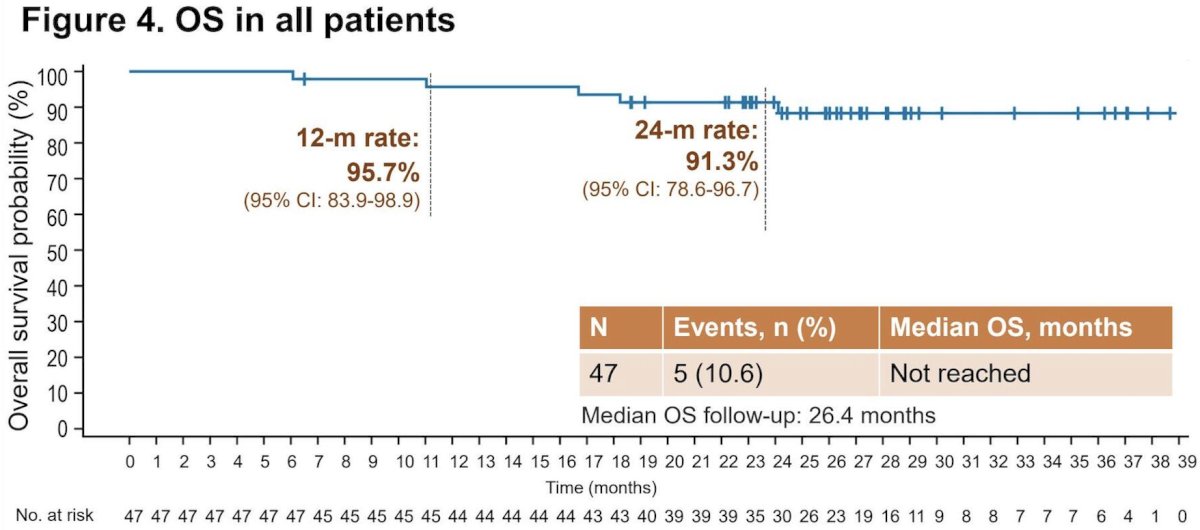
The median overall survival was not reached, and the 12- and 24-month overall survival rates were 95.7% (95% CI 83.9-98.9) and 91.3% (95% CI 78.6-96.7), respectively:
No new safety signals were observed.
Dr. Sheng concluded this presentation discussing updated results from the phase II RC48-C017 trial with the following take-home points:
- These updated data demonstrated that the initial treatment response has translated into a durable long-term disease control and survival, as evidenced by the event-free survival and overall survival outcomes
- This sustained treatment effect of neoadjuvant disitamab vedotin + perioperative toripalimab in patients with HER2-expressing muscle invasive bladder cancer in the perioperative setting deserves further evaluation in pivotal clinical studies
Presented by: Xinan Sheng, MD, Peking University Cancer Hospital & Institute, Beijing, China
Reference:
- Sheng X, Zeng G, Zhang C, et al. Disitamab Vedotin plus Toripalimab in HER2-Expressing Advanced Urothelial Cancer. N Engl J Med. 2025 Dec 11;393(23):2324-2337