(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Joaquim Bellmunt discussing an exploratory analysis of ctDNA dynamics in the IMvigor011 trial. In the randomized, double-blind, Phase 3 IMvigor011 trial, ctDNA-guided adjuvant atezolizumab led to statistically significant improvements in investigator assessed disease free survival and overall survival versus placebo after radical cystectomy in patients with muscle invasive bladder cancer:1
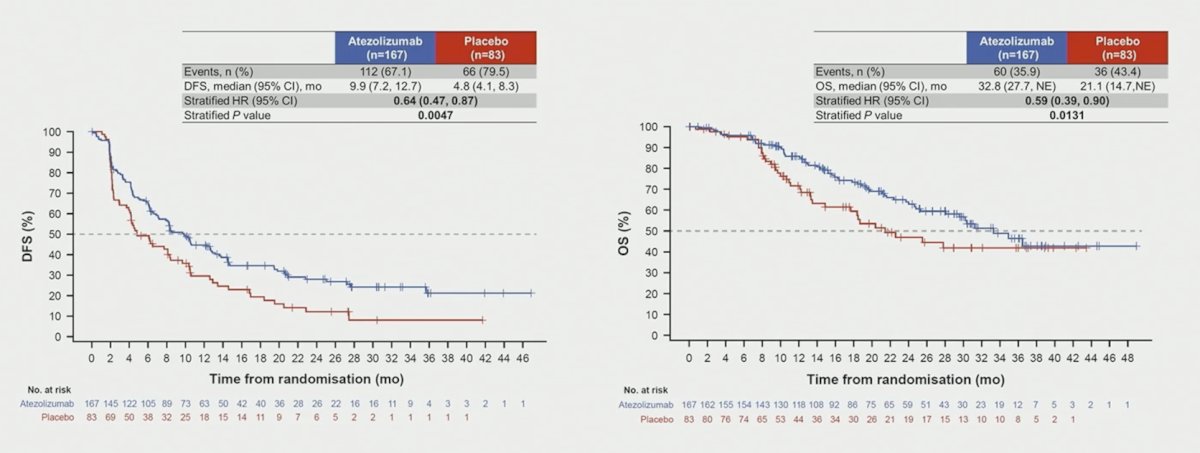
A higher proportion of patients in the atezolizumab arm cleared ctDNA at either cycle 3 or cycle 5, and all patients in the placebo arm who cleared ctDNA had low baseline concentrations [1]. At ASCO GU 2026, Dr. Bellmunt and colleagues reported exploratory analyses of ctDNA timing and concentration in ctDNA-positive patients in surveillance, and on-treatment ctDNA dynamics in randomized patients, including correlation with clinical outcomes.
Patients with muscle invasive bladder cancer and no radiographic disease were enrolled in surveillance within 6–24 weeks of radical cystectomy. Serial ctDNA monitoring was done every 6 weeks with imaging every 12 weeks for up to 1 year post-radical cystectomy. Patients who tested ctDNA positive at any time were screened for the treatment phase:
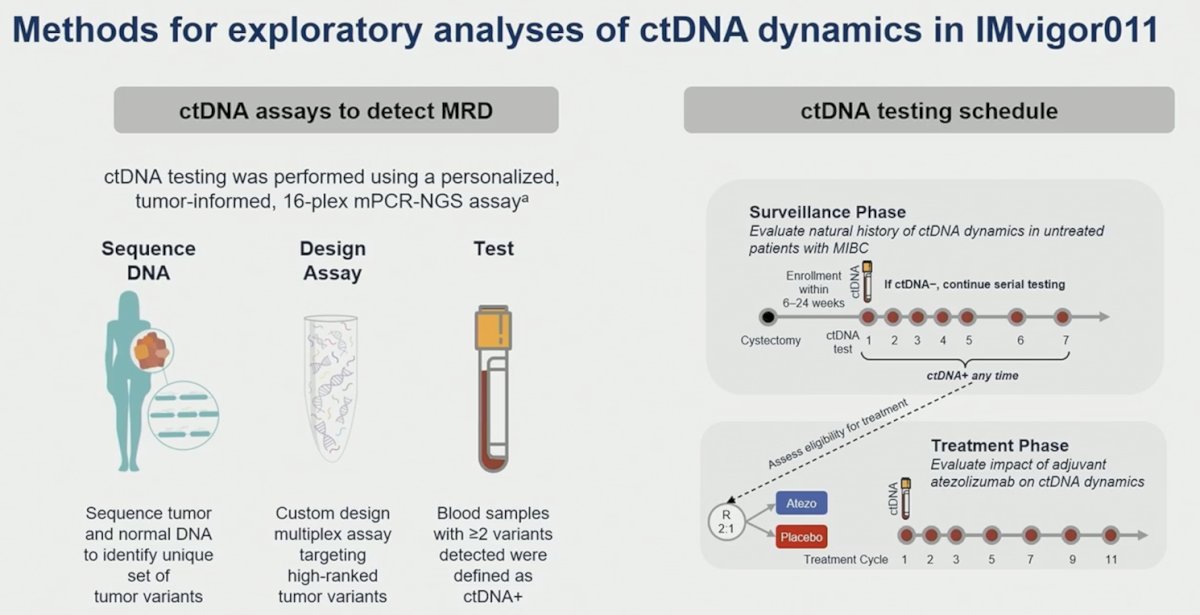
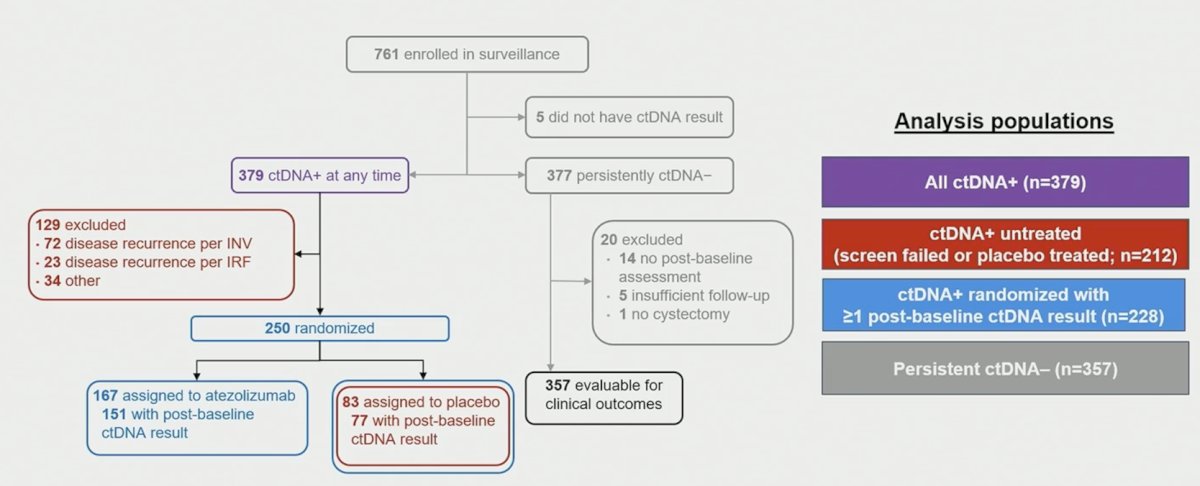
Eligible patients were randomized 2:1 to atezolizumab or placebo every 4 weeks for 12 cycles or up to 1 year. Time to first ctDNA positive result and baseline ctDNA concentration were assessed in all patients who tested ctDNA positive during surveillance (n = 379), and correlation with investigator assessed disease free survival was evaluated in patients who did not receive active adjuvant treatment (n = 212). On-treatment ctDNA dynamics, including association with investigator assessed disease free survival and overall survival, were evaluated in patients who received ≥1 dose of atezolizumab (n = 165) or placebo (n = 83). The consort diagram and analysis populations for this study are as follows:
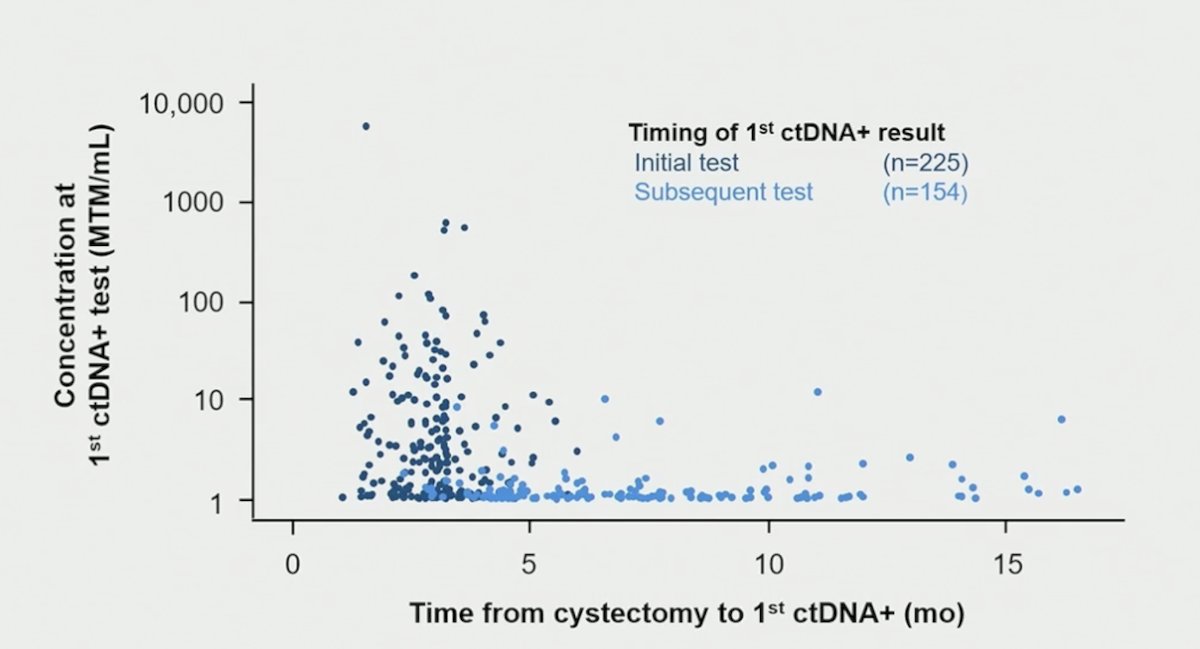
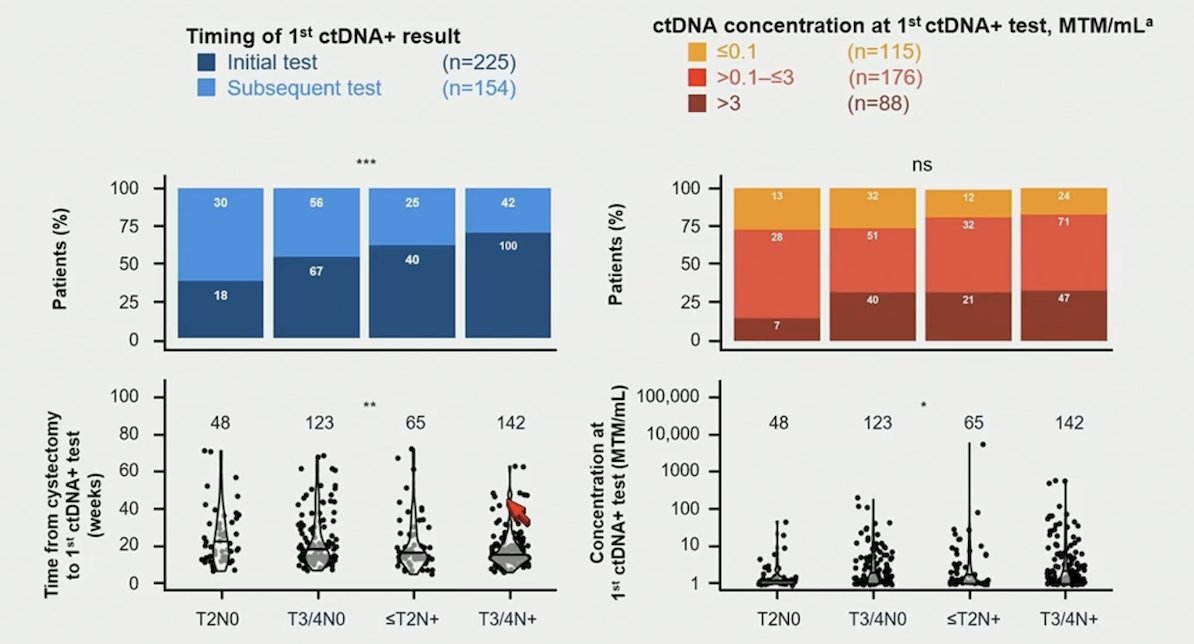
In patients who tested ctDNA positive during surveillance, the concentration of ctDNA at time of first positive test ranged from 0.01–613.8 mean tumor molecules/mL (median, 0.27 mean tumor molecules/mL). The majority of patients (n = 281, 74.1%) tested ctDNA positive within 24 weeks of radical cystectomy. In IMvigor011, late conversion to ctDNA positive status was associated with lower ctDNA concentration:
Pathology alone was insufficient to predict ctDNA timing or concentration. High risk pathological stage was associated with earlier time to positivity and high concentration. However, variability within pathological risk groups was greater than variability between them:
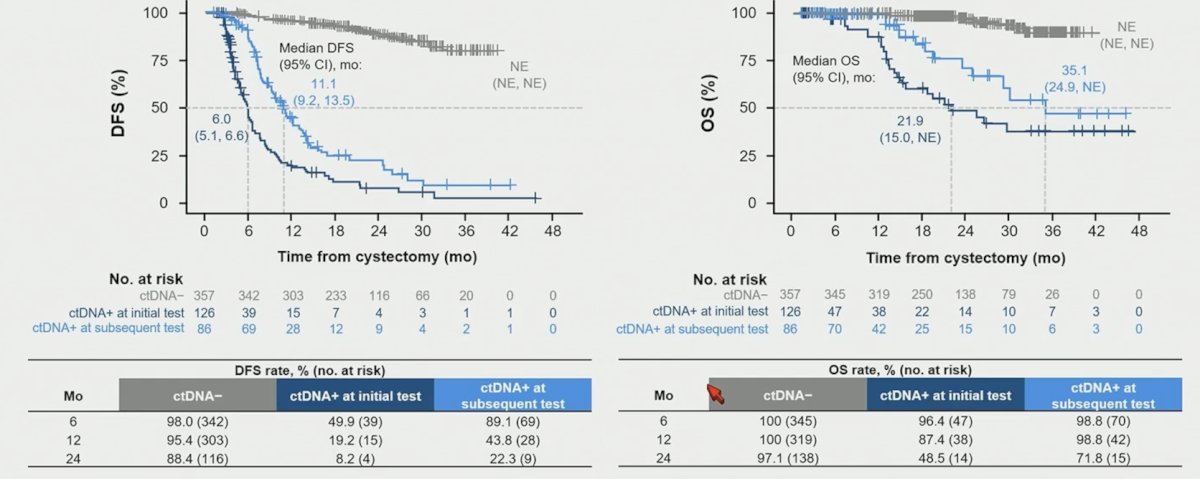
Timing of ctDNA positivity provided prognostic information beyond binary ctDNA status in untreated patients, in that early ctDNA positivity was associated with inferior clinical outcomes:
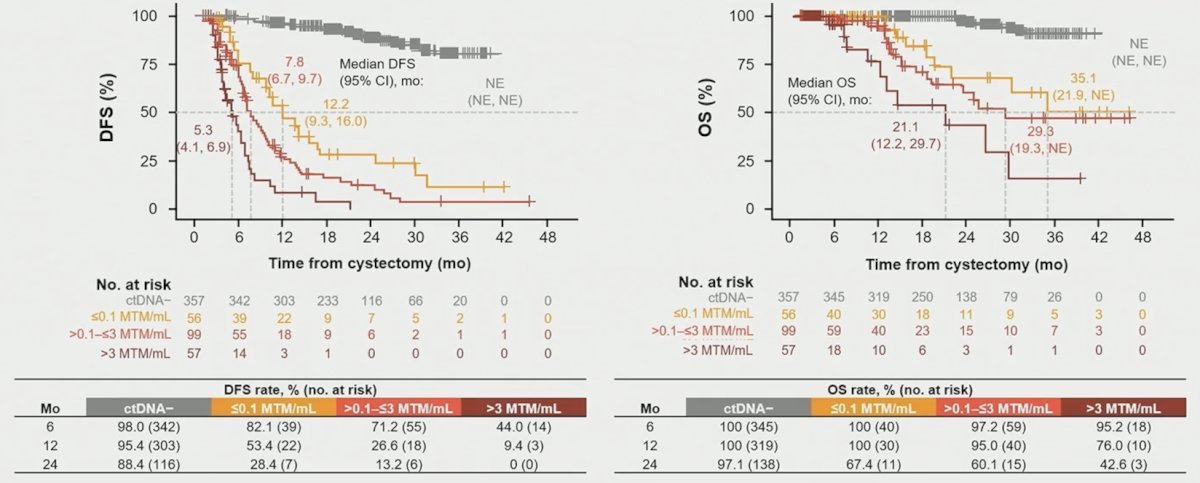
Additionally, ctDNA concentration provided prognostic information beyond binary ctDNA status in untreated patients, in that high ctDNA concentration was associated with inferior clinical outcomes:
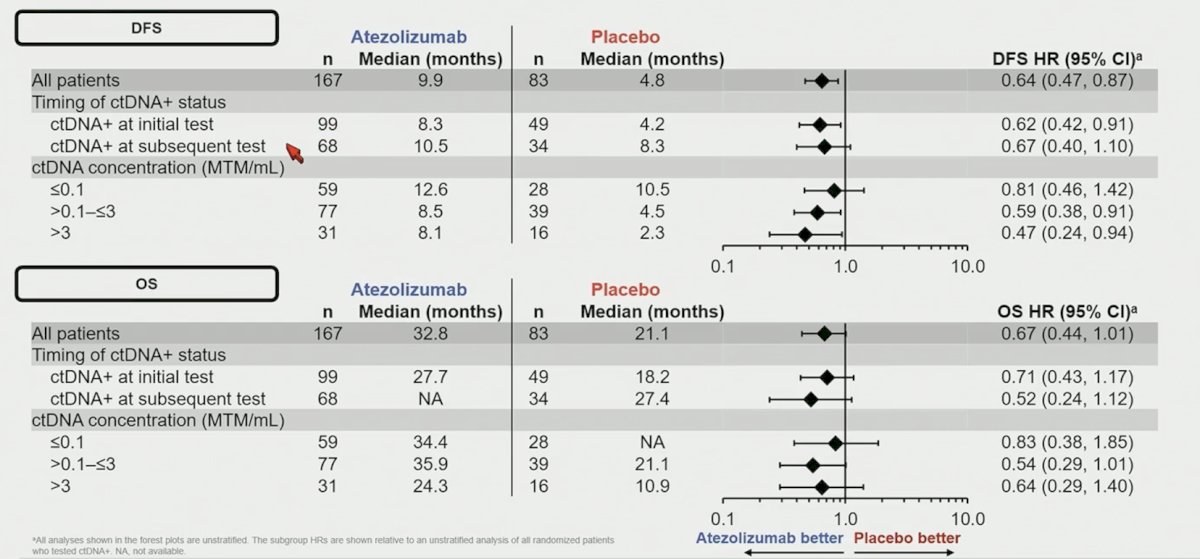
Importantly, atezolizumab had similar efficacy regardless of ctDNA positive timing or concentration:
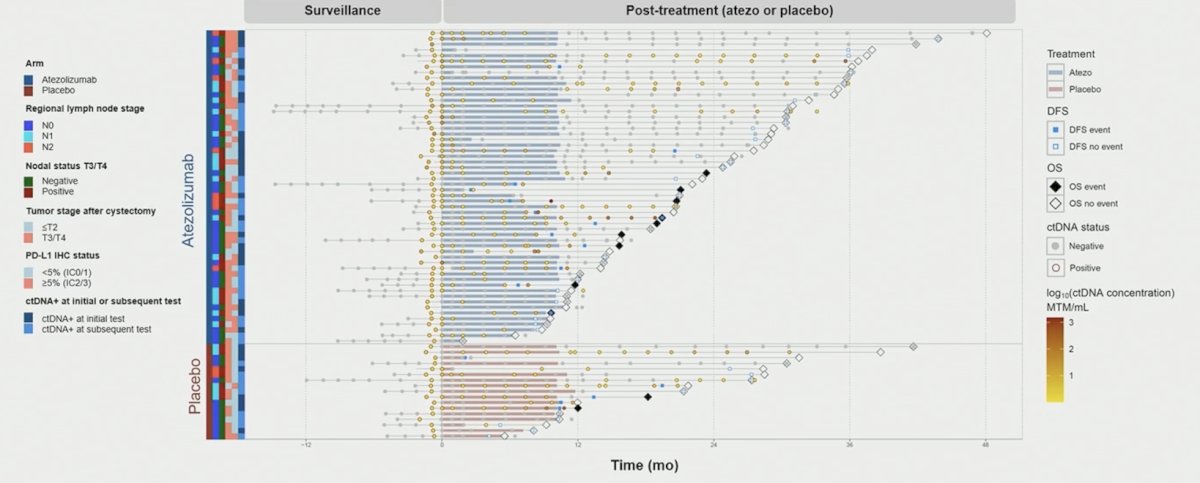
In randomized patients, atezolizumab decreased ctDNA levels between cycle 1 and cycle 3 (log2 fold-change –0.4), while levels increased on placebo (log2 fold-change 0.5; Wilcoxon p = 0.009). ctDNA clearance at cycle 3 or cycle 5 was associated with improved disease free survival and overall survival, and landmark disease free survival and overall survival rates were numerically higher in atezolizumab treated patients. Finally, the following figure is an overview of individual patients who cleared ctDNA, which offers a rich dataset for exploration of ctDNA dynamics:
Dr. Bellmunt concluded his presentation discussing an exploratory analysis of ctDNA dynamics in the IMvigor011 trial with the following take-home points:
- Serial ctDNA testing can differentiate patients with high versus low recurrence risk, which can help avoid unnecessary treatment
- Patients with any detectable ctDNA had a poor prognosis, while those with persistent ctDNA negative status had low risk of recurrence or death
- ctDNA timing and concentration conveyed additional prognostic information beyond binary ctDNA positive/negative status
- Early ctDNA positivity and high ctDNA concentration were associated with shorter disease free survival and overall survival
- In patients with ctDNA positive status, atezolizumab efficacy was similar regardless of timing of positivity or concentration
- Some patients treated with placebo cleared ctDNA and had improved disease free survival, which represents a prognostically favorable subgroup with low baseline ctDNA concentration
- Adjuvant atezolizumab promotes ctDNA reduction and clearance, and these dynamics were associated with improved disease free survival
Presented by: Joaquim Bellmunt, MD, PhD, Dana Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References: