(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, was host to the Poster Session B: Prostate Cancer and Urothelial Carcinoma. Dr. Karim Chamie presented the poster: ECOG ACRIN EA8291 Cohort C: Treatment of recurrent NMIBC with UGN-301 (zalifrelimab) alone and in combination: A phase 1 dose escalation study.
Dr. Chamie began his presentation by noting that high-grade and intermediate-risk NMIBC frequently recur or progress despite standard therapies. UGN-301 is designed to deliver local immune checkpoint blockade within the bladder while limiting systemic exposure. This first-in-human study evaluated UGN-301 alone and in combination with either intravesical UGN-201 (imiquimod) or gemcitabine.
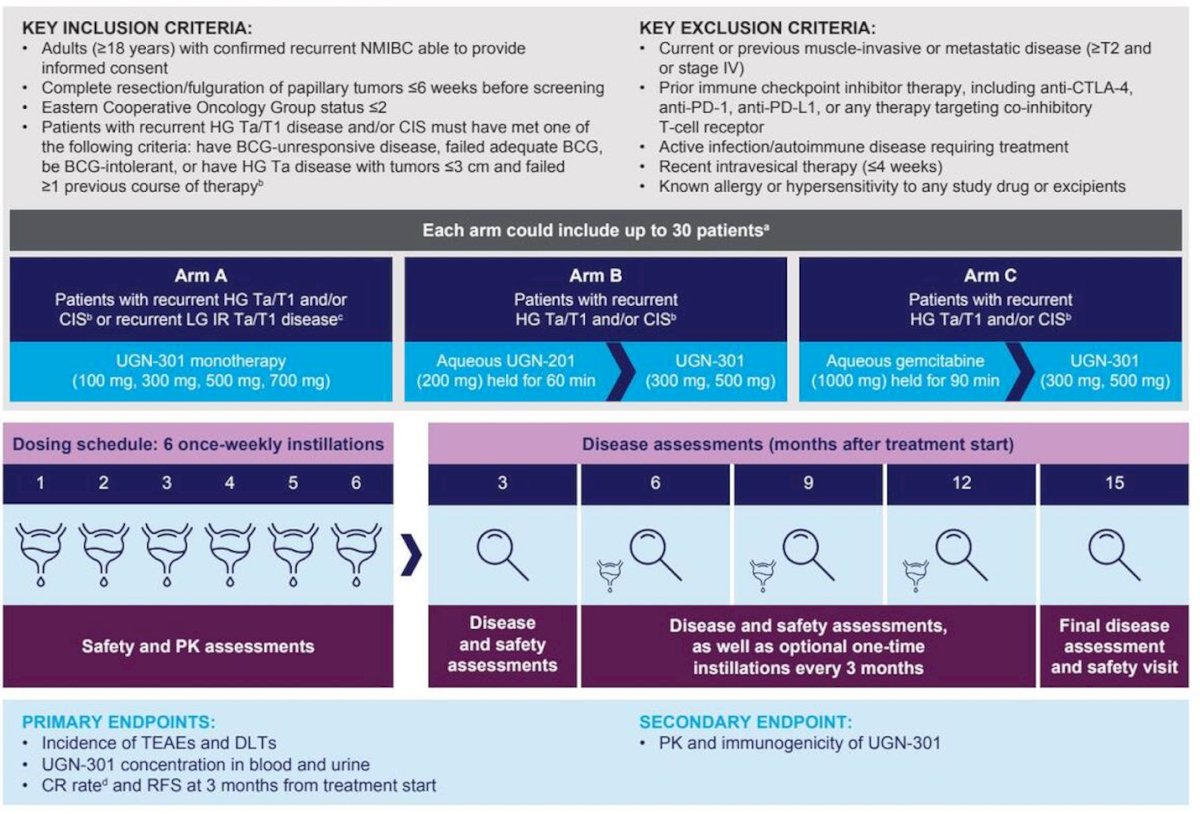
Dr. Chamie outlined that the primary objectives of this study were to determine the biologically effective dose (BED), maximum tolerated dose (MTD), and recommended phase 2 dose (RP2D) of UGN-301 administered as monotherapy and in combination with UGN-201 (imiquimod, a toll-like receptor 7 agonist) or gemcitabine in patients with recurrent NMIBC. Secondary objectives included assessment of the pharmacokinetics (PK) and immunogenicity of UGN-301, both as a single agent and in combination with UGN-201 or gemcitabine
Eligible patients had recurrent NMIBC, including intermediate-risk low-grade Ta/T1 disease or high-grade Ta/T1 and/or CIS. All patients underwent tumor resection or fulguration prior to study entry. Treatment consisted of six once-weekly intravesical instillations, with optional maintenance for patients who were recurrence-free (Ta/T1) or achieved complete response (CIS). Arms included:
- Arm A: UGN-301 monotherapy
- Arm B: UGN-201 plus UGN-301
- Arm C: Gemcitabine plus UGN-301
Dose escalation was guided by adaptive Bayesian modeling to determine the recommended phase II dose.
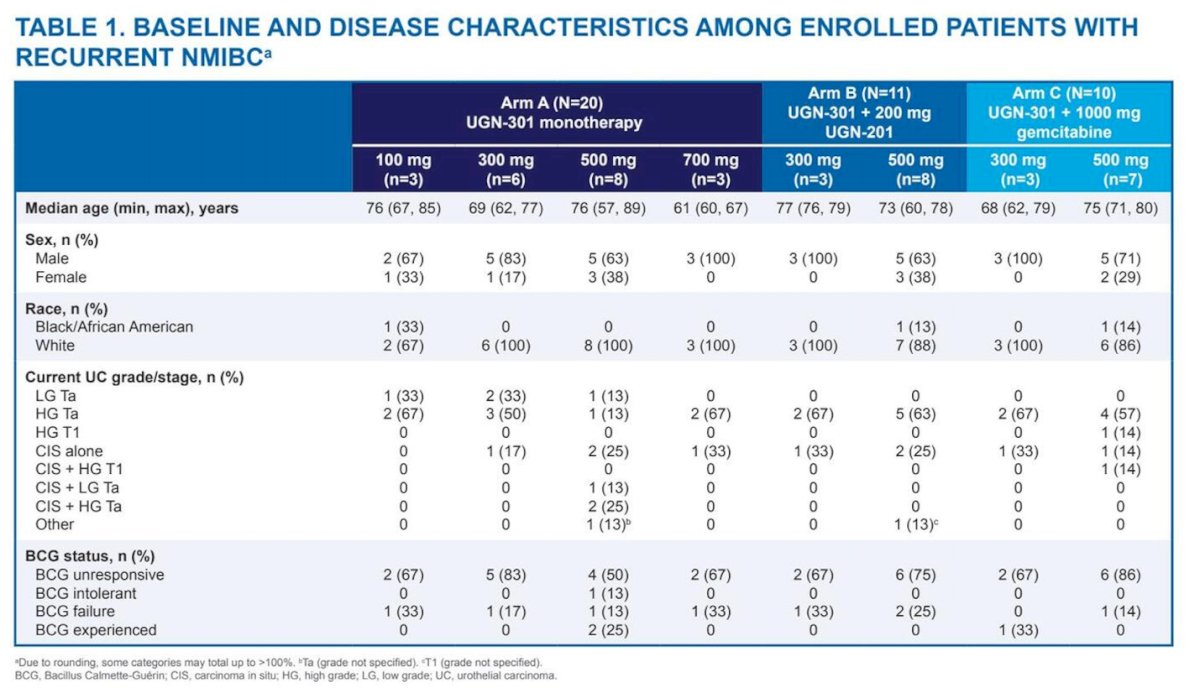
At the September 5, 2025 data cutoff, 41 patients had been treated across dose levels, with most completing all six planned induction instillations. Dose escalation in Arm A reached the maximum feasible dose. The study population was predominantly White, male, and over 65 years of age. In Arm A (n=20), all patients received at least one dose and 95% completed all six doses; in Arms B (n=11) and C (n=10), 100% of patients completed all six induction doses.
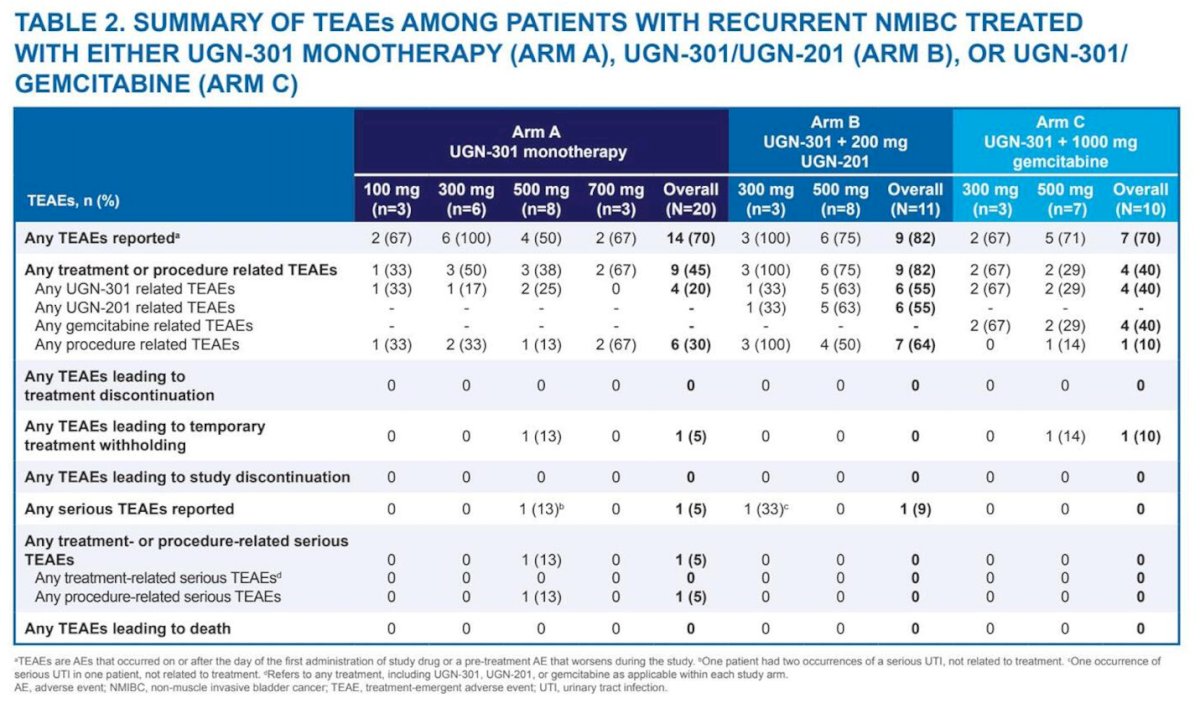
Treatment-emergent adverse events (TEAEs) occurred in 70–82% of patients across arms; however, no dose-limiting toxicities or treatment-related discontinuations were observed. Nearly all TEAEs were mild to moderate in severity, with two severe urinary tract infections deemed unrelated to treatment. There was no dose-dependent increase in TEAE incidence, no TEAEs leading to study discontinuation or death, and only two instances of temporary treatment withholding (one each in Arms A and C). Overall, all dose levels were well tolerated, with few serious TEAEs reported, none considered treatment-related, and no immune-related toxicities identified. A summary of the most common TEAEs is shown in the table below.
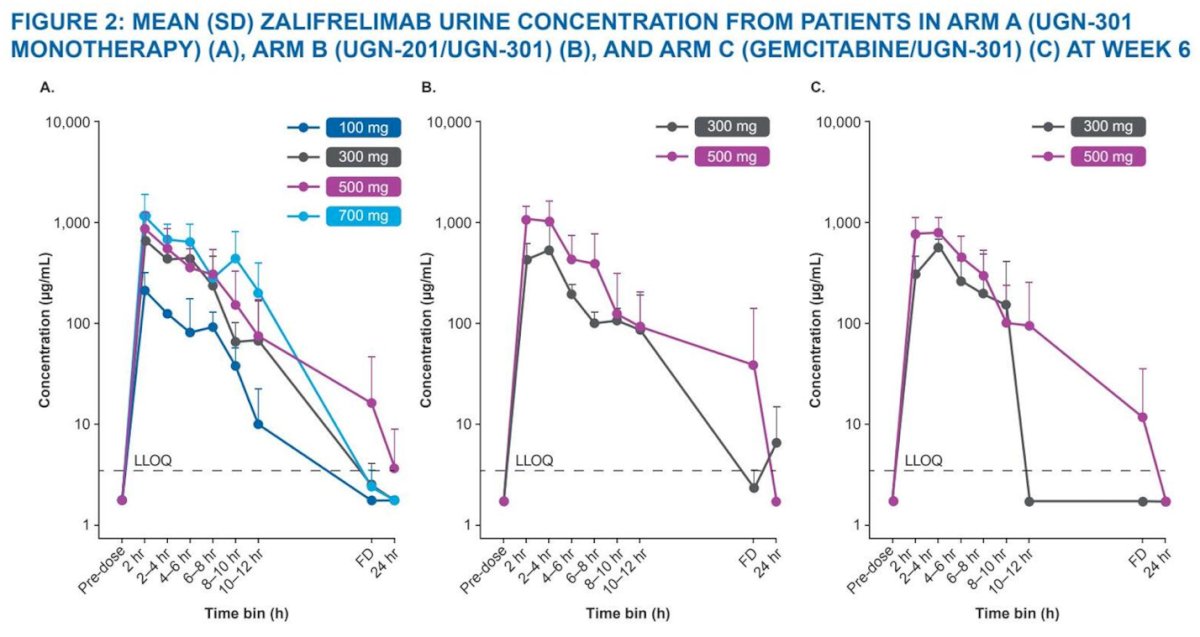
Pharmacokinetic analysis demonstrated sustained intravesical exposure to zalifrelimab, with minimal systemic absorption. Detectable systemic levels occurred in only two patients and were markedly lower than levels seen with intravenous CTLA-4 blockade.
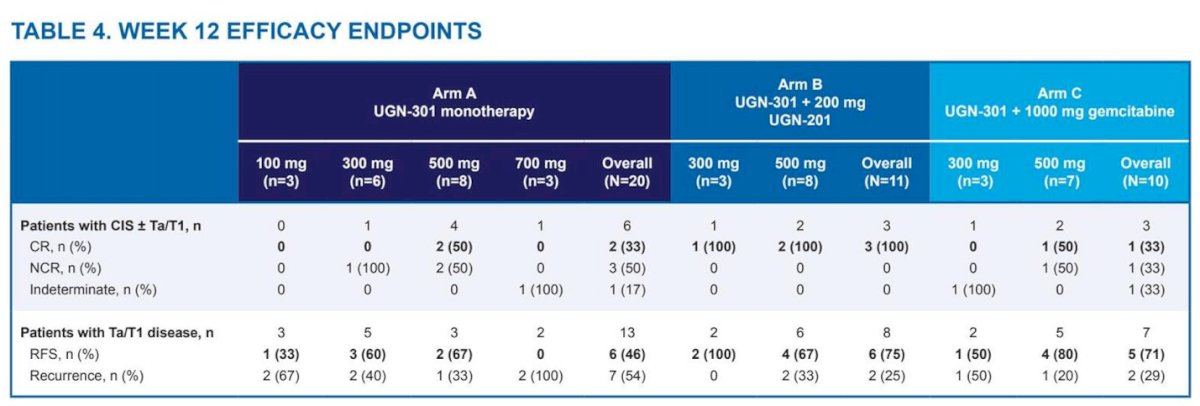
Preliminary efficacy signals were observed at UGN-301 doses of at least 300 mg:
- In patients with CIS ± Ta/T1, complete response rates at Week 12 were 33% with UGN-301 alone, 100% with UGN-201/UGN-301, and 33.3% with gem/UGN-301.
- In patients with Ta/T1 disease, recurrence-free rates at Week 12 were 50% with UGN-301 alone, 75% with UGN-201/UGN-301, and 71.4% with gem/UGN-301.
Durability signals were encouraging. In the monotherapy arm, some patients maintained complete response or recurrence-free status out to 6–15 months. In the combination arm with UGN-201, a subset of CIS and Ta/T1 patients remained disease-free through 9 months and continue on follow-up.
Dr. Chamie concluded:
- Intravesical UGN-301, administered as monotherapy or in combination with UGN-201 or gemcitabine, achieved sustained local bladder exposure with minimal systemic absorption, potentially mitigating CTLA-4–related systemic toxicity.
- The safety profile was favorable across all arms, with no dose-limiting toxicities observed.
- Pharmacokinetic data confirmed prolonged intravesical exposure and limited systemic distribution of UGN-301 (zalifrelimab).
- Early efficacy signals were encouraging, including complete responses in CIS and favorable recurrence-free rates in Ta/T1 disease.
- UGN-301 alone and in combination demonstrated preliminary antitumor activity, supporting continued clinical development.
- Based on the totality of safety, PK, and efficacy data, 500 mg UGN-301 has been selected as the recommended Phase 2 dose (RP2D).
Presented by: Karim Chamie, MD, MSHS, Urologist, Associate Professor of Urology, University of California, Los Angeles, Los Angeles, CA
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.