(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session B: Prostate Cancer and Urothelial Carcinoma. Dr. Kyung Hae Jung presented the poster: Trastuzumab deruxtecan in pretreated patients with HER2-expressing bladder cancer: Final results from the bladder cancer cohort in Part 1 of DESTINY-PanTumor02.
Dr. Jung began by noting that trastuzumab deruxtecan is a HER2-directed antibody–drug conjugate approved for HER2-positive, HER2-low, and HER2-ultralow breast cancer, HER2-positive gastric or gastroesophageal junction adenocarcinoma, and HER2-mutant non–small cell lung cancer. In the primary analysis of DESTINY-PanTumor02 Part 1 (NCT04482309; data cutoff June 8, 2023), trastuzumab deruxtecan demonstrated clinically meaningful antitumor activity across HER2-expressing solid tumors, with an investigator-assessed objective response rate of 37.1%. (1-3)
Within the bladder cancer cohort, the overall objective response rate was 39.0%, including 56.3% in patients with HER2 IHC 3+ tumors and 35.0% in those with IHC 2+ expression. These data supported regulatory approvals in multiple countries for patients with unresectable or metastatic HER2-positive (IHC 3+) solid tumors who have received prior therapy or lack satisfactory alternatives. Final analyses of DESTINY-PanTumor02 Part 1 showed consistent results, with an overall objective response rate of 37.5%. (4) The current report presents the final subgroup analyses of the bladder cancer cohort, including patients with urothelial carcinoma of the renal pelvis, ureter, bladder, or urethra.
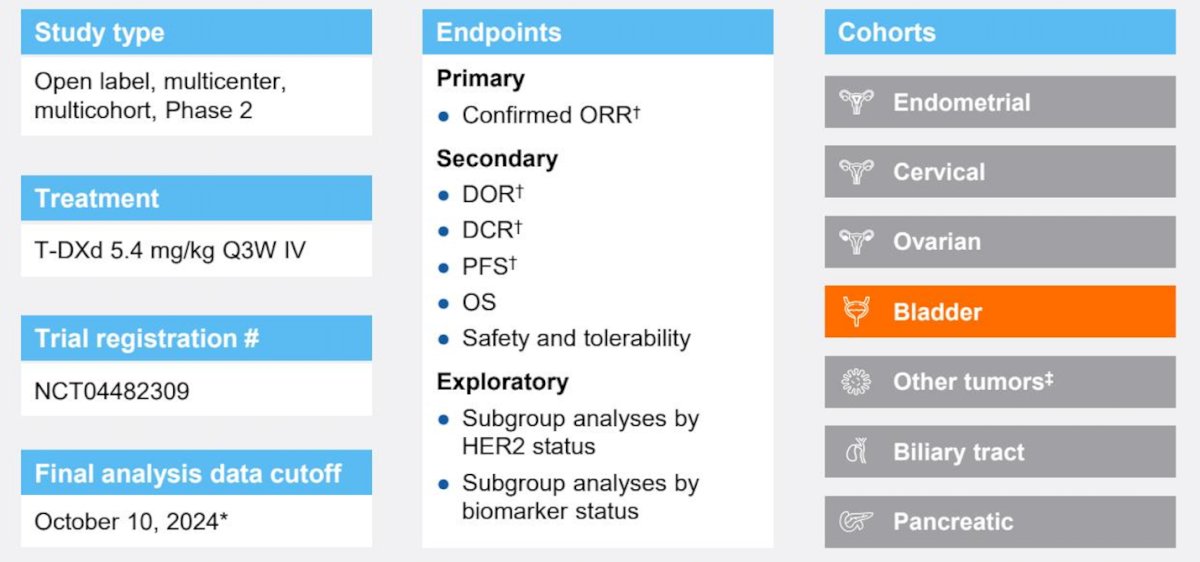
DP-02 (NCT04482309) is a two-part, open-label phase II trial. Part 1 evaluated T-DXd at 5.4 mg/kg every three weeks in patients with HER2 IHC 3+ or 2+ locally advanced or metastatic solid tumors (excluding breast, colorectal, gastric, and non-small cell lung cancer who had received at least one prior systemic therapy or had no remaining treatment options.
Notably, at data cutoff, 267 patients had received T-Dd across all tumor cohorts; investigator-assessed per RECIST 1.1; #included patients with salivary gland cancer (n=19), malignant neoplasm of unknown primary site (n=5), extramammary Paget disease (n=3), cutaneous melanoma (n=2), oropharyngeal neoplasm (n=2), adenoid cystic carcinoma, head and neck cancer, lip and/or oral cavity cancer, esophageal adenocarcinoma, intestinal adenocarcinoma, appendiceal adenocarcinoma, esophageal squamous cell carcinoma, testicular cancer, and vulvar carcinoma (all n=1).
The primary endpoint was investigator-confirmed objective response rate, with secondary endpoints including duration of response, progression-free survival, overall survival, and safety.
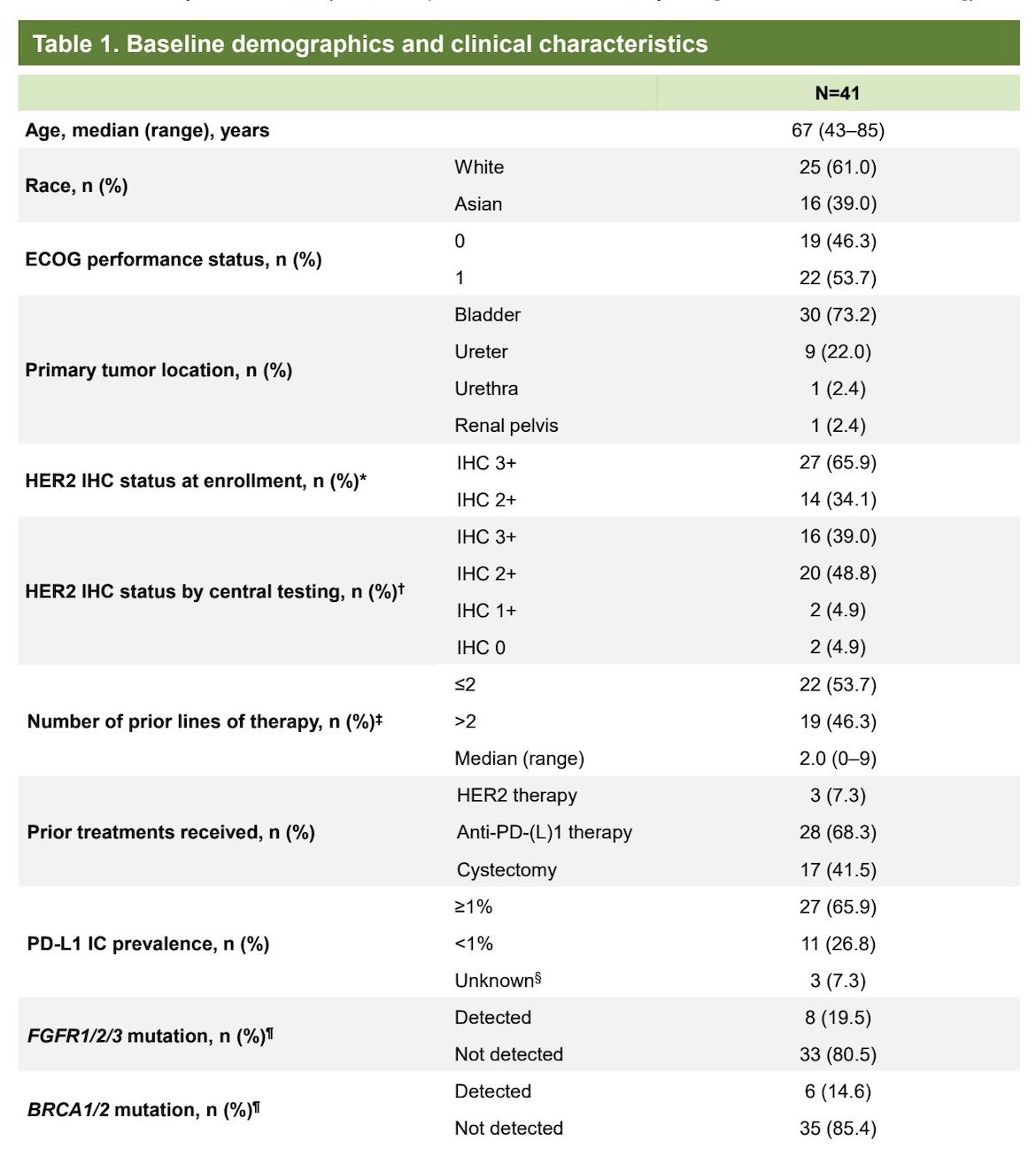
At the October 2024 data cutoff, 41 patients with urothelial carcinoma were treated. Median follow-up was 12.7 months, with a median treatment exposure of 6.2 months and a median of 8 cycles administered. Notably, the most common reason for treatment discontinuation was objective disease progression (65.9%).
Among the 41 patients with urothelial carcinoma included in the analysis, 16 (39.0%) had centrally confirmed HER2 IHC 3+ tumors and 20 (48.8%) had HER2 IHC 2+ tumors. The median age was 67 years, and the majority of patients had an ECOG performance status of 1 at baseline, reflecting a previously treated but functionally preserved population. Other characteristics are shown in the table below.
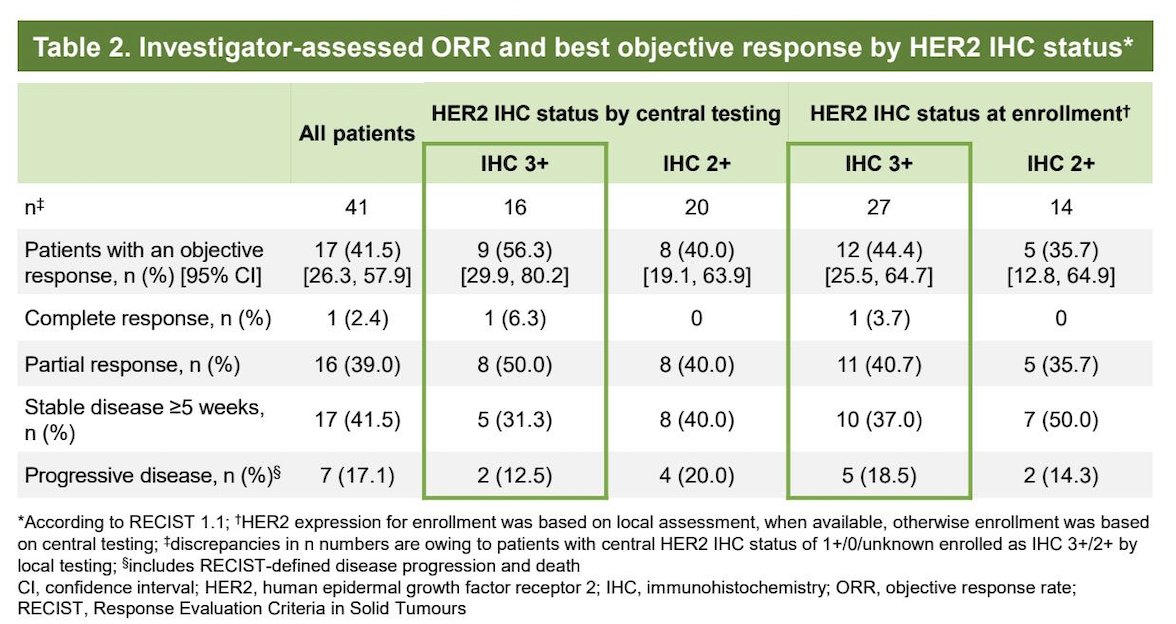
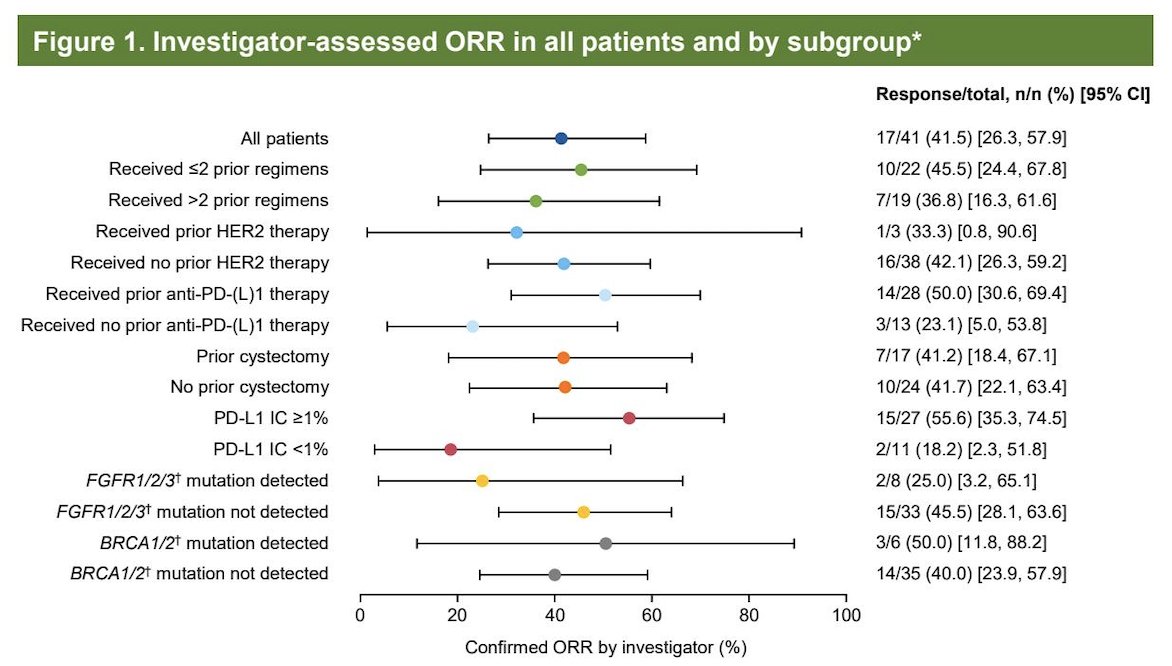
The investigator-assessed ORR was 41.5% (17 of 41 patients; 95% CI 26.3 to 57.9). Among responders, 7 had received more than two prior systemic regimens, 14 had prior anti–PD-L1 therapy, and 7 had undergone prior cystectomy, demonstrating activity in a heavily pretreated population.
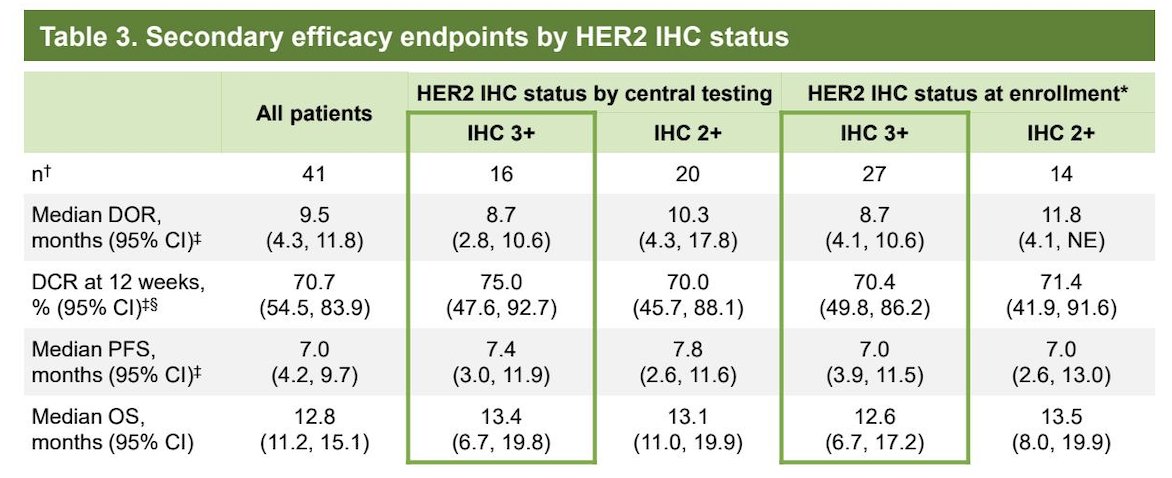
By HER2 expression level on central testing:
- In IHC 3+ tumors (n=16), ORR was 56.3%, including one complete response and eight partial responses.
- In IHC 2+ tumors (n=20), ORR was 40.0%, all partial responses.
Investigator-assessed objective responses were observed across a broad range of prior treatment exposures and tumor biomarker subgroups. Responses were seen irrespective of number of prior regimens, prior anti–PD-(L)1 therapy, prior cystectomy, and prior HER2-directed therapy. Activity was also observed across biomarker-defined groups, including PD-L1 expression levels and FGFR1/2/3 and BRCA1/2 mutation status, supporting consistent antitumor activity across clinically diverse patient subsets.
Median duration of response was 9.5 months in the overall cohort, with similar durability across IHC subgroups. Median progression-free survival was 7.0 months overall, and median overall survival was 12.8 months. Outcomes were generally consistent whether HER2 status was determined locally or centrally.
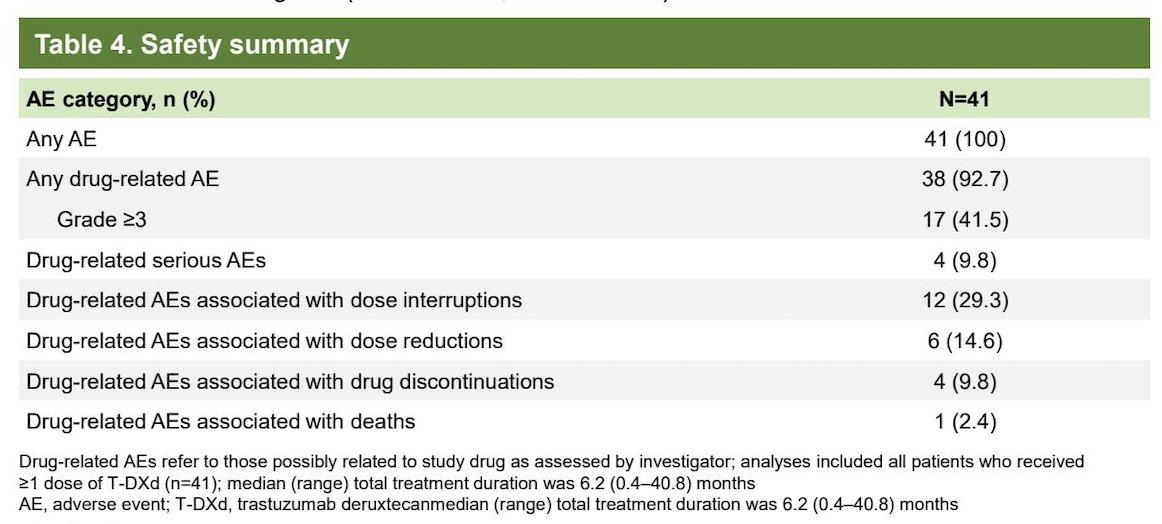
Regarding safety, drug-related interstitial lung disease or pneumonitis occurred in 4 patients (9.8%), including one grade 1 and three grade 2 events. No new safety signals were observed, and the overall safety profile was consistent with prior experience with T-DXd.
Dr. Jung concluded with several key observations:
- T-DXd demonstrated durable and clinically meaningful activity in HER2-expressing advanced bladder cancer.
- Responses were observed across varied prior treatment backgrounds, including prior immunotherapy and multiple prior lines.
- Higher response rates were seen in IHC 3+ tumors, though meaningful activity was also observed in IHC 2+ disease.
- The safety profile remained consistent, with manageable rates of interstitial lung disease.
Presented by: Kyung Hae Jung, MD, Professor of Oncology, University of Ulsan College of Medicine (UUCM), Medical Oncologist, Asan Medical Center (AMC), Seoul, Korea
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:- Meric-Bernstam F, Makker V, Oaknin A, Oh DY, Banerjee S, González-Martín A, Jung KH, Ługowska I, Manso L, Manzano A, Melichar B, Siena S, Stroyakovskiy D, Fielding A, Ma Y, Puvvada S, Shire N, Lee JY. Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J Clin Oncol. 2024 Jan 1;42(1):47-58. doi: 10.1200/JCO.23.02005. Epub 2023 Oct 23. PMID: 37870536; PMCID: PMC10730032.
- Enhertu (fam-trastuzumab deruxtecan-nki): highlights of prescribing information 2025. Available from: https://www.accessdata.fda.gov Accessed January 29, 2026.
- Enhertu (trastuzumab deruxtecan): summary of product characteristics. 2025. Available from: https://www.medicines.org.uk/emc/product/12135/smpc. Accessed January 29, 2026.
- Meric-Bernstam F, Makker V, Oaknin A, Oh DY, Banerjee S, González-Martín A, Jung KH, Ługowska I, Manso L, Manzano A, Melichar B, Siena S, Stroyakovskiy D, Fielding A, Ma Y, Puvvada S, Shire N, Lee JY. Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J Clin Oncol. 2024 Jan 1;42(1):47-58. doi: 10.1200/JCO.23.02005. Epub 2023 Oct 23. PMID: 37870536; PMCID: PMC10730032.