(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session B: Prostate Cancer and Urothelial Carcinoma. Dr. Raj Satkunasivam presented the poster: ECOG ACRIN EA8291 Cohort C: A phase II clinical trial of neoadjuvant sasanlimab and stereotactic body radiation therapy as an in situ vaccine for cisplatin-ineligible muscle invasive bladder cancer (MIBC): The RAD VACCINE MIBC clinical trial.
Dr. Satkunasivam began by highlighting that up to half of patients with MIBC are not candidates for cisplatin-based neoadjuvant chemotherapy, representing a significant unmet need. Immune checkpoint inhibitors have emerged as an alternative strategy, and combining them with local therapies such as SBRT may enhance antitumor immunity.1-3 SBRT delivered at 8 Gy × 3 fractions can induce immunogenic cell death and potentially function as an in situ vaccine, augmenting systemic immune responses when paired with ICI.4
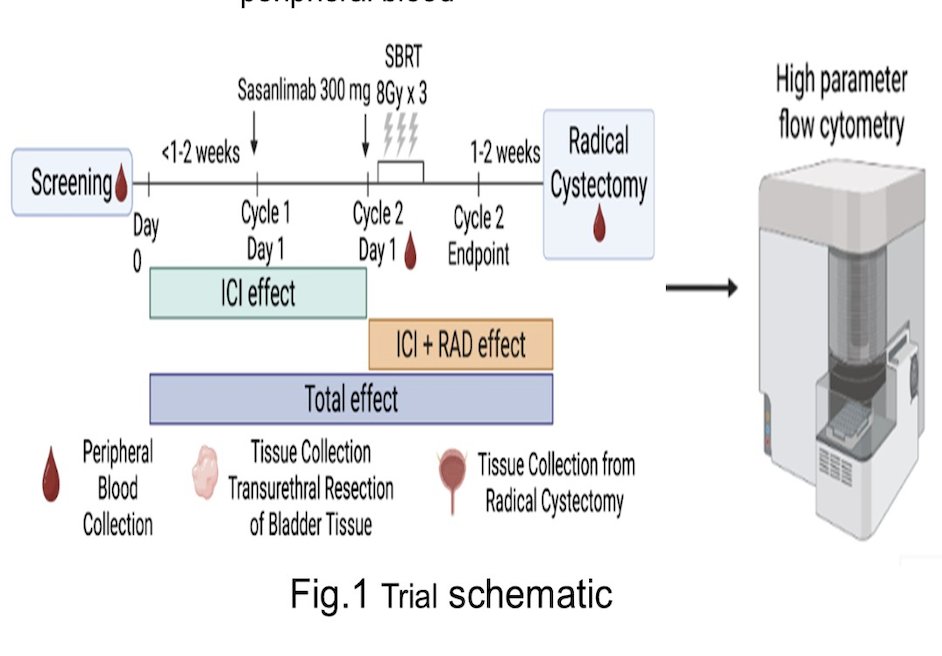
This prospective phase II trial enrolled patients with cT2–4aN0M0 MIBC who were cisplatin-ineligible or declined chemotherapy. Patients received sasanlimab (two 300 mg subcutaneous doses, 28 days apart) with SBRT to the bladder tumor (8 Gy × 3 fractions at 48-hour intervals, starting during the second ICI cycle) prior to radical cystectomy.
The study used a Simon two-stage design, enrolling 33 patients with pathologic complete response (pT0) as the primary endpoint. Secondary endpoints included safety, health-related quality of life, and recurrence-free survival, with exploratory correlative immune analyses. The study schema is shown below.
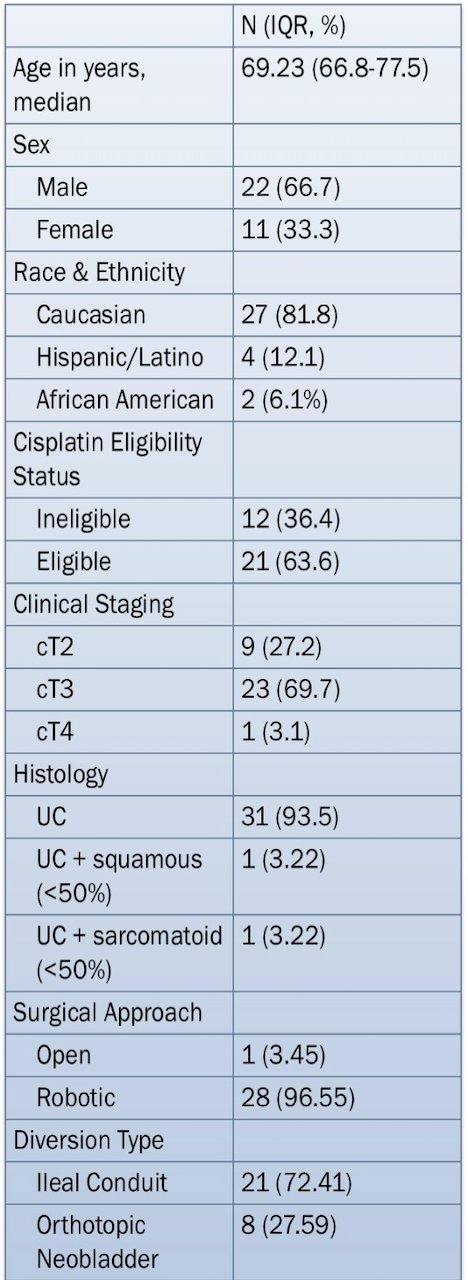
Between March 2022 and April 2025, 33 patients were enrolled; 73% had ≥cT3 disease. Four patients withdrew due to progression before cystectomy, and a total of 29 patients completed the intervention. Baseline characteristics are illustrated in the table below.
The trial met its primary endpoint:
- Pathologic complete response (pT0) rate was 44.8%.
- 75.9% of patients were downstaged to pT0/Ta/T1 at cystectomy.
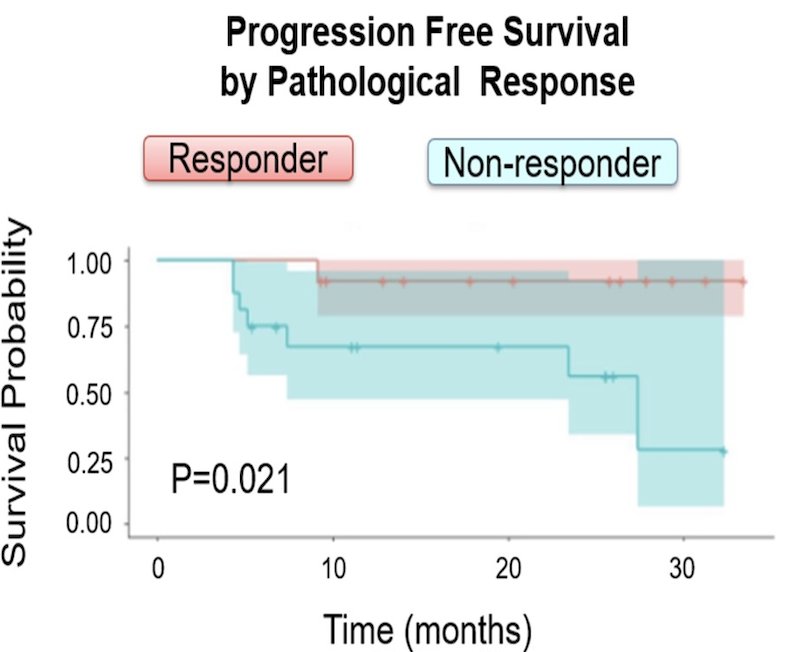
With a median follow-up sufficient for early outcomes, the two-year metastasis-free survival was:
- 72.2% overall,
- 92.3% in patients achieving pCR,
- 56.3% in patients without pCR (p = 0.02).
Treatment was generally well tolerated. Grade ≥3 treatment-related adverse events occurred in 9.1% of patients, including hypothyroidism (21%), adrenal insufficiency (6.9%), and nephritis (3.5%), both managed with steroids. Grade ≥3 Clavien-Dindo 30-day surgical complications occurred in 13.8%, with no perioperative mortality. Importantly, there was no significant deterioration in EORTC QLQ-C30 quality-of-life scores during ICI therapy, SBRT, or after cystectomy.
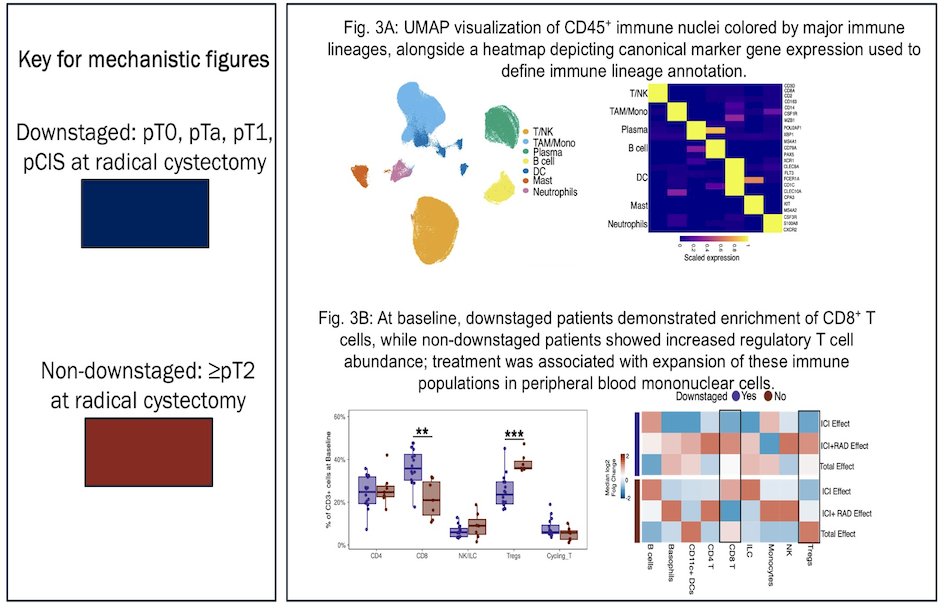
Correlative analyses integrating tumor and peripheral immune profiling demonstrated distinct immune signatures associated with pathologic downstaging. UMAP-based clustering of CD45⁺ immune nuclei identified major immune lineages, supported by canonical marker gene expression. At baseline, patients who ultimately achieved downstaging (pT0/pTa/pT1/pCIS) showed enrichment of CD8⁺ T cells, whereas non-downstaged (≥pT2) patients exhibited increased regulatory T-cell abundance. Treatment was associated with expansion of these immune subsets in peripheral blood mononuclear cells, suggesting that both baseline immune contexture and therapy-induced immune modulation may contribute to pathologic response.
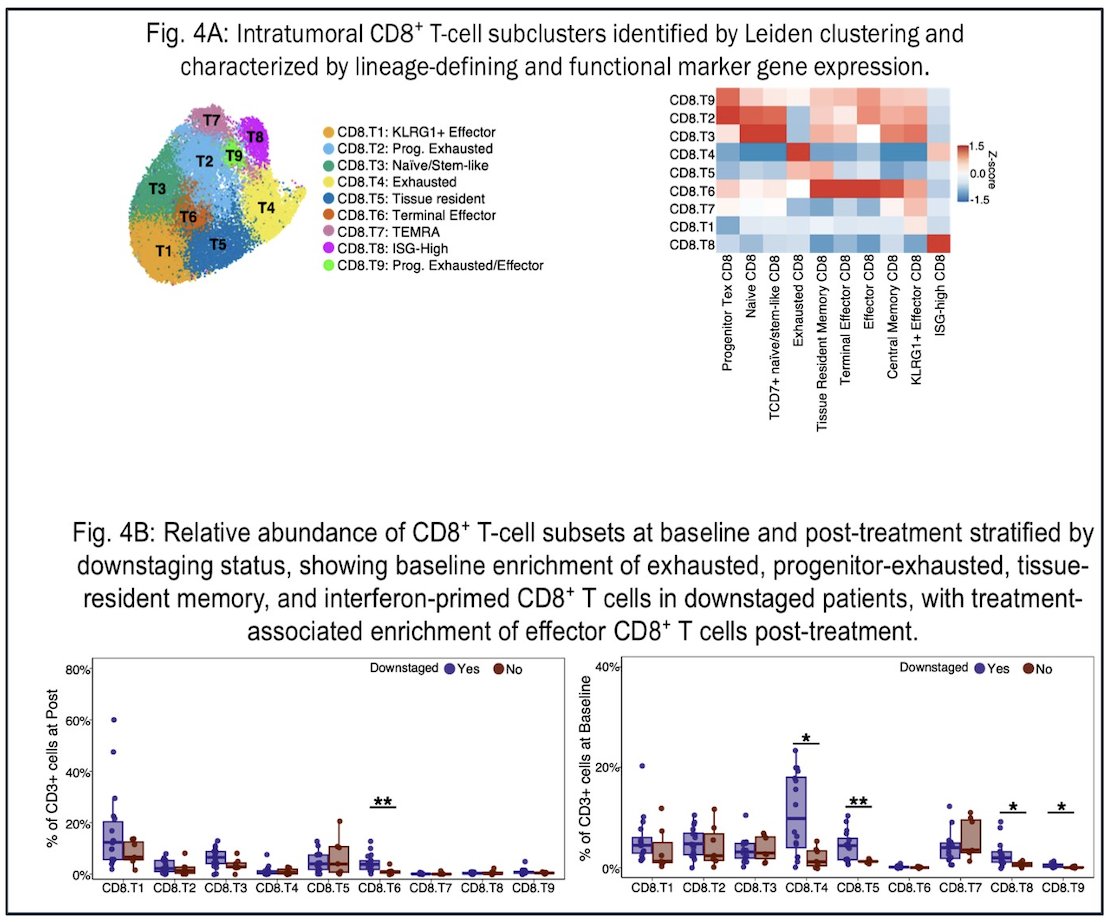
Moreover, high-resolution clustering of intratumoral CD8⁺ T cells identified multiple functionally distinct subpopulations, including naïve/stem-like, progenitor-exhausted, terminally exhausted, tissue-resident memory, ISG-high, and KLRG1⁺ effector subsets. At baseline, downstaged patients demonstrated enrichment of exhausted, progenitor-exhausted, tissue-resident memory, and interferon-primed CD8⁺ T-cell populations, consistent with a pre-existing, antigen-experienced immune microenvironment. Following treatment, there was a relative expansion of effector CD8⁺ T cells, supporting a model in which therapy reshapes the intratumoral immune landscape toward a more cytotoxic, antitumor phenotype associated with pathologic response.
Furthermore, pseudotime trajectory analysis of intratumoral CD8⁺ T cells revealed four distinct differentiation pathways spanning naïve/stem-like to terminally exhausted states. Gene expression trends across pseudotime demonstrated coordinated upregulation of checkpoint (HAVCR2, LAG3, PDCD1), cytotoxic (GNLY, GZMB, IFNG), and exhaustion-associated (CXCL13, ENTPD1, TOX) markers, alongside dynamic changes in memory and effector-related genes. Importantly, pathological downstaging correlated with limited progression toward late terminally exhausted phenotypes, with preservation of earlier, progenitor-like and intermediate states. These findings suggest that maintaining a less terminally differentiated CD8⁺ T-cell landscape may be associated with improved pathologic response.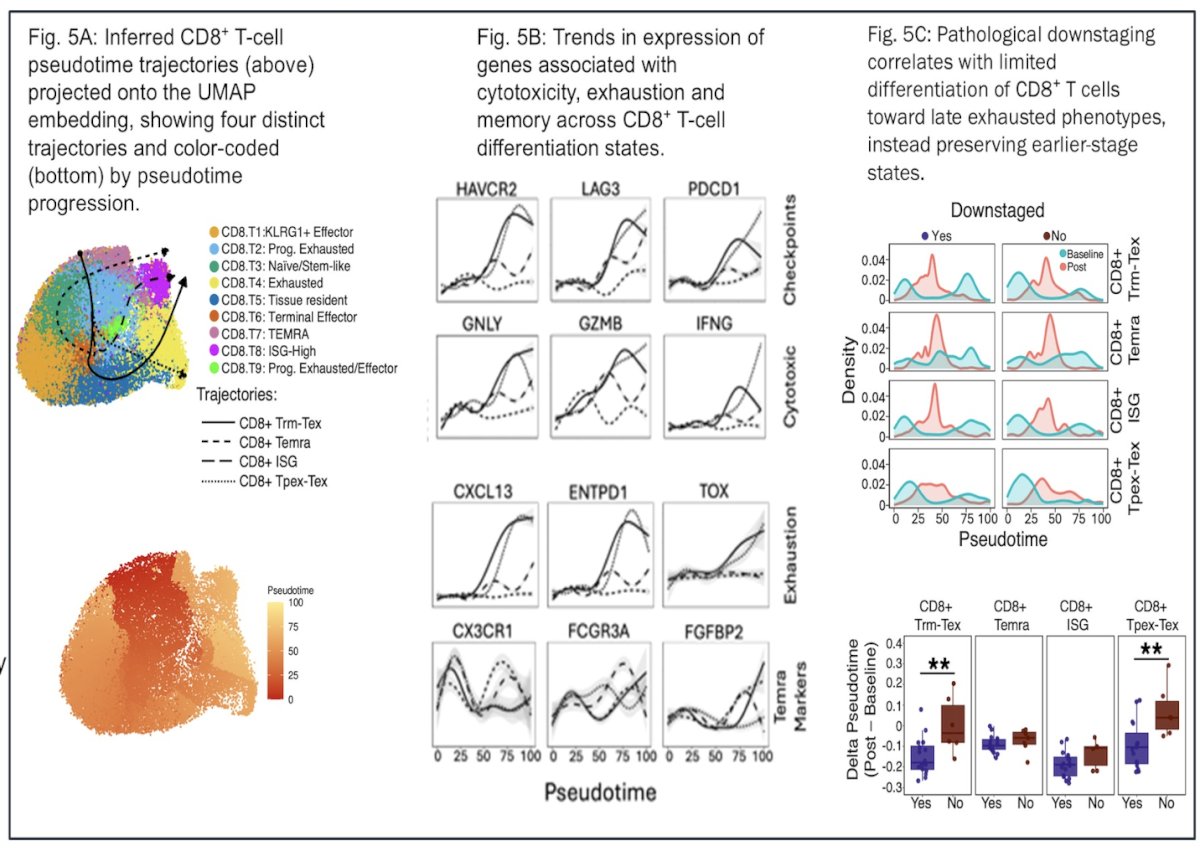
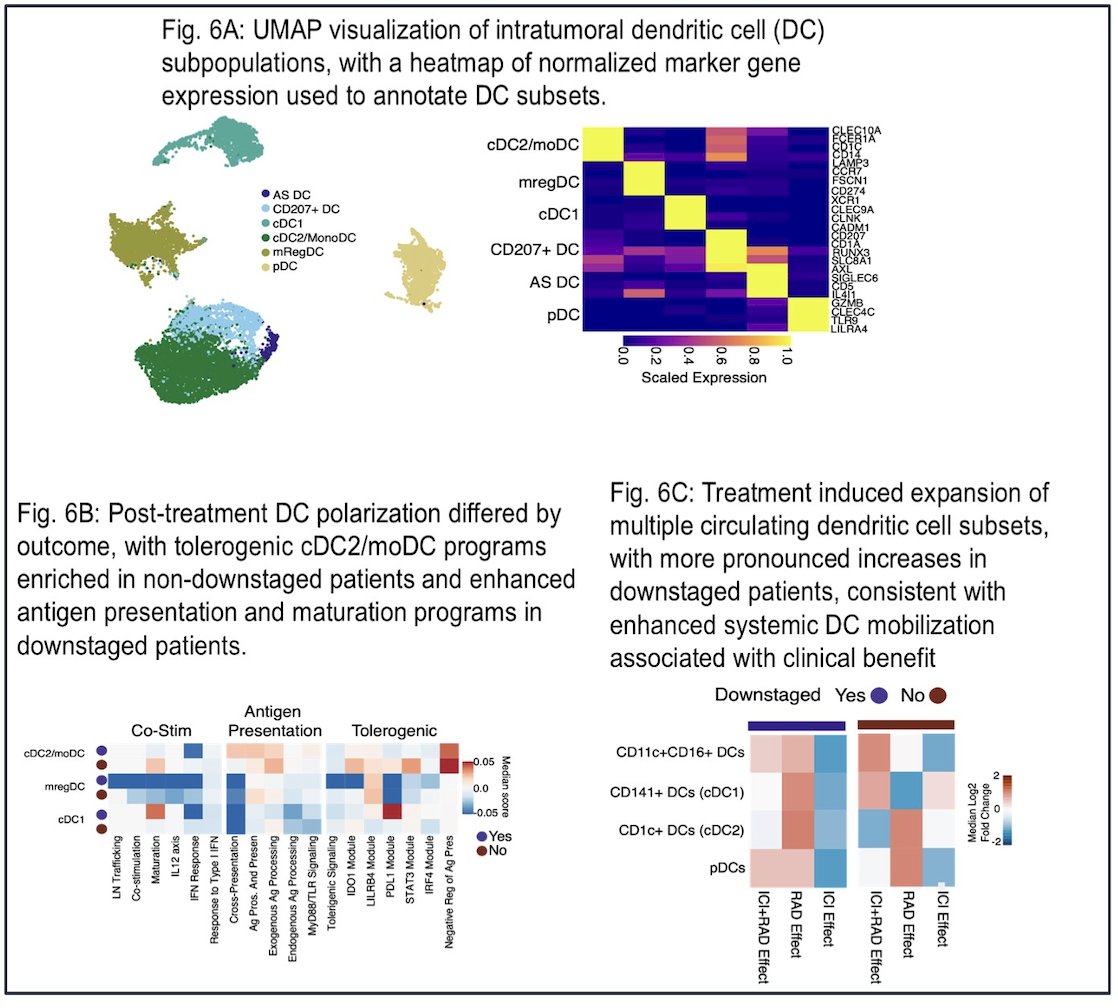
Another subset exhibited robust dendritic cell expansion associated with activated CD4+ T-cell responses, suggesting multiple immune pathways contributing to the response.
Dr. Satkunasivam concluded:
- The combination of SBRT and sasanlimab achieved a clinically meaningful pCR rate in cisplatin-ineligible MIBC.
- Downstaging rates were high, and pCR was strongly associated with improved metastasis-free survival.
- Toxicity was acceptable, with manageable immune-related events and no significant impact on quality of life.
- Correlative analyses suggest biologically distinct response mechanisms that may inform future patient selection.
- These findings support further investigation of in situ vaccination strategies, potentially in combination with additional systemic agents, to improve pCR and long-term disease control, with implications for organ preservation approaches.
Presented by: Raj Satkunasivam, MD, MS, FRCSC, Assistant Professor, Weill Cornell Medical College, Department of Urology, Houston Methodist Hospital
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.Related content: Phase II Trial of Neoadjuvant Sasanlimab and SBRT as an In Situ Vaccine in Cisplatin-Ineligible MIBC - Raj Satkunasivam
- Szabados B, Kockx M, Assaf ZJ, van Dam PJ, Rodriguez-Vida A, Duran I, Crabb SJ, Van Der Heijden MS, Pous AF, Gravis G, Herranz UA, Protheroe A, Ravaud A, Maillet D, Mendez MJ, Suarez C, Linch M, Prendergast A, Tyson C, Stanoeva D, Daelemans S, Rombouts M, Mariathasan S, Tea JS, Mousa K, Sharma S, Aleshin A, Banchereau R, Castellano D, Powles T. Final Results of Neoadjuvant Atezolizumab in Cisplatin-ineligible Patients with Muscle-invasive Urothelial Cancer of the Bladder. Eur Urol. 2022 Aug;82(2):212-222. doi: 10.1016/j.eururo.2022.04.013. Epub 2022 May 14. PMID: 35577646.
- Divya V Natesan et al. Updated results of phase II trial using escalating doses of neoadjuvant atezolizumab for cisplatin-ineligible patients with nonmetastatic urothelial cancer (NCT02451423).. J Clin Oncol 39, e16510-e16510(2021).
DOI:10.1200/JCO.2021.39.15_suppl.e16510 - Li R, Nocera L, Rose KM, Raggi D, Naidu S, Mercinelli C, Cigliola A, Tateo V, Patanè D, Grass GD, Gilbert SM, Sexton WJ, Bandini M, Moschini M, Briganti A, Montorsi F, Spiess PE, Necchi A. Comparative Effectiveness of Neoadjuvant Pembrolizumab Versus Cisplatin-based Chemotherapy or Upfront Radical Cystectomy in Patients with Muscle-invasive Urothelial Bladder Cancer. Eur Urol Oncol. 2024 Jun;7(3):614-624. doi: 10.1016/j.euo.2023.12.008. Epub 2024 Jan 6. PMID: 38184473.
- Vanpouille-Box C, Alard A, Aryankalayil MJ, Sarfraz Y, Diamond JM, Schneider RJ, Inghirami G, Coleman CN, Formenti SC, Demaria S. DNA exonuclease Trex1 regulates radiotherapy-induced tumour immunogenicity. Nat Commun. 2017 Jun 9;8:15618. doi: 10.1038/ncomms15618. PMID: 28598415; PMCID: PMC5472757.