(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Devaki Surasi discussing combination sequencing for PSMA-based therapy in advanced disease. Dr. Surasi started with a case of a 74 year old with metastatic castration resistant prostate cancer (mCRPC) status post ADT, 6 cycles of docetaxel, enzalutamide, and palliative radiotherapy to the prostate, the right clavicle, and L3/L4. The patient’s medical history included hypertension, hyperlipidemia, and lymphoplasmacytic lymphoma. This patient subsequently presented for 177Lu-PSMA with a PSA of 197 ng/mL:

Unfortunately, after 6 cycles of 177Lu-PSMA-617, the patient’s disease progressed (PSA 1,017 ng/mL):
Dr. Surasi notes that there are several therapeutic options for mCRPC, including hormonal therapy, radioligand therapy (alpha emitters), chemotherapy, or immunotherapy: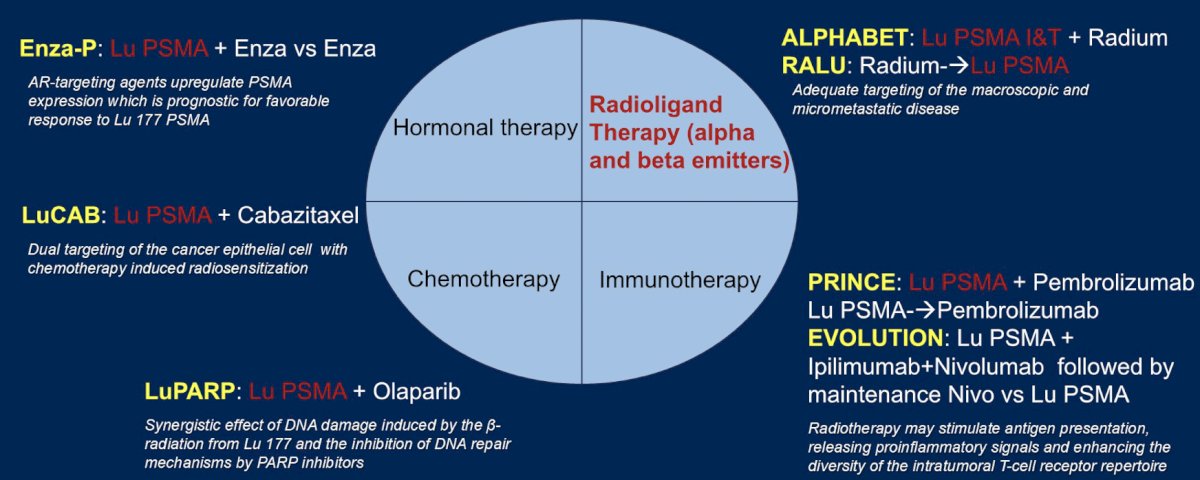
Enza-P patients had mCRPC not previously treated with chemotherapy or androgen receptor pathway inhibitors (prior abiraterone and/or docetaxel for hormone-sensitive disease were allowed), 68Ga-PSMA-positive disease on PET, and at least 2 risk factors associated with early progression on enzalutamide.1 Patients were randomized to 177Lu-PSMA-617 + enzalutamide versus enzalutamide alone:![Enza-P patients had mCRPC not previously treated with chemotherapy or androgen receptor pathway inhibitors (prior abiraterone and/or docetaxel for hormone-sensitive disease were allowed), 68Ga-PSMA-positive disease on PET, and at least 2 risk factors associated with early progression on enzalutamide [1]. Patients were randomized to 177Lu-PSMA-617 + enzalutamide versus enzalutamide alone:](/images/com-doc-importer/189-asco-gu-2025/asco-gu-2025-psma-based-therapy-in-advanced-disease-touching-on-combination-sequencing/image-3.jpg)
In the enzalutamide + 177Lu-PSMA-617 arm, 81% of patients received four doses of 177Lu-PSMA-617. Over a median follow up of 20 months (IQR 18-21), PSA progression free survival was longer with enzalutamide + 177Lu-PSMA-617 versus enzalutamide-alone (median 13 versus 7.8 months; HR 0.43, 95% CI 0.29-0.63, p < 0.001). Additionally, other clinical outcomes, including PSA50 and PSA90 improved with 177Lu-PSMA-617 + enzalutamide: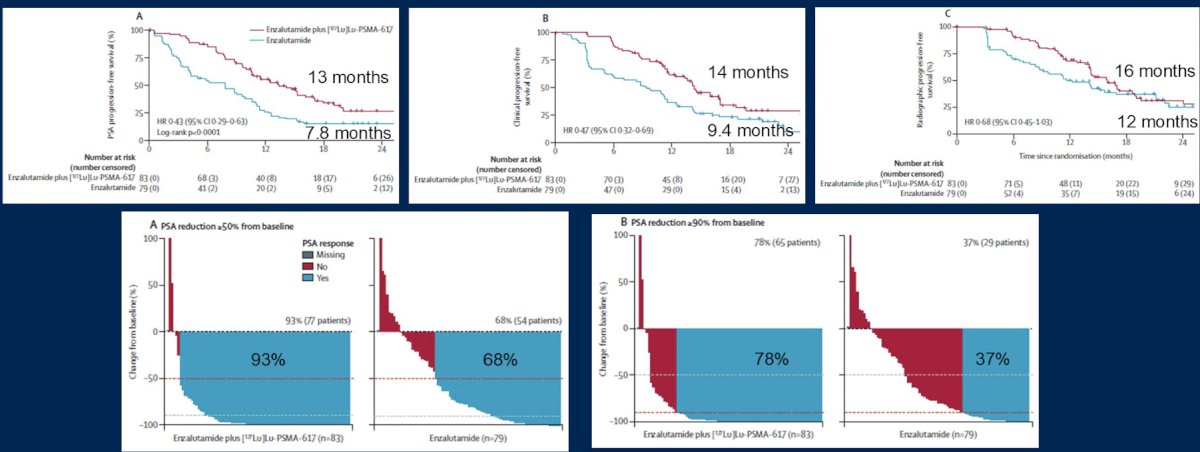
The LuCAB phase I/II trial is a single center, ongoing trial that was initially presented at ASCO 2023. This trial is combining 177Lu-PSMA-617 up to six cycles with cabazitaxel up to 12 doses, with cabazitaxel dose escalation: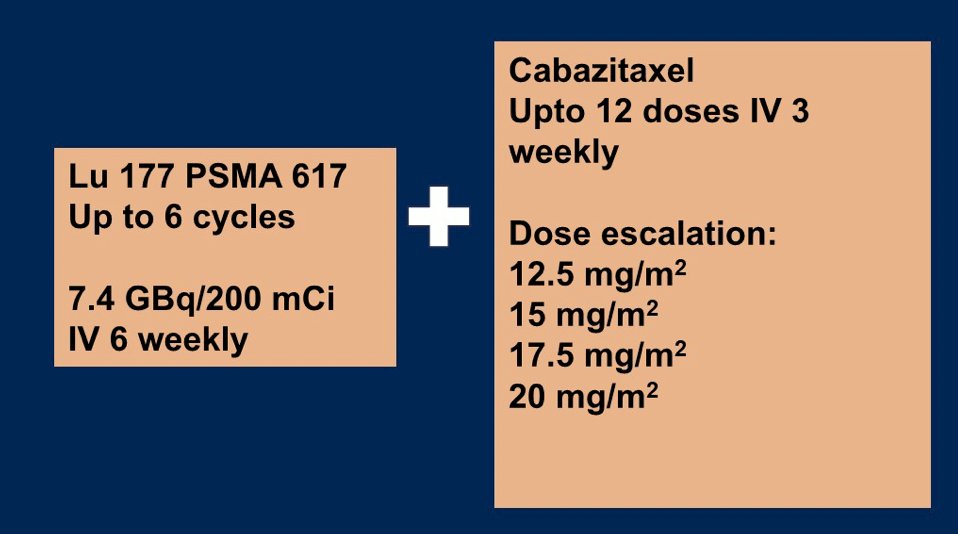
The primary objective was assessing the maximal tolerated dose of cabazitaxel and 177Lu-PSMA-617, with secondary objectives including adverse events, PSA50, response rate, radiographic progression free survival, PSA progression free survival, overall survival, objective response rate, and evaluation of pain and health-related quality of life. This trial has been recruiting since August 2022.
LuPARP is a phase 1 trial of 177Lu-PSMA-617 and olaparib with the following trial schema: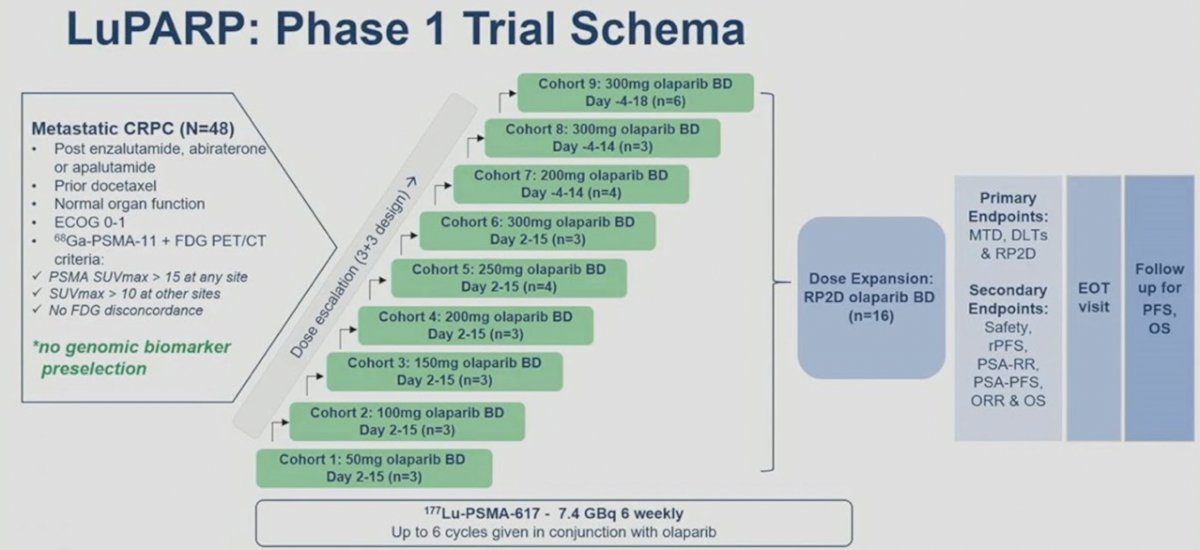
For treatment-related adverse events, no dose limiting toxicities were reported across the dose levels, and there were no grade 4 adverse events. One treatment-related serious adverse event occurred (febrile neutropenia), and dose delay due to hematological toxicity occurred in 3 (9%) patients (cohorts 2, 5, and 6). Dose reduction was required in 4 patients (12%), with 3 due to hematological toxicity and 1 due to xerostomia. The recommended phase 2 dose was 7.4 Gb of 177Lu-PSMA-617 in conjunction with olaparib 300 mg twice daily on days -4 to 18 of each 6 weekly cycle. In the overall cohort (i.e., Cohorts 1 to 9), the PSA50 and PSA90 response rates were 66% and 44%, respectively, and the objective response rate by RECIST v1.1 criteria was 78%: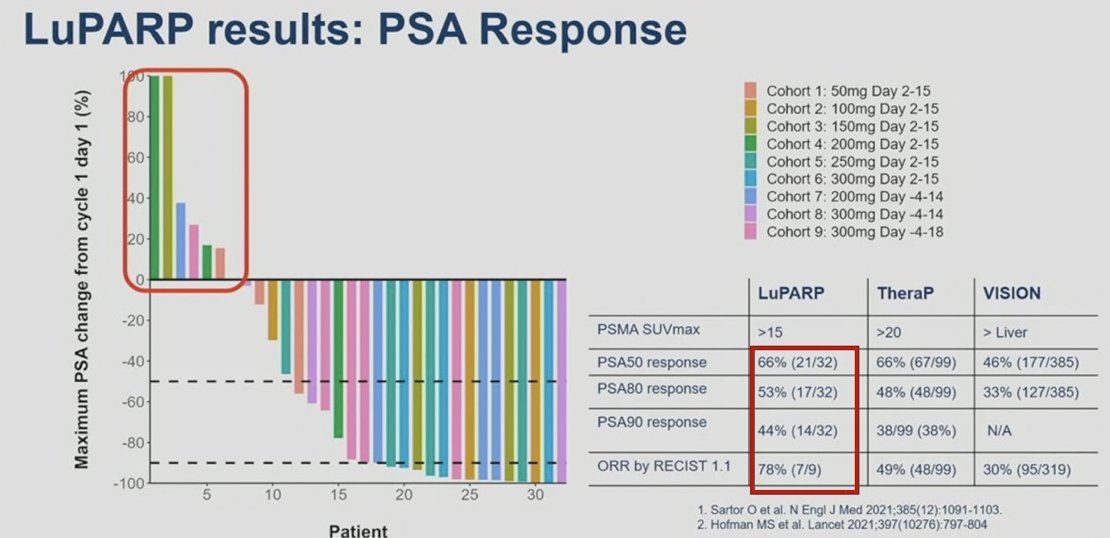
PRINCE is a phase 1 trial of 177Lu-PSMA-617 in combination with pembrolizumab in mCRPC, first presented at ESMO 2021. The trial design for PRINCE is as follows: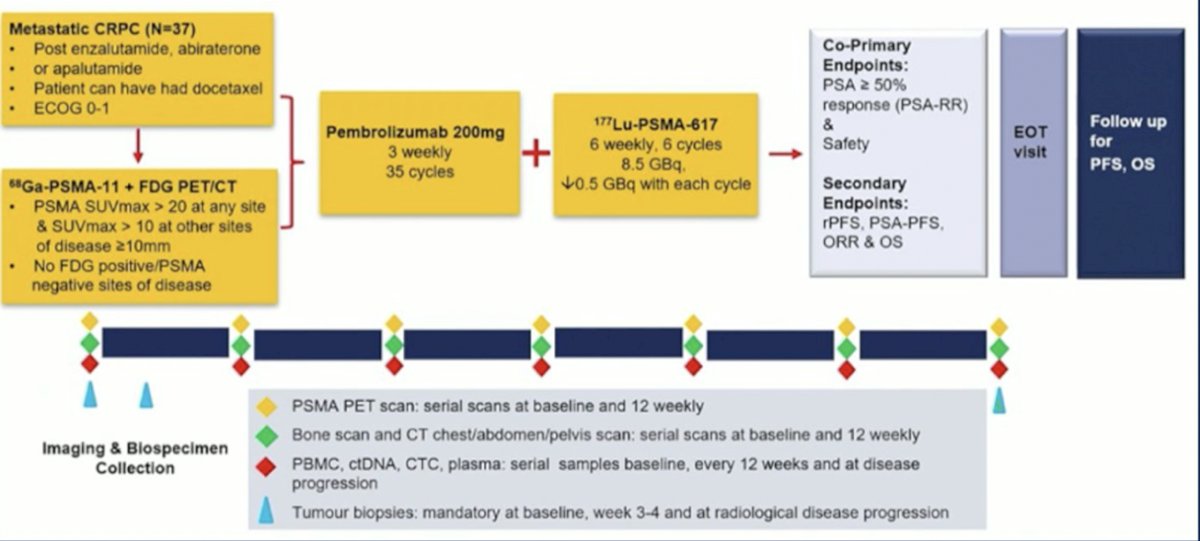
Patients received a median of 4 cycles of 177Lu-PSMA-617 and 8 doses of pembrolizumab. Treatment-related adverse events (>=10%) were low grade (1-2) and included xerostomia (76%), fatigue (43%), nausea (24%), rash (22%), pruritus (19%), elevated ALT (11%), diarrhea (11%), and bone pain (11%). The objective response rate according to RECIST v1.1 was 78%, with a PSA50 response of 73%: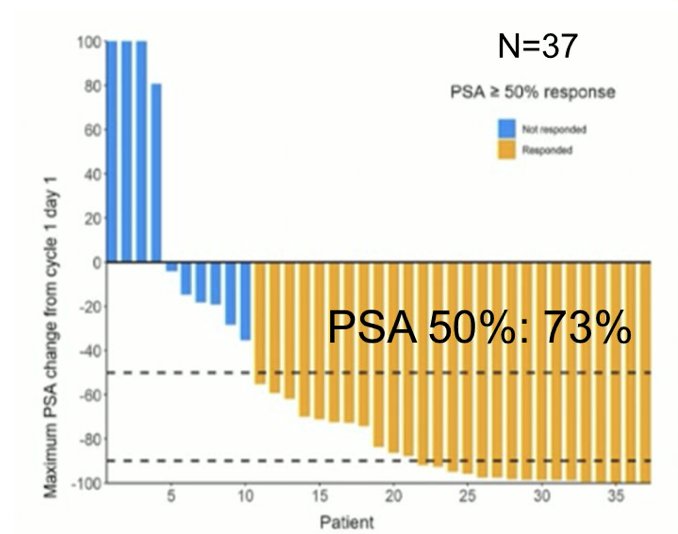
Another phase I trial assessed single dose 177Lu-PSMA-617 followed by maintenance pembrolizumab in patients with mCRPC: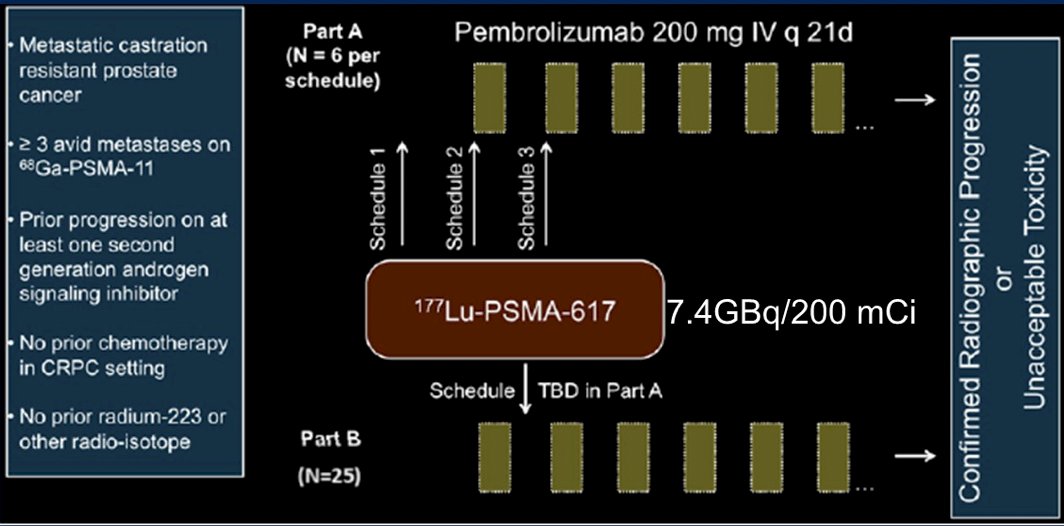
Part B had an objective response rate of 56% (14/25) and 5% (2/43) had a treatment-related adverse event of grade 3 or worse. There was one serious adverse event (one death due to aspiration pneumonia) and no treatment-related deaths were observed. Dr. Surasi also highlighted the phase II ongoing EVOLUTION trial, which is randomizing patients 2:1 to Arm A 177Lu-PSMA-617 + induction ipilimumab + nivolumab versus Arm B 177Lu-PSMA-617: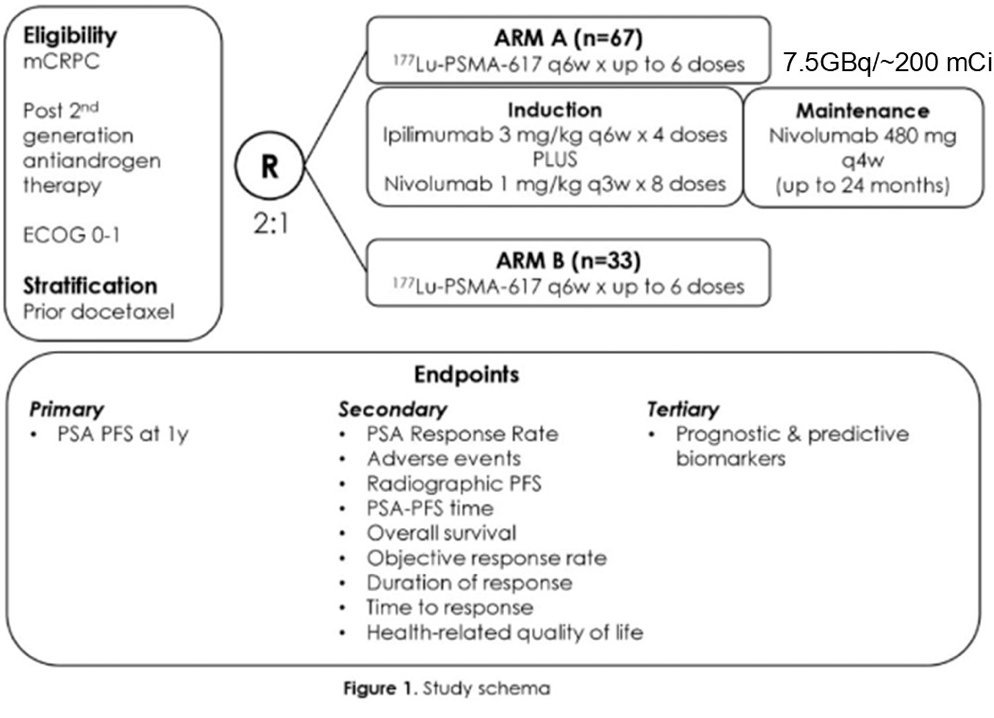
The primary endpoint of EVOLUTION is PSA progression free survival at 1 year.
Dr. Surasi then discussed alpha therapy, which has most commonly been utilized as radium-223 based on data from the ALSYMPCA trial.2 More recently, the alpha emitter Actinium-225 has been assessed in the retrospective multicenter study WARMTH Act,3 specifically 488 patients at 7 centers. Actinium-225 was associated with a median overall survival of 15.5 months and median progression free survival of 7.9 months. Any PSA decline was noted in 73% of patients, and PSA50 response was noted in 57% of patients.
The interim analysis of the RaLu study,4 published in 2023, showed that the median time between treatment with radium-223 and 177Lu-PSMA-617 therapy was 9.3 months (range: 0.9-41.9), with acceptable toxicity given the grade 3-4 treatment emergent adverse event rate was 41%. The median overall survival from the first radium-223 injection was 31.4 months, and the overall survival from the first 177Lu-PSMA-617 injection was 12.6 months. Thus, in patients with bone-predominant disease, radium-223 before 177Lu-PSMA-617 treatment was clinically feasible and well tolerated, with a similar survival outcome to those reported in previous studies:![The interim analysis of the RaLu study [4], published in 2023, showed that the median time between treatment with radium-223 and 177Lu-PSMA-617 therapy was 9.3 months (range: 0.9-41.9), with an acceptable toxicity given the grade 3-4 treatment emergent adverse event rate was 41%. The median overall survival from the first radium-223 injection was 31.4 months and the overall survival from the first 177Lu-PSMA-617 injection was 12.6 months. Thus, in patients with bone-predominant disease, radium-223 before 177Lu-PSMA-617 treatment was clinically feasible and well tolerated, with a similar survival outcome to those reported in previous studies:](/images/com-doc-importer/189-asco-gu-2025/asco-gu-2025-psma-based-therapy-in-advanced-disease-touching-on-combination-sequencing/image-12.jpg)
The phase I/II ongoing ALPHABET trial is testing the combination of 177Lu-PSMA-I&T + radium-223, with the co-primary objective of determining the maximum tolerated dose of radium-223 when combined with 177Lu-PSMA-I&T, and the PSA50 rate. Secondary objectives include adverse events, efficacy through radiographic and PSA progression free survival, overall survival and objective response rate, as well as evaluation of pain and health related quality of life. Recruitment for this trial commenced in September 2022.
Dr. Surasi concluded her presentation discussing combination sequencing for PSMA-based therapy in advanced disease with the following take-home points:
- 177Lu-PSMA radioligands are a promising new class of treatment
- The synergistic effects of combining 177Lu-PSMA with other therapeutic agents could offer new avenues for enhancing treatment efficacy.
- There is a need to optimize PSMA theranostics to balance the efficacy and toxicity.
- Continued research on predictors of response and mechanisms of resistance will inform rational combinations.
Presented by: Devaki S. Surasi, MBBS, CMQ, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Emmett L, Subramaniam S, Crumbaker M, et a. [177Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): An open-label, multicentre, randomized, phase 2 trial. Lancet Oncol. 2024 May;25(5):563-571.
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.
- Sathekge MM, Lawal IO, Bal C, et al. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): A multicentre, retrospective study. Lancet Oncol. 2024 Feb;25(2):175-183.
- Rahbar K, Essler M, Pabst KM, et al. Safety and Survival Outcomes of 177Lu-Prostate-Specific Membrane Antigen Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer with Prior 223Ra Treatment: The RALU Study. J Nucl Med. 2023 Apr;64(4):574-578.