(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Danny Cortes discussing radiographic criteria to assess response to radioligand therapy. Currently, theranostics relies on molecular imaging based selection criteria. In VISION, this was a visual approach: >= 1 PSMA-positive lesions anywhere in the body (uptake > liver). In TheraP, this required an SUVmax > 20. Dr. Cortes notes that we see is what we treat, and we treat is what we see:
PSMA uptake can assess therapy response. For lesions that have high lesion PSMA uptake, there is very low radioactive waste, whereas with low lesion PSMA uptake, there is high radioactive waste. At APCCC 2024, the experts were asked the question: In the majority of patients that you evaluate for 177Lu-PSMA therapy eligibility, what imaging do you routinely recommend, assuming all scans are readily available? A combined total of 100% voted in favor of PSMA PET imaging for evaluation of 177Lu-PSMA therapy eligibility.
According to PCWG3, imaging with bone scans and CT/MRI should be done every 12 weeks when assessing patients in metastatic prostate cancer clinical trials. But, does vintage imaging really help in assessing radioligand therapy? Dr. Cortes cautions that relying on a vintage imaging approach alone is not enough and PSMA PET imaging should also be incorporated:
RECIP 1.0 combines changes in PSMA positive total tumor volume and the occurrence of new lesions. Changes in total tumor volume can be determined quantitatively by using tumor segmentation software and combined with occurrence of new lesions to calculate quantitative RECIP. Changes in total tumor volume can be determined qualitatively by nuclear medicine physicians and combined with the occurrence of new lesions to calculate visual RECIP: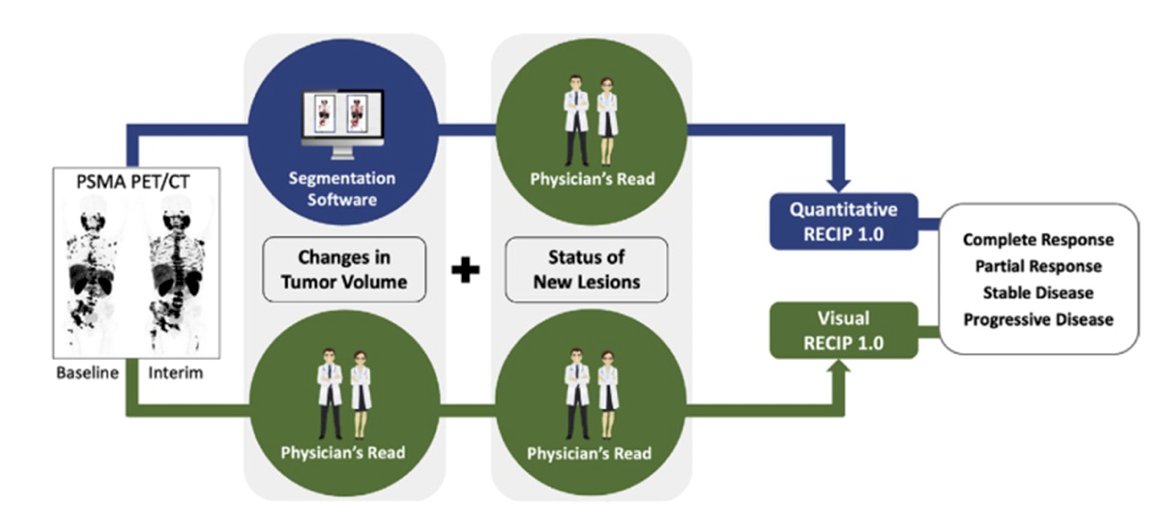
The following demonstrates utilization of RECIP 1.0 to delineate RECIP-PR (PSMA volume decline >=30% and no new lesions), RECIP-SD (PSMA volume decline >=30% and new lesions), and RECIP-PD (PSMA volume increase >=20% and new lesions):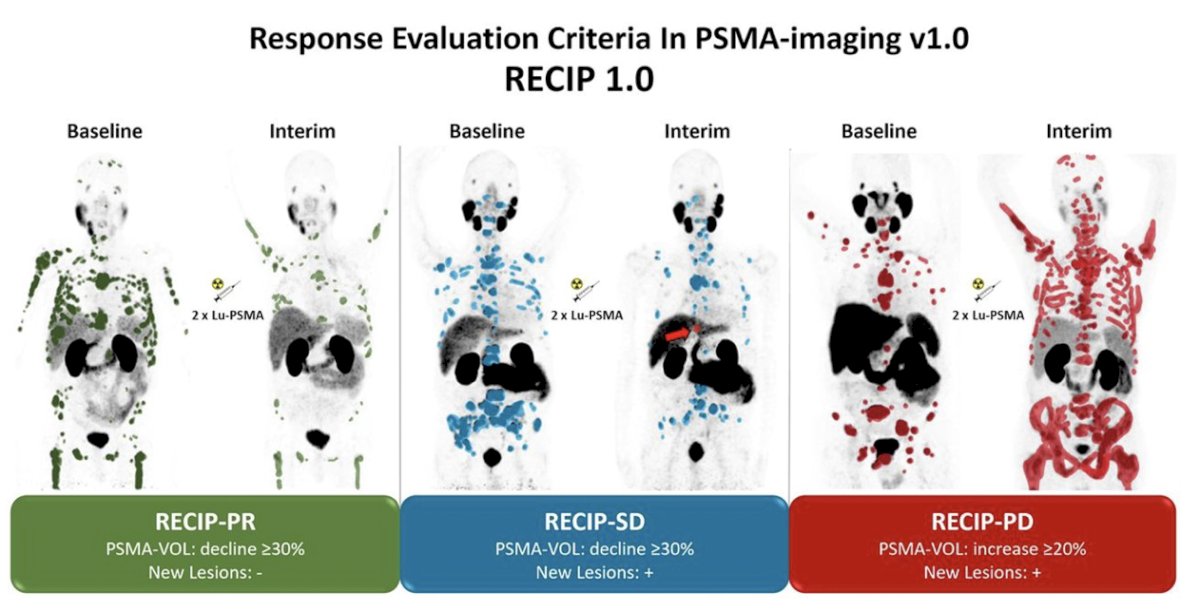
Dr. Cortes notes that PSMA PET/CT is being incorporated into PCWG4 using preliminary work from the PRINCE trial, with the goal of sparing patients the inconvenience of bone scans, switching to PSMA PET/CT, and making better decisions about stopping or changing treatments.
For patients ~24 hours after a cycle of 177Lu-PSMA therapy, SPECT is useful for assessing a change in radioligand therapy response, and may even predict progression free survival for patients undergoing 177Lu-PSMA therapy. A second question posed to the APCCC 2024 experts was: In the majority of patients on treatment with 177Lu-PSMA, which imaging modality do you recommend for response monitoring? There was no consensus in responses with 12% voting for LuPSMA SPECT/CT, 18% voting for conventional imaging, 22% voting for PSMA PET, 36% voting for PSMA PET + diagnostics, and 12% abstaining from voting.
Dr. Cortes notes that GBq from 177Lu-PSMA therapy transforms to Gy, with Gy representing real therapy effect when matched with radioligand therapy response: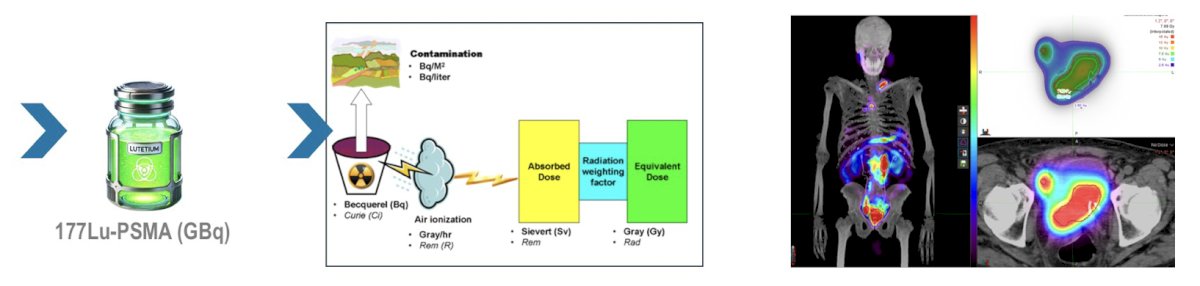
Thus, radioligand dosimetry is likely an effective way to assess response.
Dr. Cortes concluded his presentation discussing radiographic criteria to assess response to radioligand therapy with the following take-home points:
- Understanding the concept of radioligand therapy is essential to changing imaging response tools
- High PSMA uptake = high tumor absorbed dose
- Low PSMA uptake = low tumor absorbed dose and bad results
- A vintage imaging approach is not enough
- Next generation imaging (PSMA PET)/Lu-PSMA SPECT/CT represents real radioligand therapy evaluation
- Dosimetry results should be integrated into therapy response analysis
- We need to close the circle:

Presented by: Danny M. Cortes, Nuclear Medicine World, Mexico City, Mexico
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.