(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Case-Based Session: Management of Biochemical Recurrence After Radiation Therapy for Localized Prostate Cancer. Dr. Thomas Polascik discussed ablative therapies for Radio-recurrent Disease.
Dr. Polascik began his presentation by stating that when considering salvage therapies, several key assumptions have to be made. These include that cancer is still localized, with a positive prostate biopsy and a negative seminal vesicle biopsy. Additionally, it is assumed that the patient has a 10-year life expectancy and is willing to accept the risks and benefits associated with salvage treatments. He also emphasized that biologically more aggressive cancers are more susceptible to the morbidity related to salvage therapies, which complicates treatment decisions and outcomes.
It is important to estimate the incidence of radio-recurrent prostate cancer. Of approximately 65,000 cases treated with radiation therapy in 2018, assuming a biochemical recurrence (BCR) incidence of 25%, we would expect an incidence of around 16,000 new cases of radiation-resistant prostate cancer by 2025, seven years later. Therefore, radio-recurrent prostate cancer could be considered the fourth most common genitourinary malignancy in men, following primary prostate cancer, bladder cancer, and renal cell carcinoma.
The cumulative incidence of BCR varies significantly depending on the risk group category of patients. As illustrated in the table below, patients in the high D’Amico Risk group have a 36% (33% - 39%) cumulative BCR incidence (95% CI).1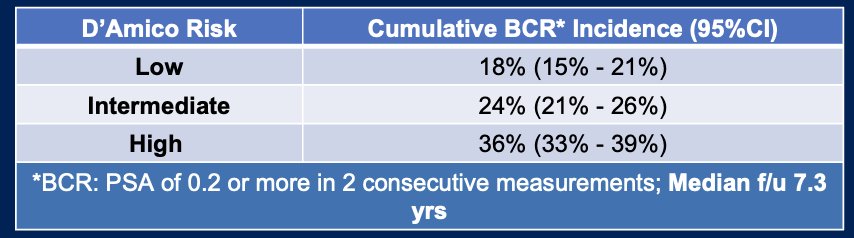
Dr. Polascik posed the question of why offer salvage ablative therapies. First, he showed data from studies with more than 100 cases, comparing incontinence rates. Notably, in patients who underwent salvage surgery, the incontinence rate ranged from 21% to 68%. In contrast, patients treated with salvage cryotherapy had incontinence rates (1-4 years of follow-up) ranging from 2% to 20%. Dr. Polascik pointed out that in more recent studies (from left to right), the results are improving in both groups.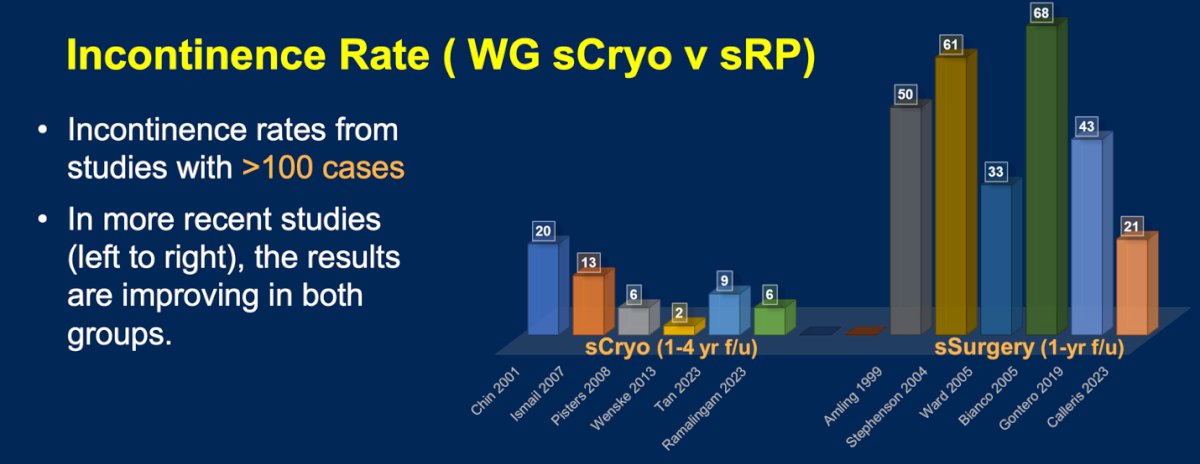
Moreover, the rectal injury rate comparing salvage surgery to salvage cryotherapy is also considerably higher. In studies with more than 100 cases, the rectal injury rates for salvage surgery range from 5% to 7%, while for salvage cryotherapy, the rates range from 1% to 3%, which is almost half the rate seen in surgery.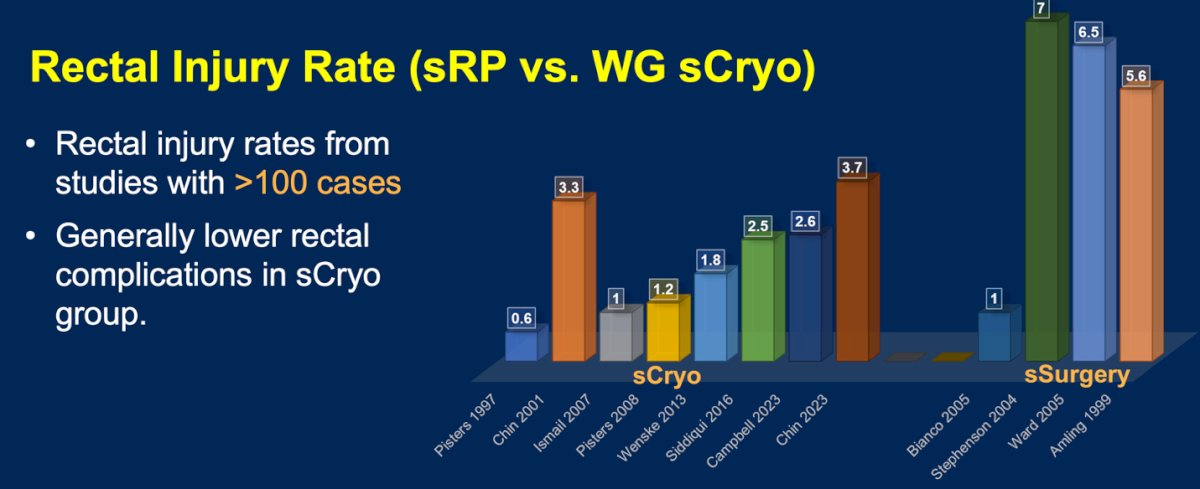
Patient selection remains a key factor for salvage ablative therapy, factors to be considered are:
- Life expectancy > 10 years
- Biopsy-confirmed local recurrence without distant metastasis
- Tumor size and location primarily determine whether whole-gland or focal salvage is appropriate
- PSA <10 ng/mL at recurrence (the lower, the better)
- A prolonged disease-free interval (>5 years) from radiation therapy is preferred
- No seminal vesicle invasion, PSA doubling time <12 months, or ill-defined extracapsular extension
It is important to carefully weigh the pros and cons of salvage ablative therapies for radio-recurrent prostate cancer. On the positive side, these therapies offer excellent continence outcomes, shorter recovery times, and earlier catheter removal, with most procedures being performed on an outpatient basis. However, there are several drawbacks to consider. PSA surveillance becomes more challenging post-treatment, and certain modalities have specific limitations. For example, High-Intensity Focused Ultrasound (HIFU) and Transurethral Ultrasound Ablation (TULSA) are not ideal options after brachytherapy, while cryotherapy may not be suitable in cases involving peri-urethral recurrence. Additionally, Irreversible Electroporation (IRE) is contraindicated for patients with pacemakers or large tumor volumes.
Dr. Polascik presented data from a systematic review and meta-analysis of salvage ablation for radiation-recurrent localized prostate cancer, conducted by the Focal Therapy Society. This analysis included 53 studies with a total of 7,842 patients, spanning from 1996 to 2023. The review comprised 45 retrospective studies and 8 prospective studies. Key study details included a median patient number of 87.5 (range: 13–898) and a median follow-up duration of 37 months. In terms of stage, 69% had Stage 2b (n=37), while 31% had Stage 4 (n=16).2
In terms of biochemical progression-free survival (BPFS), the 5- and 10-year BPFS for salvage whole gland ablation (sWGA) was 54% and 35%, respectively. In patients treated with salvage focal ablation (sFA), the 5-year BPFS was 50%, which is comparable to the whole gland approach. Notably, 34 studies reported the use of neo-adjuvant androgen deprivation therapy (neo-ADT), which was administered to 42% of the total study population, with a duration of 3 to 6 months. The 5-year BPFS was significantly different between patients who received neo-ADT and those who did not: 56% without neo-ADT versus 29% with neo-ADT (p < 0.01).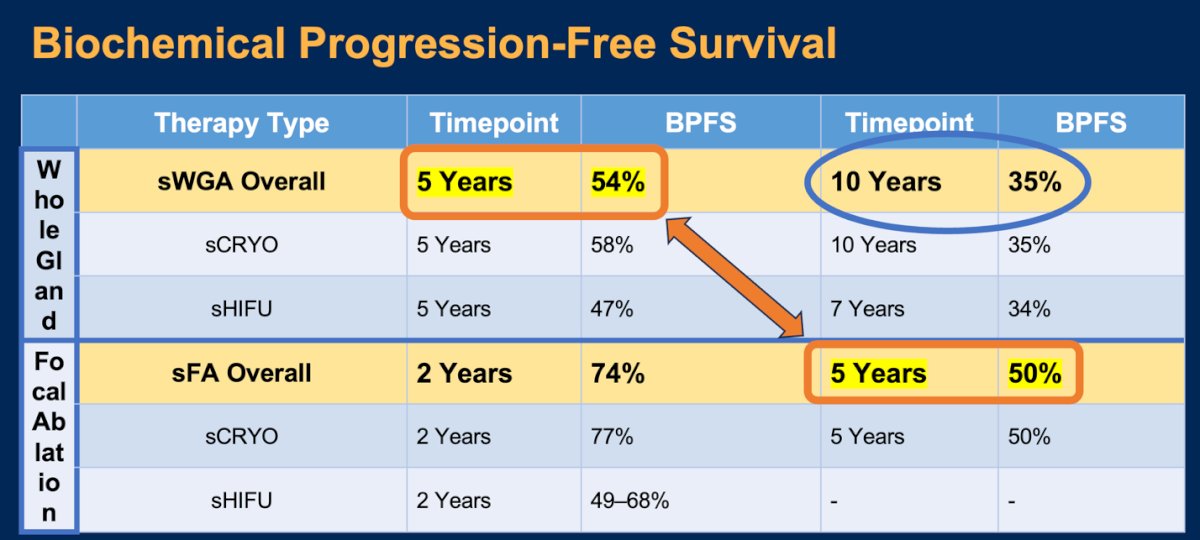
Progression-free survival, defined as no cancer on follow-up biopsy, metastasis, clinical recurrence, or need for additional treatment, was reported at 5 years in 50% of those treated with salvage whole gland ablation and 54% in those treated with salvage focal ablation, which is fairly similar.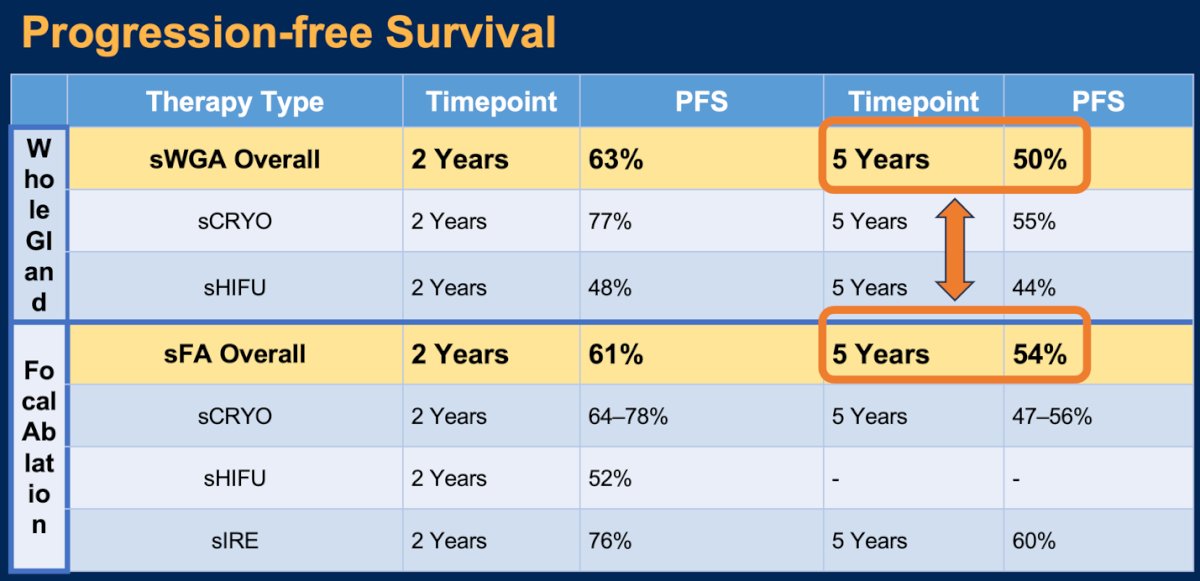
Notably, overall survival was also similar at 10 years of follow-up in patients treated with whole-gland cryotherapy and focal ablation cryotherapy, at 80% versus 83%, respectively.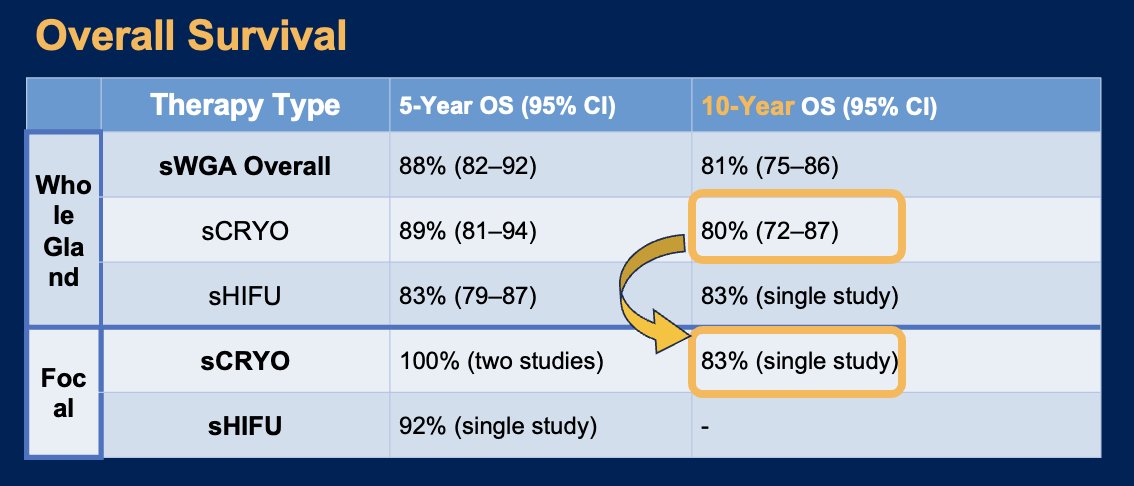
In terms of ablation-related morbidities, outcomes for urethral stricture, recto-urethral fistula, urethral sloughing, perineal pain, and urinary tract infections were similar when comparing salvage whole-gland ablation versus salvage focal ablation. However, urinary retention was more than double (13% vs. 6%) in patients treated with salvage whole-gland ablation.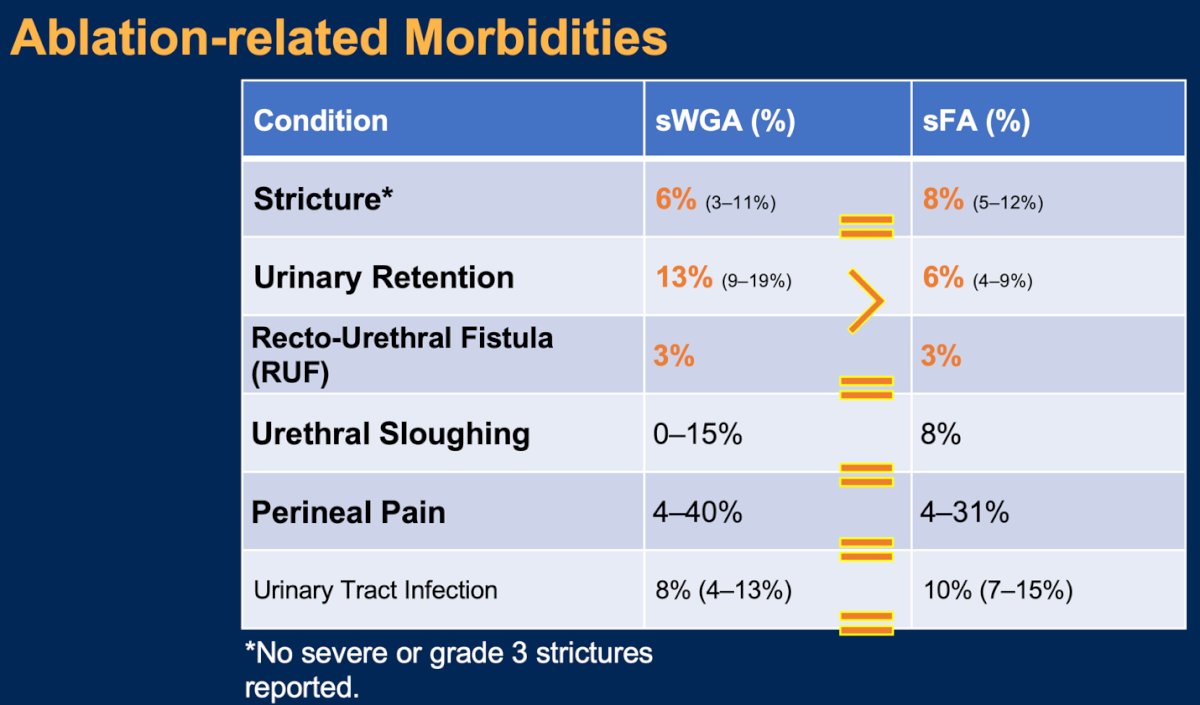
Lastly, Dr. Polascik discussed the functional outcomes associated with salvage focal ablative therapies. He noted that there was significant heterogeneity in functional outcomes for both whole-gland and focal ablation, which could be partially explained by the surgeon's experience. The pad-free rate in patients treated with salvage whole-gland ablation was 77%, compared to 85% in those treated with salvage focal ablation, as illustrated below. Rates of preserved erectile function were only reported for some focal therapy modalities, with 21% in patients treated with whole-gland cryotherapy versus 41% in those treated with focal ablation cryotherapy.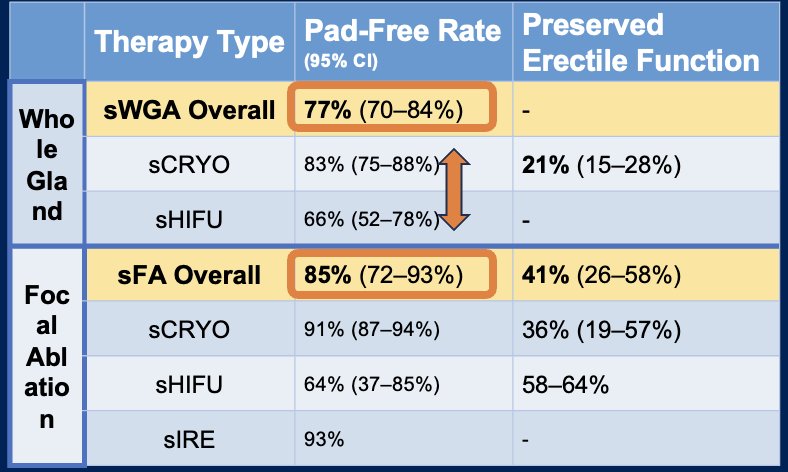
When comparing focal ablation in the primary versus salvage setting, Dr. Polascik emphasized that the patient needs to understand the differences between these two settings. Realistic expectations should be set, as prior radiation therapy affects function following ablation. He noted that primary focal ablation is superior in terms of metastasis-free survival, cancer-specific survival, and the pad-free rate at one year when compared to salvage whole-gland therapy.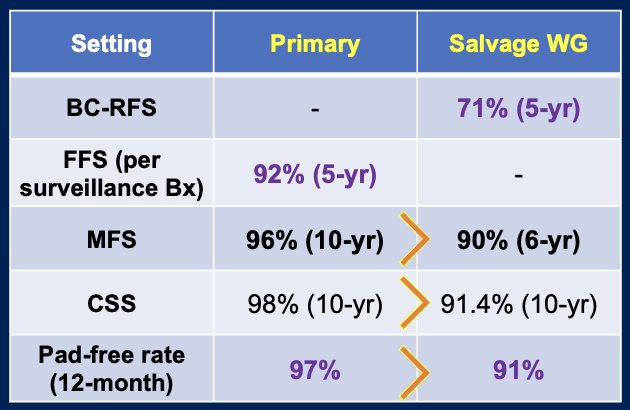
Dr. Polascik concluded his presentation with the following remarks:
- Radio-recurrent disease is biologically more aggressive, and patients are more susceptible to side effects.
- Biochemical progression-free survival shows higher rates for focal therapies at shorter timepoints, but long-term outcomes are comparable to whole-gland approaches.
- Overall survival (OS) outcomes are similar across modalities.
- In terms of morbidity, salvage focal ablation (sFA) shows better continence and erectile function.
- Future directions include the need for more cancer-targeted therapies, long-term trials, and advanced imaging to optimize treatment.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Falagario UG, Abbadi A, Remmers S, Björnebo L, Bogdanovic D, Martini A, Valdman A, Carrieri G, Menon M, Akre O, Eklund M, Nordström T, Grönberg H, Lantz A, Wiklund P. Biochemical Recurrence and Risk of Mortality Following Radiotherapy or Radical Prostatectomy. JAMA Netw Open. 2023 Sep 5;6(9):e2332900. doi: 10.1001/jamanetworkopen.2023.32900. PMID: 37695584; PMCID: PMC10495864.
- Deivasigamani, S., Rastinehad, A. R., Klotz, L., Lepor, H., Ahmed, H. U., Pinto, P., ... & Polascik, T. J. Systematic Review and Meta-Analysis of Salvage Ablation for Radiation-Recurrent Localized Prostate Cancer–A Focal Therapy Society Project.