(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Case-Based Session: Management of Biochemical Recurrence After Radiation Therapy for Localized Prostate Cancer. Dr. Ashley Ross discussed the management of biochemical recurrence after radiation therapy for localized prostate cancer with salvage prostatectomy.
Dr. Ross structured his presentation into five key topics: goals of salvage prostatectomy, patient selection criteria, expectations regarding cancer control and potential complications, basic principles of the procedure, special circumstances that may influence surgical decisions, and the future of salvage prostatectomy.
He began by stating that the goals of salvage prostatectomy include achieving cancer control, delaying disease progression and mortality, providing the possibility of cure, and limiting local symptoms associated with recurrent disease. However, salvage prostatectomy is not suitable for all patients, and appropriate patient selection remains critical. The most important factors for patient selection include good overall health, a performance status that allows for surgery, and a life expectancy of more than 10 years, with minimal comorbidities. Additionally, patients should not have metastatic disease or should have a low likelihood of metastasis. Historically, selection criteria included N0M0 status based on axial imaging and bone scans, PSA levels below 10 ng/mL, and clinical stage T1-T2 disease. However, with advancements in imaging, current selection criteria incorporate N0M0 status as determined by PSMA PET imaging, as well as confirmation of surgical resectability through MRI.
Moreover, candidates for salvage prostatectomy should not be ideal candidates for ablative therapies, and in many cases, ablative approaches are preferred, particularly when there are limited options for non-reconstructive treatments following salvage procedures. The patterns of recurrence after radiation therapy play a crucial role in determining the suitability of different salvage strategies. A study by Takeda et al. analyzed detailed prostate mapping in 77 men and found that recurrences frequently occur in challenging locations. Peri-urethral involvement was observed in 69% of cases, with 6.5% demonstrating direct urethral extension. Apical involvement was nearly universal, with 90% of cases showing some degree of apical recurrence and 32% involving the last 3 mm of the apex. Additionally, seminal vesicle invasion was present in 42% of cases, though isolated seminal vesicle involvement was rare, occurring in only 2.6% of patients.1 These patterns highlight the complexities of salvage treatment decision-making, as patients with significant peri-urethral or apical recurrence may not be suitable for salvage prostatectomy and may instead require ablative therapies.
A crucial question to ask ourselves and our patients is: what are the expectations of salvage prostatectomy? Undoubtedly, cancer control is a primary goal. Data from multiple series have shown that approximately the 5-year biochemical recurrence-free survival, metastasis-free survival, and cancer-specific survival rates are around 50%, 80%, and 95%, respectively, as illustrated in the table below.2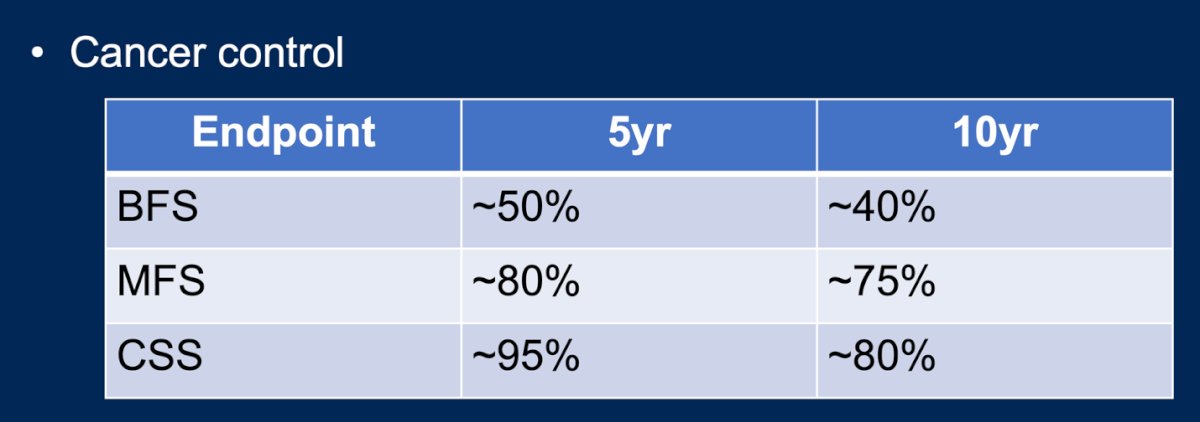
However, the treatment-associated morbidity should also be carefully balanced within the expectations of salvage prostatectomy. Morbidity remains high regardless of the surgical approach (open or minimally invasive). Reported rates of incontinence range between 30-60%, while erectile dysfunction occurs in the majority of patients (80-90%). Additionally, there is a risk of major complications in approximately 15% of cases, including rectal injury or fistula (1-4%) and urethral stricture (10-30%).3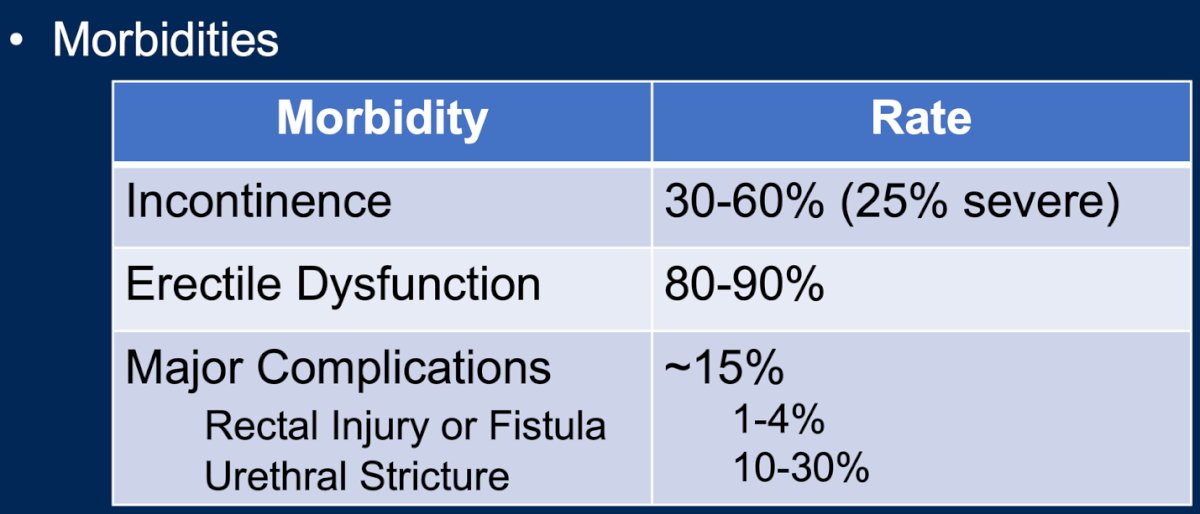
The basic principles of salvage prostatectomy should account for the challenges posed by devitalized tissue due to prior radiation, which increases the risk of anastomotic leaks (10-20%). To mitigate this, key considerations include leaving a drain, prolonging catheterization for 3-4 weeks, and performing a cystogram before catheter removal. Additionally, pelvic lymph node dissection (PLND) enhances staging accuracy, although its oncological benefit remains uncertain. Furthermore, if robotic surgery is available, it should be the preferred approach for salvage prostatectomy. A modern series of robotic salvage prostatectomy demonstrated significantly improved perioperative outcomes compared to open surgery, including:
- ~3x lower blood loos
- ~2x shorter hospital stay
- ~2x lower urethral stricture rates
- ~2.5x lower incontinence rates
- ~6x lower rectal injury risk (not statistically significant)
- ~5x lower wound infection risk (not statistically significant)4
Seminal vesicles can be an area of undertreatment in patients who have undergone radiation therapy, with 2-5% of post-radiation recurrences being isolated to the seminal vesicles. Robotic seminal vesiculectomy has been shown to be a feasible option for these patients, with very low complication rates. A study by Langley et al. demonstrated that the procedure typically involves an operative time of less than 2 hours and hospitalization of less than 24 hours. Additionally, there was no observed change in continence, and complications were minimal in the limited series of patients. The 3-year failure-free survival rate is approximately 50%, suggesting that robotic seminal vesiculectomy could be a viable treatment for this subset of patients with localized post-radiation recurrence.5
Dr. Ross discussed the case of a 74-year-old patient who had undergone external beam radiation therapy with a brachytherapy boost, as well as androgen deprivation therapy (ADT). The patient was now presenting with a PSA level of 2.4 ng/ml and a biopsy-proven recurrence, which was isolated to the seminal vesicles with Gleason Grade 5 (GG5) disease as shown in the image below. This is a good case to consider for robotic vesiculectomy.

Dr. Ross concluded his presentation by emphasizing the future directions of salvage prostatectomy, which should focus on improving continence outcomes. He pointed out that robot-assisted Retzius-sparing salvage prostatectomy may improve continence. Additionally, he highlighted the importance of better candidate identification, suggesting that image-based tissue perfusion measurement could play a role in optimizing patient selection and surgical outcomes.
Presented by: Ashley Ross, MD, PhD, Urologic Oncologist at Northwestern University Feinberg School of Medicine. Chicago, IL.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Takeda T, Tin AL, Corradi RB, Mamoor M, Benfante NE, Sjoberg DD, Scardino PT, Eastham JA, Fine SW, Touijer KA. Topography of Prostate Cancer Recurrence After Radiation Therapy: A Detailed Mapping Study of Salvage Radical Prostatectomy Specimens. Eur Urol. 2018 Apr;73(4):488-490. doi: 10.1016/j.eururo.2017.08.005. Epub 2017 Aug 26. PMID: 28851581; PMCID: PMC6050029.
- Calleris G, Marra G, Benfant N, Rajwa P, Ahmed M, Abreu A, Cacciamani G, Ghoreifi A, Ribeiro L, Westhofen T, Tourinho-Barbosa R, Raskin Y, Veerman H, Albisinni S, Smith JA, Rouprêt M, Oderda M, Massari E, Persad R, Van Der Poel H, Joniau S, Sanchez-Salas R, Kretschmer A, Cathcart P, Gill I, Karnes RJ, Tilki D, Shariat SF, Touijer K, Gontero P. Salvage Radical Prostatectomy for Recurrent Prostate Cancer Following First-line Nonsurgical Treatment: Validation of the European Association of Urology Criteria in a Large, Multicenter, Contemporary Cohort. Eur Urol Focus. 2023 Jul;9(4):645-649. doi: 10.1016/j.euf.2023.01.006. Epub 2023 Jan 20. PMID: 36682962.
- Marra G, Marquis A, Yanagisawa T, Shariat SF, Touijer K, Gontero P. Salvage Radical Prostatectomy for Recurrent Prostate Cancer After Primary Nonsurgical Treatment: An Updated Systematic Review. Eur Urol Focus. 2023 Mar;9(2):251-257. doi: 10.1016/j.euf.2023.01.013. Epub 2023 Feb 22. PMID: 36822924.
- Gontero P, Marra G, Alessio P, Filippini C, Oderda M, Munoz F, Linares E, Sanchez-Salas R, Challacombe B, Dasgupta P, Goonewardene S, Popert R, Cahill D, Gillatt D, Persad R, Palou J, Joniau S, Piechaud T, Morlacco A, Vidit S, Rouprêt M, De La Taille A, Albisinni S, Gandaglia G, Mottrie A, Joshi S, Fiscus G, Berger A, Aron M, Van Der Poel H, Tilki D, Lawrentschuk N, Murphy DG, Leung G, Davis J, Karnes RJ; Collaborators. Salvage Radical Prostatectomy for Recurrent Prostate Cancer: Morbidity and Functional Outcomes from a Large Multicenter Series of Open versus Robotic Approaches. J Urol. 2019 Oct;202(4):725-731. doi: 10.1097/JU.0000000000000327. Epub 2019 Sep 6. PMID: 31075058.
- Langley S, Eden C, Perry M, Patil K, Moschonas D, Higgins D, Deering C, Laing R, Perna C, Khaksar S, Uribe-Lewis S, Uribe J. Robot-assisted salvage seminal vesicle excision for isolated recurrence after low-dose-rate prostate brachytherapy. BJU Int. 2022 Jun;129(6):731-736. doi: 10.1111/bju.15586. Epub 2021 Sep 14. PMID: 34460980.