(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a rapid oral abstract prostate cancer session. Dr. Tamim Niazi presented GROUQ-PCS 9, a randomized phase II trial of metastasis-directed therapy in addition to standard systemic therapy in oligometastatic castration resistant prostate cancer (omCRPC).
Dr. Niazi noted that ADT + enzalutamide is one of the standard options for androgen receptor pathway inhibitor (ARPI)-naive mCRPC patients.1,2 PCS 9 was designed to evaluate the role of MDT (Stereotactic body radiotherapy (SBRT)) addition to standard of care therapy to provide an additional treatment option for omCRPC patients.
This trial was originally designed as an adaptive phase II/III randomized study. However, due to ARPI becoming standard of care in the castration sensitive setting during the study enrollment period, the recruitment of ARPI-naïve patients to this trial became increasingly challenging. As such, the trial was halted at the phase II stage, and results herein were reported for 100 omCRPC patients.
The study design is summarized below:
This trial included mCRPC patients with 1–5 metastases, who had received no prior ARPIs (docetaxel in hormone-sensitive setting was permitted), and were planned for therapy in the 1st line castrate-resistant setting. Eligible patients underwent 1:1 randomization to:
- Enzalutamide 160 mg + ADT
- Enzalutamide 160 mg + ADT + MDT (SBRT)
The primary endpoint was investigator-assessed rPFS. Key secondary endpoints were:
- Biochemical progression-free survival
- Time to subsequent therapy
- Health-related quality of life
- Safety and tolerability
- Overall survival
The two treatment arms were well-balanced for baseline patient demographics. The median age was 72 years in both arms. 43% of patients had undergone a prior radical prostatectomy, and ~80% had received radiotherapy to the prostate or prostate bed. 85-90% of patients had <4 metastases. The most common location of metastases was bone (62–75%), followed by lymph nodes (21–33%).
With regards to the primary endpoint, the addition of SBRT to enzalutamide + ADT was associated with a 52% risk reduction in radiological progression or death (HR: 0.48, 95% CI: 0.27–0.86, p=0.014). There was a 2.3-year improvement in rPFS with the addition of SBRT to systemic therapy.
The addition of SBRT to ADT + enzalutamide reduced the risk of biochemical progression or death by 42% (HR: 0.58, 95% CI: 0.32–1.03, p=0.065). This corresponded to a 1.5-year median improvement in biochemical progression-free survival.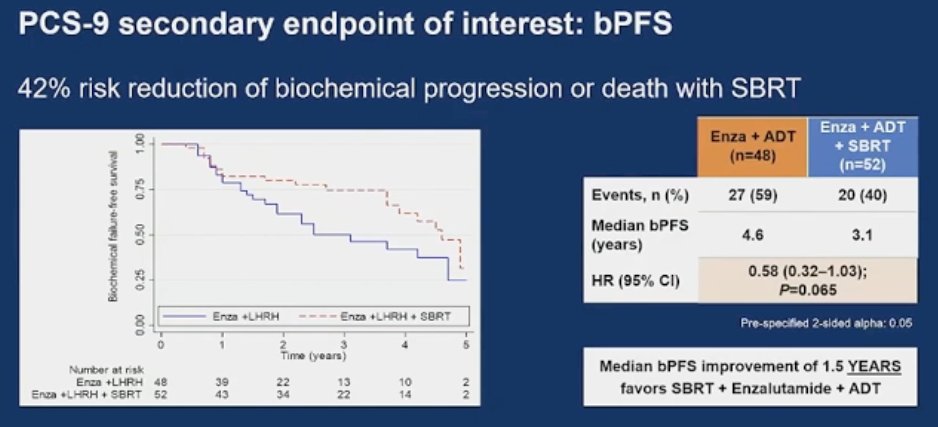
Patients in the SBRT arm had a 58% risk reduction in time to subsequent line of therapy (HR: 0.42, 95% CI: 0.22-0.8, p=0.009). This corresponded to a 2.2-year delay in time to subsequent line of therapy.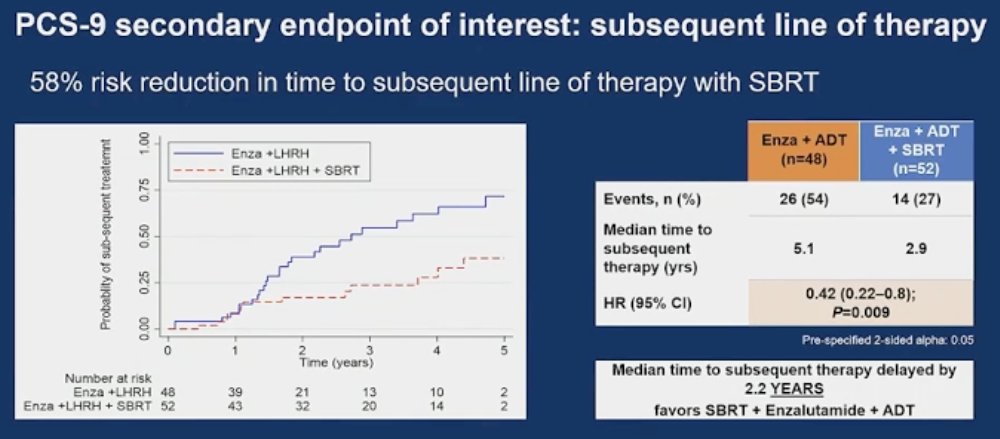
Overall survival was improved by 29% in the SBRT arm, albeit not statistically significant and data for overall survival is not mature yet (HR: 0.71, 95% CI: 0.31–1.59, p=0.407).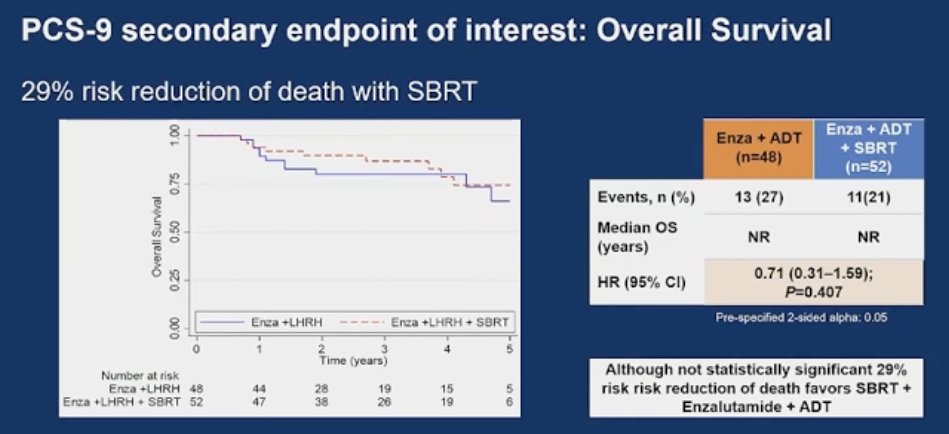
The adverse event profile was consistent with that of enzalutamide. Pain at the SBRT site was reported by 4 patients (7.7%), and one (2%) experienced asymptomatic pneumonitis.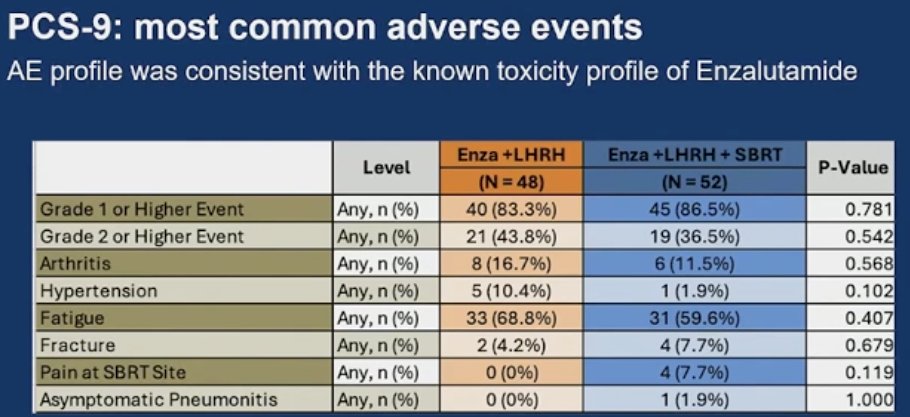
Dr. Niazi concluded as follows:
- The addition of SBRT to enzalutamide +ADT in ARPI-naïve oligometastatic CRPC patients led to a statistically and clinically meaningful improvement in rPFS (HR: 0.48, 95% CI: 0.27–0.86): 4.6 versus 2.3 years
- Secondary and exploratory endpoints support the treatment benefit of SBRT + enzalutamide + ADT over enzalutamide + ADT alone
- The safety profile of SBRT + enzalutamide + ADT was consistent with the safety profile of enzalutamide + ADT
- MDT using SBRT should strongly be considered for CRPC patients with oligometastases
Presented by: Tamim Niazi, MD, Associate Professor, Department of Oncology, Division of Radiation Oncology, Jewish General Hospital, University of McGill, Montreal, QC
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Scher HI, Fizazi K, Saad F, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med 2012; 367:1187-1197.
- Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 2014; 371(5):424-433.