(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Louise Emmett discussing overall survival and quality of life in ENZA-p with 177Lu-PSMA-617 (LuPSMA) plus enzalutamide versus enzalutamide alone in poor-risk, metastatic castration-resistant prostate cancer (mCRPC).
The interim analysis of ENZA-p, with a median follow-up 20 months, showed improved PSA progression free survival and depth of PSA-response with the addition of LuPSMA to enzalutamide as first-line treatment of poor-risk, mCRPC.1 Recently, we have seen in PSMAfore a radiographic progression free survival benefit (HR 0.49, 95% CI 0.39-0.61) for patients receiving LuPSMA in the pre-taxane chemotherapy mCRPC disease space, but no survival benefit (HR 0.98, 95% CI 0.75-1.28) secondary to the control arm crossing over to receive LuPSMA:2
At GU ASCO 2025, Dr. Emmett and colleagues reported effects on overall survival and health-related quality of life with longer follow-up.
ENZA-p randomly assigned 162 participants to enzalutamide 160 mg daily alone, or in combination with (2 or 4 doses) LuPSMA 7.5 GBq. Eligible participants had mCRPC not previously treated with chemotherapy or an androgen receptor pathway inhibitor for mCRPC, 68Ga-PSMA PET-avid disease, and at least 2 risk factors (LDH >= ULN, ALP >= ULN, albumin <35 g/L, de novo metastatic disease at diagnosis, <3 years since initial diagnosis, >5 bone metastasis, visceral metastasis, PSA doubling time < 84 days, pain requiring opiates > 14 days, prior abiraterone) for early disease progression on enzalutamide-alone:
Health-related quality of life was to be rated with the EORTC core quality-of-life questionnaire every 6 weeks until radiological progression. Deterioration-free survival was from random assignment until the earliest of death, clinical progression, discontinuation of study treatment, or a worsening of 10 points or more from baseline in physical function, or in overall health and quality of life. Health-related quality of life scores were analyzed with repeated measures modeling to calculate group means and differences. Health-related quality of life scores range from 0 (lowest possible) to 100 (highest possible). Time to event data were analyzed with the Kaplan-Meier method, stratified log rank test, and stratified Cox-proportional hazards regression.
A total of 96 deaths were reported after a median follow-up of 34 months (IQR 29-39): 53 among those assigned enzalutamide-alone and 43 among those assigned enzalutamide + LuPSMA. Overall survival was longer in the enzalutamide + LuPSMA group than the enzalutamide-alone group: median 34 months versus 26 months (HR 0.55, 95% CI 0.36 to 0.84; p = 0.005):
There were 30 of 79 (38%) participants in the enzalutamide-alone arm that received subsequent LuPSMA off trial.
Health-related quality of life was rated by 154 of 162 participants (95%). With regards to deterioration-free survival, this favored enzalutamide + LuPSMA for both physical function (HR 0.51, 95% CI 0.36 – 0.72) and overall health status (HR 0.47, 95% CI 0.33 – 0.67):
Mean scores for pain until progression favored the enzalutamide + LuPSMA group over the enzalutamide-alone group (difference 7.3, 95% CI 1.6 to 13; p = 0.01). Mean scores for fatigue until progression favored the enzalutamide + LuPSMA group over the enzalutamide-alone group (difference 5.9, 95% CI 1.1 to 11; p = 0.02):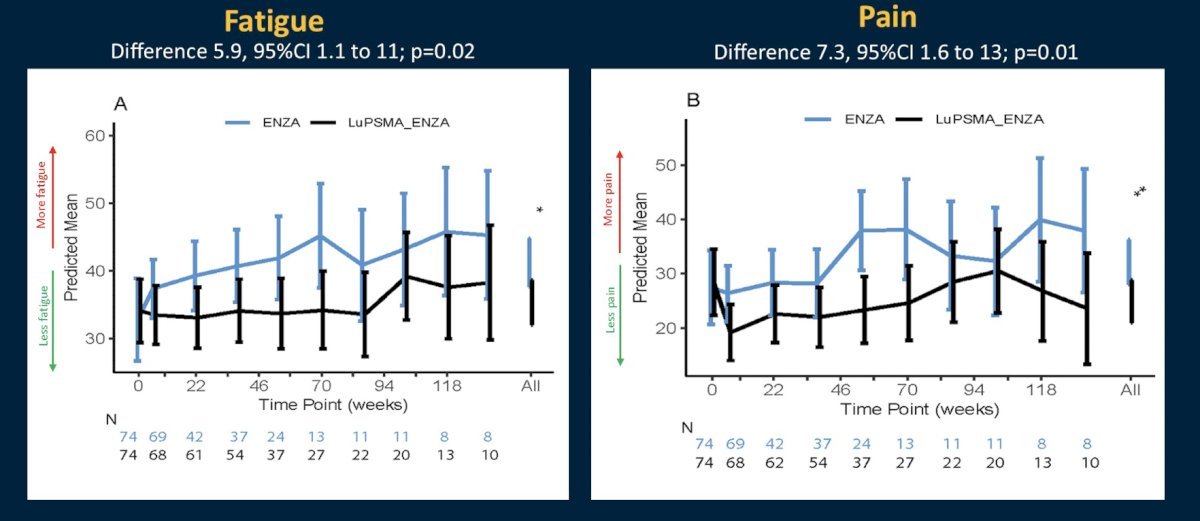
The frequency of self-rated xerostomia was lower in the enzalutamide-alone group (74% versus 57%; p = 0.04). Dr. Emmett notes several limitations from this analysis of ENZA-p: (i) utilization of first line enzalutamide in the early mCRPC pre-chemotherapy setting, (ii) this is a selective population, (iii) may limit the broad applicability of these findings. Future directions include whether PSMA radioligand therapy in prostate cancer should be administered more broadly in conjunction with androgen receptor pathway inhibitors? If so, this would pave the way for phase III trials leveraging these complementary therapies.
Dr. Emmett concluded her presentation discussing overall survival and quality of life in ENZA-p with LuPSMA plus enzalutamide versus enzalutamide alone in poor-risk mCRPC with the following take-home points:
- Combining 177Lu-PSMA-617 and enzalutamide significantly improves overall survival in men with mCRPC and risk factors for early treatment failure on enzalutamide alone
- This is an 8 month overall survival benefit compared to an active comparator arm
- The combination improved both deterioration free survival and health related quality of life indicators for pain, fatigue, physical function, and overall health and quality of life.
This data from this presentation of ENZA-p was concomitantly published in Lancet Oncology.
Presented by: Louise Emmett, MD, MBChB, FRACP, FAANMS, St Vincent's Hospital, Sydney, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References: