(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to the Keynote Presentation. Dr. William Dahut discussed how to drive science to improve patient-centered care.
Dr. Dahut highlighted the American Cancer Society's (ACS) integrated approach, which includes over $517 million in grants for cancer research across the U.S., advocacy at all levels of government in all 50 states, and patient support impacting more than 20,000 communities.
ACS has introduced EDS Accelerator Grants, aimed at funding key experiments necessary for product commercialization (e.g., drugs, diagnostics). Eligibility is currently limited to ACS-funded researchers in the first iteration. Grants provide up to $75,000, with a rolling submission process, monthly reviews, and funding for one project per month.
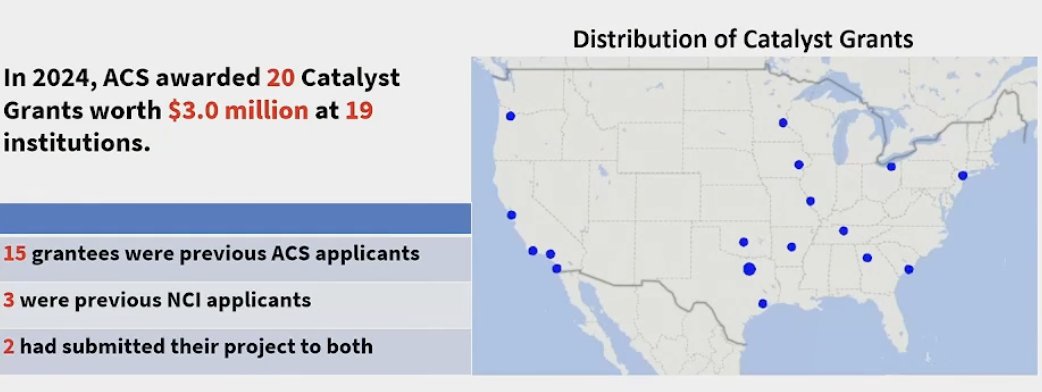
Additionally, ACS launched Catalyst Grants, awarding over $3 million in 2024 alone across 20 grants distributed among 19 institutions.
ACS is particularly interested in funding projects focused on individuals at high risk of developing prostate cancer and those with a higher risk of prostate cancer mortality, including minority groups. These initiatives fall under the Cancer Health Equity Research Centers (CHERC). Since 2021, ACS has awarded eight CHERC grants totaling $32.7 million.
Additionally, ACS is deeply committed to fostering the next generation of cancer researchers. They aim to provide training opportunities for individuals at all levels, including high school and college students, as well as research fellows. This initiative seeks to build a diverse and inclusive research community, ensuring that those who may not have had access to such opportunities can eventually become future collaborators in the field.
Dr. Dahut highlighted the annual report published by the ACS, noting key findings for 2025. These include a rising cancer incidence among women, a decline among men, and persistent racial disparities in cancer mortality.
He also referenced a publication from the COVID era that examined PSA testing rates among men by race and ethnicity. Strikingly, the study found that only 25% of men had undergone a PSA test, underscoring significant gaps in prostate cancer screening and early detection.
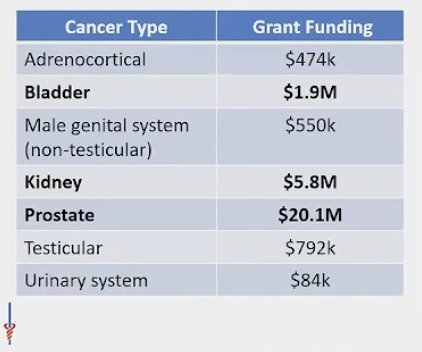
He then shifted focus to genitourinary (GU) cancers, discussing ACS’s current funding efforts. At present, ACS is supporting 76 grants related, at least in part, to GU cancers, with $29.7 million in funding allocated specifically to research in this area and distributed as shown below:
ACS prioritized prostate cancer for its clinical trial enrollment initiatives due to significant disparities in mortality, rising incidence, and an increasing number of men presenting with advanced disease despite a flattening of mortality rate improvements. Focusing on prostate cancer allows for targeted solutions within a more defined patient population, as it affects only adult males, and many physicians treating prostate cancer also manage other GU malignancies, facilitating a broader impact. By concentrating efforts on a single tumor type, ACS aims to refine effective strategies for improving clinical trial participation and amplifying successful approaches across oncology.
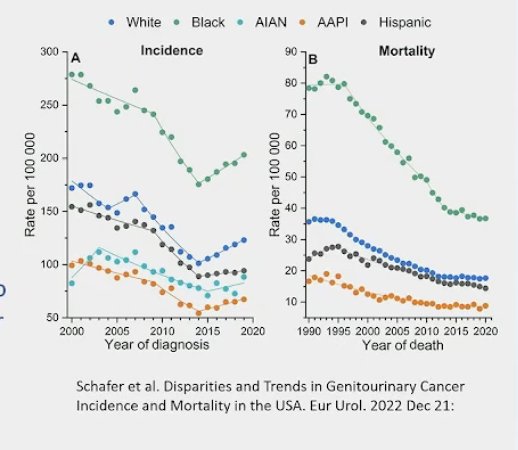
Prostate cancer incidence has increased over time, primarily driven by a rise in regional and localized disease. This trend underscores the need for improved early detection and management strategies. Notably, mortality rates remain highest among Black patients, highlighting persistent racial disparities in outcomes and the need for targeted interventions to address these inequities.1
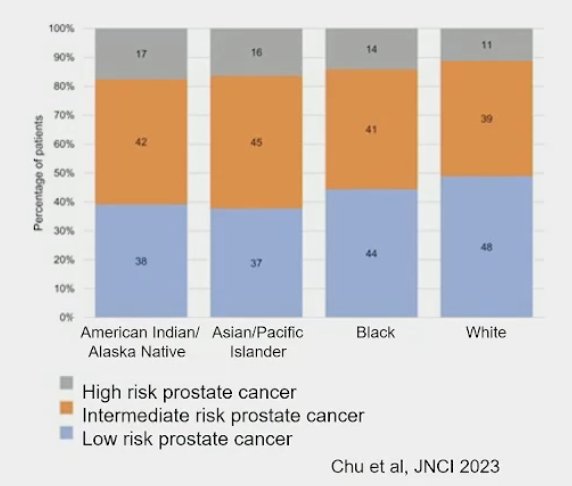
Among prostate cancer patients, American Indian/Alaska Native individuals face significant disparities, including a higher likelihood of living in rural areas with limited access to oncology care and being diagnosed with more advanced, high-risk disease. Only 38% are diagnosed with localized prostate cancer, and they are less likely to receive definitive therapy, contributing to poorer cancer survival outcomes. These disparities emphasize the urgent need for targeted efforts to improve early detection, access to treatment, and overall cancer care in this population.
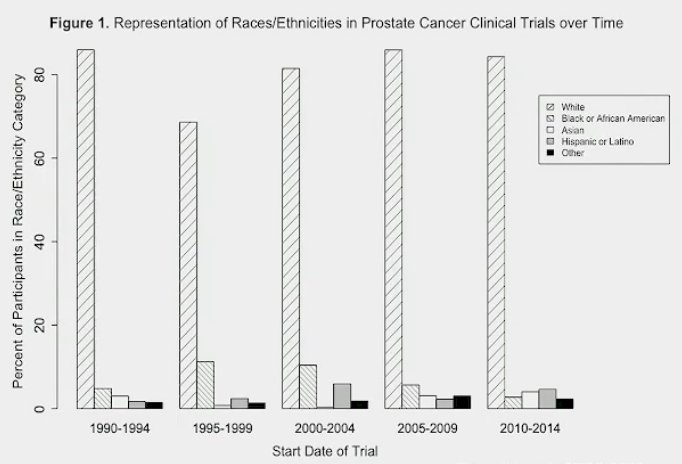
There is substantial evidence highlighting the lack of diversity in prostate cancer clinical trials. Among 70 Phase III randomized trials involving 893,000 participants, 19% did not report race or ethnicity data, and an overwhelming 96% of participants were White. Notably, individuals from the Caribbean and Africa were significantly underrepresented. This lack of diversity limits the generalizability of trial findings and underscores the need for more inclusive enrollment strategies to ensure equitable advancements in prostate cancer treatment
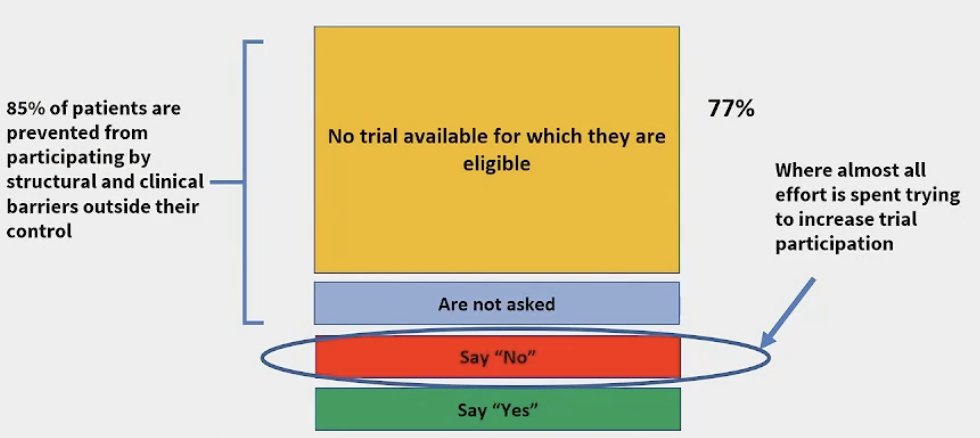
Barriers to improving diversity in prostate cancer trials include limited trial availability (77% of cases), a lack of direct invitations for patients to participate, and structural inequities in trial access. While some patients decline participation, many are never given the opportunity to enroll. Efforts to address this issue primarily focus on increasing trial participation, but a more comprehensive approach is needed—one that includes expanding trial availability, actively engaging underrepresented populations, and addressing systemic barriers to access and awareness.
Barriers to enrollment in prostate cancer clinical trials vary by institution type, with more opportunities available at academic centers than community sites. While 55% of patients offered a trial will accept, acceptance rates do not significantly differ by race. Among those who decline, reasons include both pragmatic barriers (cost, time, transportation) and philosophical concerns (mistrust, aversion to randomization). To address these issues, ACS CAN is focused on overcoming logistical challenges, and the ACS is launching the Prostate Cancer Clinical Trials Community Expansion Grants to improve trial accessibility and participation.
Artificial IntelligenceAI can have an initial impact on preclinical target and drug discovery, imaging and pathologic stratification, prognosis, and clinical predictions, ultimately improving patient care. It also holds promise for reducing healthcare disparities and increasing access to quality treatment. A recent ASCO publication highlighted how AI integration into prostate cancer care can enhance clinical decision-making, improve early detection, and enable personalized treatment strategies. In metastatic prostate cancer, AI-facilitated quantification of metastatic burden remains an active area of research with significant potential benefits.4
Dr. Dahut discussed the Artera AI model, which aids clinicians and patients in making personalized treatment decisions. The initial study utilized image data from over 5,000 patients across five Phase 3 randomized trials with long-term follow-up, involving patients from more than 100 centers in the US and Canada. The model serves as both a prognostic and predictive tool, helping guide clinical decisions. He emphasized that this technology has the potential to transform how prostate cancer treatment is approached.2
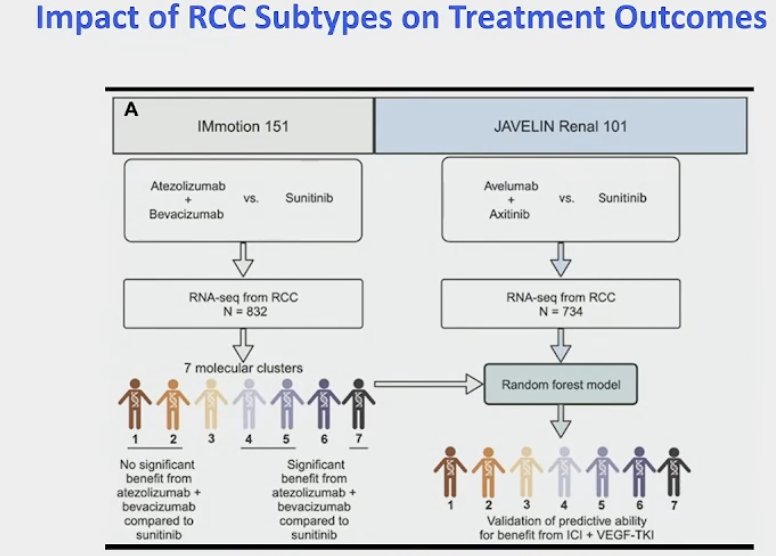
He then discussed a study that utilized transcriptomic data from the IMmotion 151 trial to predict outcomes in the JAVELIN Renal 101 trial for renal cancer. Using machine learning, the study aimed to determine the impact of RCC subtypes on treatment outcomes, highlighting the potential of AI-driven approaches in refining treatment selection and improving patient stratification.
Pathology is expected to be one of the areas where AI will have the greatest impact in the near future. Dr. Dahut briefly discussed an ACS-funded publication introducing the Clinical Histopathology Imaging Evaluation Foundation (CHIEF) model, a novel weakly supervised machine learning framework designed for cancer diagnosis and prognosis prediction. He emphasized the importance of selecting the appropriate AI techniques and highlighted ACS-funded patient-centric AI grants (below), which will continue to play a crucial role as innovation progresses.
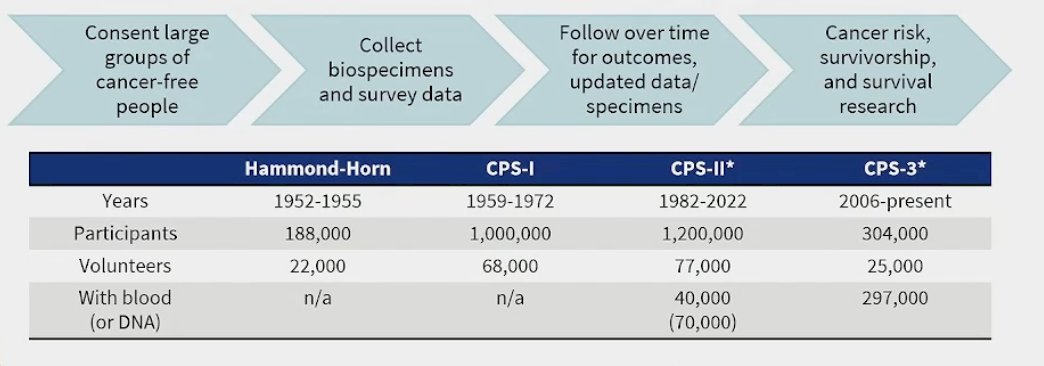
Dr. Dahut highlighted that the ACS has been conducting cohort studies since the 1950s, making significant contributions to cancer prevention research. Over the past 70 years, ACS has led some of the world’s largest prospective epidemiologic cohort studies to identify cancer risk factors, including the landmark association between tobacco and cancer. These cancer prevention studies have generated vast amounts of valuable data. He emphasized the need to make this data more accessible and practical and how AI could have a major role in this.
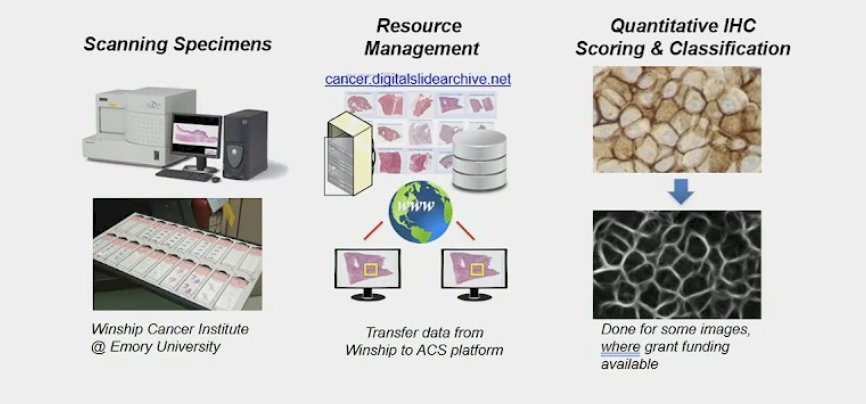
Dr. Dahut discussed a shared digital pathology resource developed in collaboration with Emory, where specimens were scanned for resource management and analysis, not only focusing on cancerous tissue but also examining benign areas. This initiative led to the development of HiPS, a novel AI tool created using digital tumor tissue images from CPS-II, CPS-3, and PLCO studies. HiPS is the first tool to integrate both cancerous and non-cancerous cell patterns to predict outcomes in invasive breast cancer. It analyzes 26 properties to generate an overall prognostic score, along with individual scores for cancer, immune, and stromal cells. Notably, HiPS has demonstrated superior predictive accuracy for patient outcomes compared to traditional methods, offering potential applications for personalized treatment planning.
Another critical application of AI is in data abstraction, addressing the vast amount of information that needs to be processed. ACS Cancer Prevention Studies are leading efforts to validate an AI-powered platform designed to accelerate high-quality chart abstraction, enabling research on a much larger scale and at greater speed. This platform extracts ~70 data elements and has already processed over 1,500 charts with an accuracy of 98–100%, matching or surpassing human performance. Notably, AI reduces the time required for data abstraction from months to mere hours, significantly enhancing research efficiency.
He then discussed a study evaluating the adenoma detection rate, a key predictor of colorectal cancer. Detecting adenomas during colonoscopy is crucial, as it directly impacts cancer prevention.1 AI has revolutionized this process by introducing CADe alert boxes that identify polyps in real time during colonoscopy. Previously, there was no standardized quality control in colonoscopy, but AI now enhances both detection accuracy and predictive capabilities, helping identify polyps more likely to be malignant.
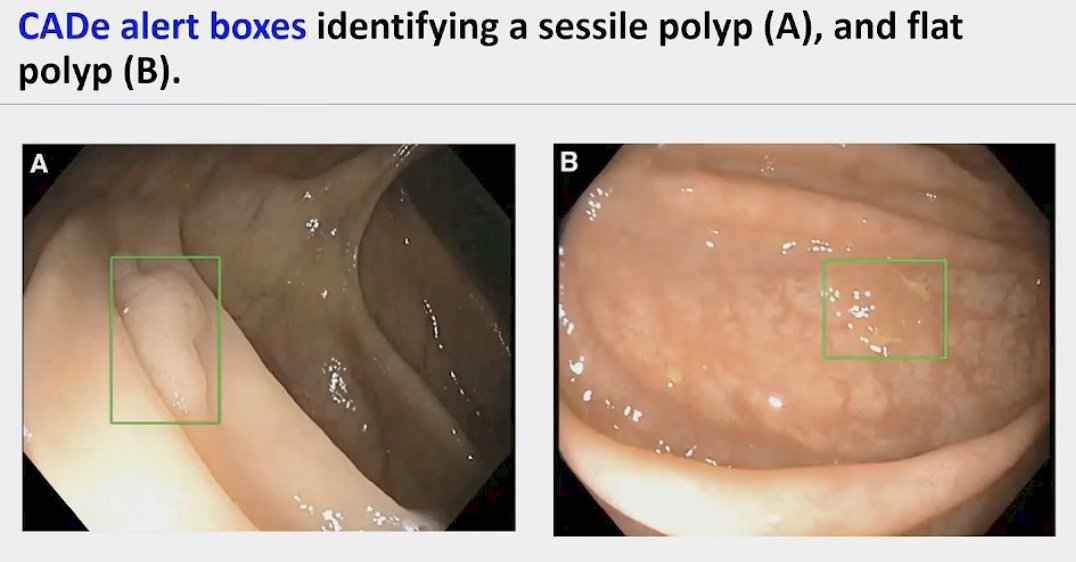
Studies have shown that adenoma and polyp detection rates decline as the day progresses, likely due to operator fatigue. Later colonoscopy sessions were associated with a significant decrease in adenoma detection rates (ADR early vs. late: 13.73% vs. 5.70%; P = .005; OR, 2.42; 95% CI, 1.31-4.47). However, with the assistance of AI systems, no such decline was observed in ADR or polyp detection. These findings suggest that AI could mitigate time- and workload-related degradation in colonoscopy quality, ensuring consistent detection rates regardless of the time of day.
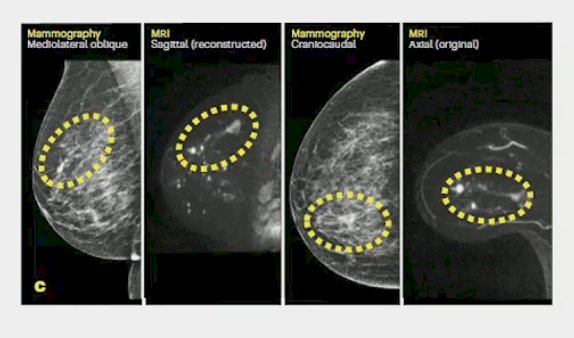
In Breast cancer, Among 88,844 screened women, those triaged to MRI using the AI tool had a cancer detection rate of 64.4 cancers per 1,000 MRI examinations. The positive predictive value (PPV) was 38% for individuals recalled after MRI and 50.7% for those who underwent biopsy, highlighting AI’s potential in improving triage accuracy and optimizing breast cancer screening.
Despite AI’s potential to enhance patient care, significant barriers to clinical adoption remain. There are concerns about clinician and patient trust in AI systems and the requirements needed to establish that trust. While AI technology is advancing rapidly, there is a growing record of overpromised performance. A key challenge for clinical integration is determining how machine learning interventions are incorporated into clinical trials and healthcare practice guidelines.
Dr. Dahut wrapped up his presentation by saying that we should amplify each other's humanity, prioritize patients and caregivers, and commit to excellence in our work.
Presented by: William L. Dahut, MD, Chief Scientific Officer for the American Cancer Society (ACS), Maryland, United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Schafer EJ, Jemal A, Wiese D, Sung H, Kratzer TB, Islami F, Dahut WL, Knudsen KE. Disparities and Trends in Genitourinary Cancer Incidence and Mortality in the USA. Eur Urol. 2023 Jul;84(1):117-126. doi: 10.1016/j.eururo.2022.11.023. Epub 2022 Dec 21. PMID: 36566154.
- Spratt DE, Liu VYT, Jia AY, Royce TJ, Sandler HM, Pugh SL, Tran PT, Feng FY. Meta-analysis of Individual Patient-level Data for a Multimodal Artificial Intelligence Biomarker in High-risk Prostate Cancer: Results from Six NRG/RTOG Phase 3 Randomized Trials. Eur Urol. 2024 Oct;86(4):369-371. doi: 10.1016/j.eururo.2024.06.019. Epub 2024 Jul 17. PMID: 39025748; PMCID: PMC11480946.
- Corley DA, Jensen CD, Marks AR, Zhao WK, Lee JK, Doubeni CA, Zauber AG, de Boer J, Fireman BH, Schottinger JE, Quinn VP, Ghai NR, Levin TR, Quesenberry CP. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014 Apr 3;370(14):1298-306. doi: 10.1056/NEJMoa1309086. PMID: 24693890; PMCID: PMC4036494.
- Irbaz Bin Riaz et al., Applications of Artificial Intelligence in Prostate Cancer Care: A Path to Enhanced Efficiency and Outcomes. Am Soc Clin Oncol EducBook 44, e438516(2024).DOI:10.1200/EDBK 438516