(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a presentation by Joan Carles Galceran, MD, PhD, discussing a subgroup analysis of ARASENS assessing age-related efficacy and safety of darolutamide + ADT and docetaxel in patients with metastatic hormone-sensitive prostate cancer (mHSPC). In ARASENS, darolutamide + ADT + docetaxel significantly reduced the risk of death by 32.5% (HR 0.68; 95% CI 0.57–0.80; p < 0.0001) versus placebo + ADT + docetaxel with similar incidence of treatment emergent adverse events between groups in patients with mHSPC.1 Given these results, darolutamide + ADT + docetaxel has become one of the standards of care in mHSPC. Importantly, older men have a higher incidence of prostate cancer, and 20% of cases are diagnosed in men aged >75 years. At GU ASCO 2025, Dr. Carles and colleagues reported post-hoc efficacy and safety data in patients by age subgroups (<75 years versus ≥75 years) in ARASENS.
Patients were randomized to receive darolutamide 600 mg orally twice daily or placebo, with ADT + docetaxel:

Age subgroups were analyzed for baseline characteristics including ongoing comorbidities, treatment duration, completion of docetaxel therapy, use of first subsequent therapy, key efficacy outcomes, and safety.
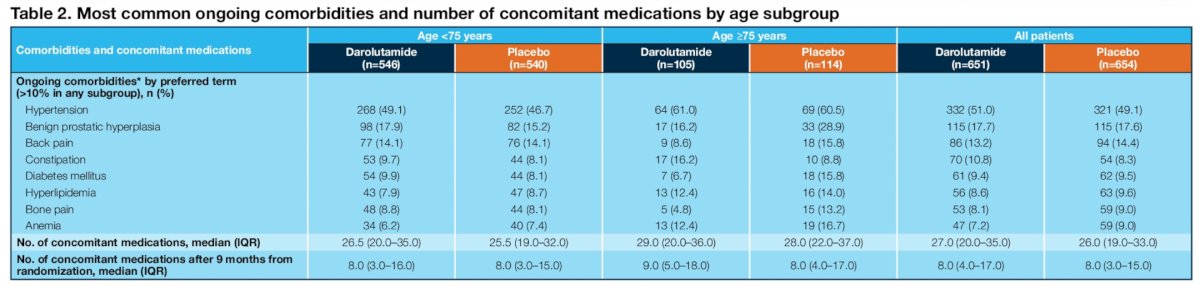
Of 1,305 patients analyzed in ARASENS, ages ranged from 41–89 years, with 1,086 patients <75 years (83%; darolutamide n = 546; placebo, n = 540) and 219 patients ≥75 years (17%; darolutamide n = 105; placebo n = 114). Baseline characteristics were generally similar in the darolutamide and placebo groups by age subgroup. The most common comorbidities by system organ class in patients <75 years and ≥75 years were vascular (55% versus 67%), musculoskeletal/connective tissue (42% versus 42%), and metabolism/nutrition (35% versus 43%) disorders:

The most common ongoing comorbid conditions (>10%) were generally more frequent in patients >= 75 years of age versus those <75 years. The median number of concomitant medications was higher for older patients overall, but, when the time period was limited to after 9 months from randomization (ie. after the period of docetaxel use when co-medications might have been required to manage associated toxicity), the number of concomitant medications was similar in the two age subgroups:
The overall survival benefit of darolutamide versus placebo was consistent across age subgroups (<75 years: HR 0.70, 95% CI 0.58–0.84; ≥75 years: HR 0.61, 95% CI 0.41–0.91):

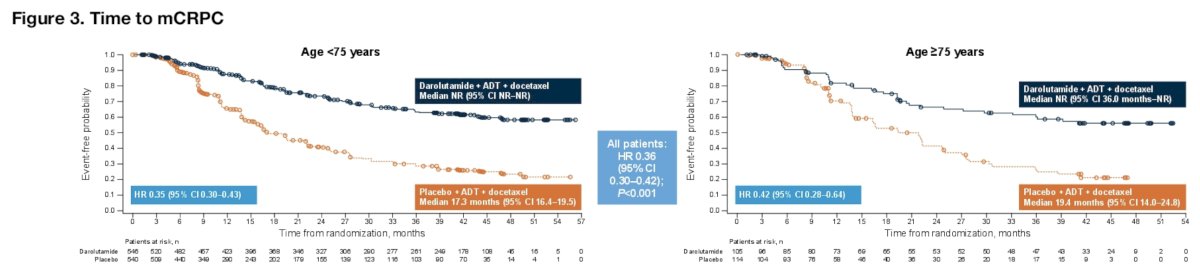
Time to metastatic castration-resistant prostate cancer (mCRPC) was also longer with darolutamide versus placebo across age subgroups (<75 years: HR 0.35, 95% CI 0.30–0.43; ≥75 years: HR 0.42, 95% CI 0.28–0.64):
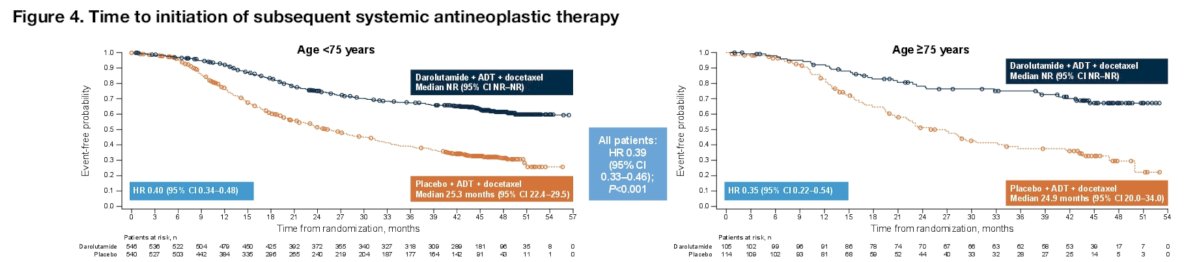
Time to initiation of subsequent antineoplastic therapy also favored the darolutamide + ADT + docetaxel arm across the age subgroups (<75 years: HR 0.40, 95% CI 0.34–0.48; ≥75 years: HR 0.35, 95% CI 0.22–0.54):
Among patients who entered follow-up, a higher percentage in the placebo group received subsequent life-prolonging systemic therapy compared with the darolutamide group in the overall population, and this was consistent in both age groups:
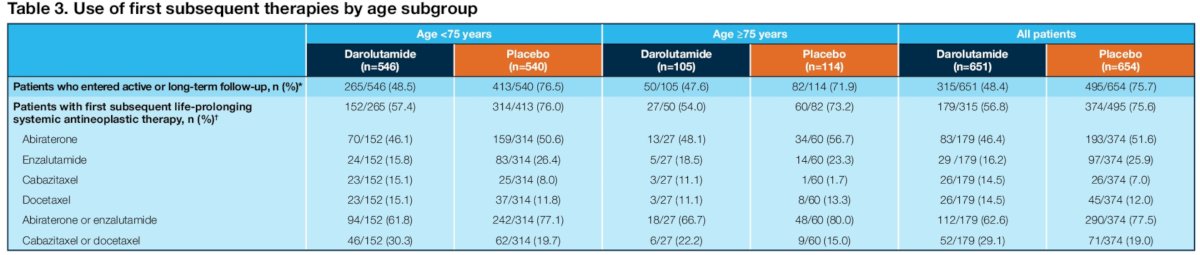
Abiraterone was the most frequently used subsequent therapy in both age groups, consistent with the overall population, and the use of chemotherapy as first subsequent therapy was less frequent in older versus younger patients. Treatment emergent adverse events were generally similar between darolutamide and placebo, with slightly higher incidence rates in older patients:
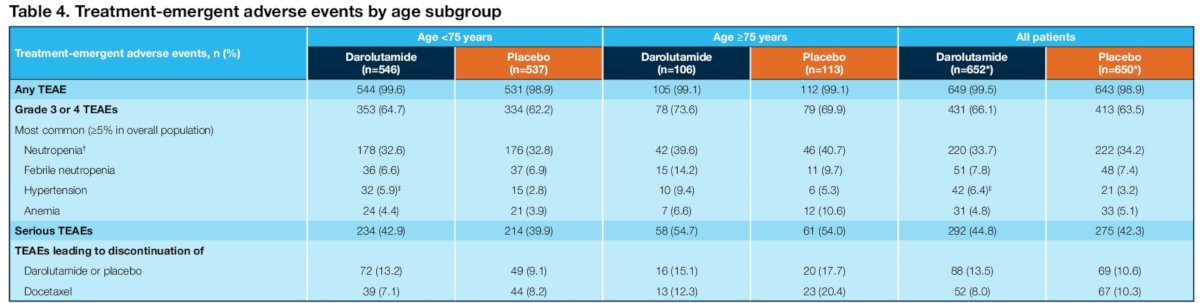
Few patients discontinued darolutamide or placebo due to treatment emergent adverse events in both age subgroups (<75 years: 13.2% versus 9.1%; ≥75 years: 15.1% versus 17.7%). The most common grade 3/4 treatment emergent adverse events were generally similar between darolutamide and placebo across age subgroups and occurred most frequently during overlapping docetaxel treatment. Treatment emergent adverse events commonly associated with androgen receptor pathway inhibitors occurred at similar incidences between treatment groups in both age subgroups:

Treatment duration was consistently longer with darolutamide versus placebo (<75 years: 41.2 versus 16.8 months; ≥75 years: 38.5 versus 15.0 months), and most patients completed 6 cycles of docetaxel (<75 years: 89% versus 88%; ≥75 years: 80% versus 76%).
Dr. Carles concluded his presentation by discussing a subgroup analysis of ARASENS assessing age-related efficacy and safety of darolutamide + ADT and docetaxel in patients with mHSPC with the following take-home points:
- Patients with mHSPC benefited from darolutamide + ADT + docetaxel irrespective of age (<75 years and ≥75 years), with consistent improvements in overall survival, time to mCRPC, and time to initiation of subsequent therapy compared with placebo + ADT + docetaxel, consistent with the overall population
- Darolutamide was well tolerated in both age subgroups, with most patients (>80%) able to receive the full six cycles of docetaxel and with similar incidence of treatment emergent adverse events compared with placebo, including treatment emergent adverse events commonly associated with androgen receptor inhibitors
- The results support the use of darolutamide in combination with ADT and docetaxel in all patients with mHSPC, regardless of age
Presented by: Joan Carles Galceran, MD, PhD, Vall d’Hebron Institute of Oncology, Hospital Universitari Vall d’Hebron, Barcelona, Spain
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References: