(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Johann De Bono discussing the association of baseline and on-treatment ctDNA fraction with clinical outcomes in patients with mCRPC in the PSMAfore study of 177Lu-PSMA-617. In PSMAfore,1177Lu-PSMA-617 prolonged radiographic progression free survival versus androgen receptor pathway inhibitor change in taxane-naive adults with PSMA-positive mCRPC progressing once on an androgen receptor pathway inhibitor. Moreover, previously presented at ASCO 2024, baseline circulating tumor DNA (ctDNA) fraction was associated with radiographic progression free survival at the second interim analysis of overall survival. At GU ASCO 2025, Dr. De Bono and colleagues assessed the association of baseline and cycle 2 day 1 ctDNA fraction, and early ctDNA and PSA dynamics, with radiographic progression free survival and overall survival at the third interim analysis of overall survival.
Patients were randomized 1:1 to 177Lu-PSMA-617 (7.4 GBq Q6W; x 6 cycles) or androgen receptor pathway inhibitor change. Endpoints included radiographic progression free survival (primary) and overall survival (key secondary):

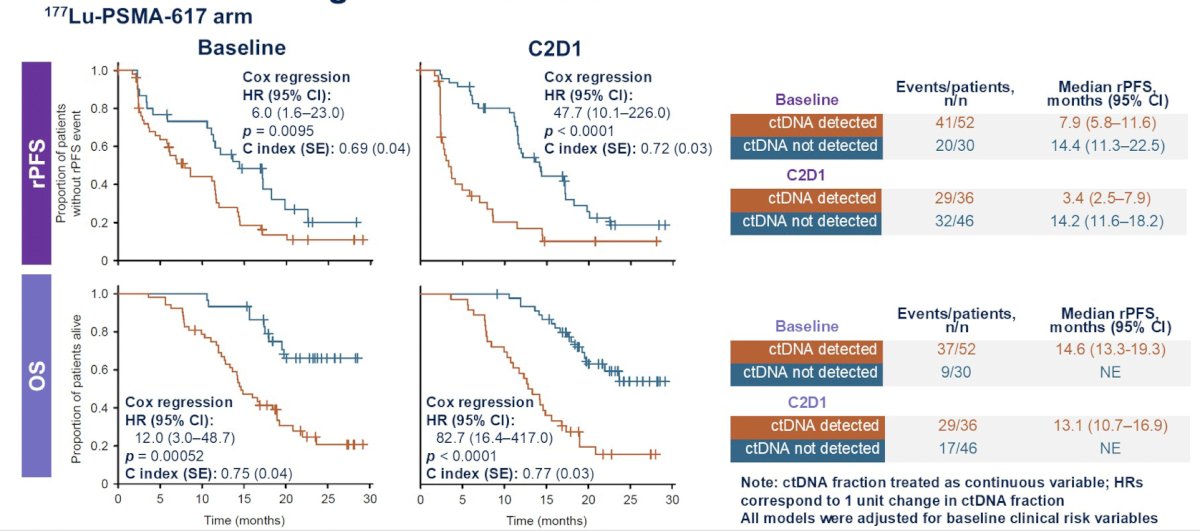
Plasma ctDNA fraction was analyzed at baseline and at cycle 2 day 1 using an in-house custom panel. Cox regression (adjusted for 3 risk classes based on clustering of 17 baseline clinical features) and random forest (adjusted for 15 baseline clinical features) modeling were used to assess the association of ctDNA fraction and PSA with clinical outcomes at the February 27, 2024 data cutoff.
Patients with plasma samples at baseline and cycle 2 day 1 were included (177Lu-PSMA-617, 82/234; androgen receptor pathway inhibitor change, 91/234). Cox regression models adjusted for clinical features in the 177Lu-PSMA-617 arm showed that higher ctDNA fraction was associated with shorter radiographic progression free survival and overall survival. These associations were stronger for cycle 2 day 1 than baseline, both when comparing individual models and within a model including both time points:
Lower baseline and cycle 2 day 1 ctDNA fraction was associated with higher frequency of RECIST response:

Moreover, PSA50 response was associated with lower baseline and cycle 2 day 1 ctDNA fraction, with a stronger association for C2D1 ctDNA fraction:

In the overall population, ctDNA clearance from baseline to cycle 2 day 1 and PSA 50 response were associated with longer radiographic progression free survival:

A similar trend for overall survival was observed in the 177Lu-PSMA-617 arm, however the low number of events among PSA50 responders (12/43) precluded accurate calculation of median overall survival. In Cox regression models, fractional decrease in ctDNA provided additional information beyond PSA50 response.

Finally, ctDNA clearance at cycle 2 day 1 provided additional information to PSA50 in the radiographic progression free survival model in the overall population (patients with detectable ctDNA at baseline):

Dr. De Bono concluded his presentation by discussing the association of baseline and on-treatment ctDNA fraction with clinical outcomes in patients with mCRPC in the PSMAfore study of 177Lu-PSMA-617 with the following take-home points:
- Higher ctDNA fraction was associated with shorter radiographic progression free survival and overall survival in patients treated with 177Lu-PSMA-617. This association was stronger with cycle 2 day 1 than at baseline ctDNA fraction
- Higher ctDNA fraction was associated with worse tumor response
- ctDNA clearance from baseline to cycle 2 day 1 was associated with longer radiographic progression free survival and overall survival
- Early ctDNA fraction dynamics contributed additional information in models of radiographic progression free survival and overall survival beyond PSA
- Post-treatment changes in ctDNA fraction merit evaluation as an intermediate endpoint for clinical benefit. The FDA recently released guidance on the use of ctDNA as a biomarker for response in clinical trials
Presented by: Johann De Bono, MD, MSc, PhD, FRCP, FMedSci, The Institute of Cancer Research and the Royal Marsden NHS Foundation Trust, Sutton, Surrey, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References: