(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to prostate cancer poster session. Dr. Pedro Isaacsson Velho presented the results of the ExBAT trial/LACOG 0620 that evaluated extreme bipolar androgen therapy (BAT), using alternating darolutamide and testosterone cypionate, in metastatic castrate-resistant prostate cancer (mCRPC) patients.
Androgen receptor inhibition remains the mainstay treatment of advanced prostate cancer. However, therapeutic resistance to androgen receptor inhibition is almost universal. Prostate cancer cells can develop resistance to androgen ablation through an adaptive marked upregulation of androgen receptors over time in response to low-androgen conditions. This upregulation can make these cells vulnerable to supraphysiologic testosterone exposure. BAT has been proposed as an approach to overcome androgen receptor therapeutic resistance. Rapid cycling between polar extremes of supraphysiologic and near-castrate serum testosterone in asymptomatic men with mCRPC has been proven safe and effective.
Prostate cancer cells adapt to chronic low testosterone conditions by upregulating androgen receptor activity.1-4 Androgen receptor levels may increase by 30 to 90-fold in CRPC cell lines and clinical samples, compared to normal prostate cells.5 While this marked upregulation of the androgen receptor can cause castration resistance, it also creates a therapeutic vulnerability to treatment with supraphysiologic androgen. BAT is typically performed by administering testosterone cypionate at the US Food and Drug Administration (FDA)–approved dose of 400 mg intramuscularly once every 28 days, while maintaining continuous testosterone suppression via surgical castration or luteinizing hormone–releasing hormone (LHRH) agonists or antagonists.
In this study, Dr. Isaacsson Velho and colleagues hypothesized that BAT could significantly enhance the efficacy of subsequent androgen receptor pathway inhibitors (ARPIs), such as darolutamide, in patients who had progressed on prior abiraterone acetate therapy.
This was a single-arm, multicenter, phase II trial. The trial design is illustrated below: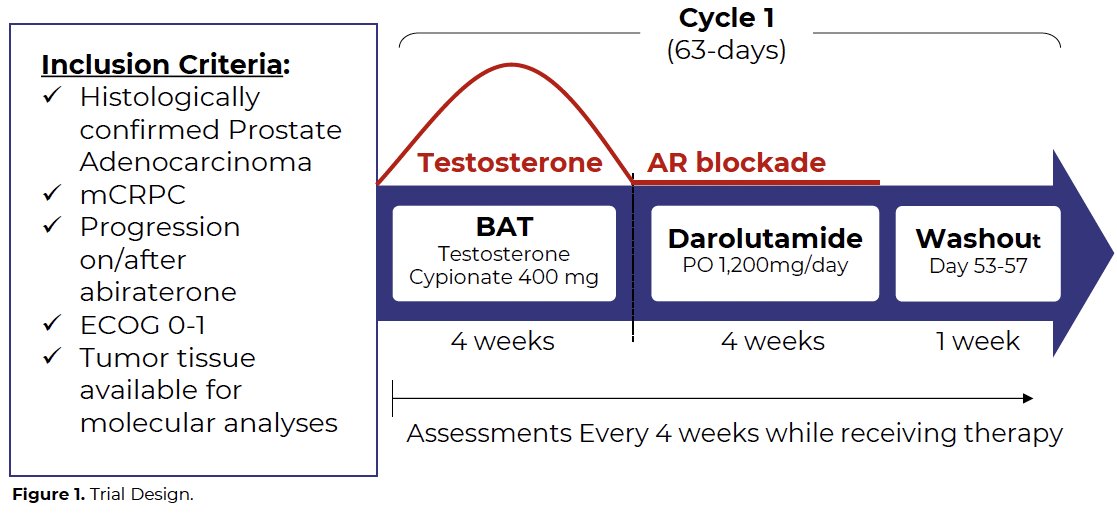
This trial included mCRPC patients who had disease progression on/after abiraterone acetate therapy and had tumor tissue available for molecular analyses. Prior docetaxel exposure in the hormone-sensitive state was allowed. Eligible patients received a pre-planned regimen of alternating BAT and darolutamide. Patients received intramuscular testosterone cypionate 400 mg on day 1, followed by oral darolutamide 1,200 mg/day from day 29 to day 56, followed by a washout period of 7 days, in 63-day cycles.
The primary endpoint was radiographic progression-free survival (rPFS) at 12 months. Secondary endpoints included:
- Median rPFS
- PSA50 response
- Overall survival
- Quality of life
- Safety
Between June 2021 and March 2023, 51 patients were enrolled across 9 centers, and 48 patients were eligible for efficacy analysis. Baseline characteristics are summarized in the table below. The mean age was 70 years. 78% of patients had received abiraterone in the castrate-resistant setting, with the remaining 22% in the castrate-sensitive setting.
The 12 months rPFS rate was 41% (95% CI: 26–55%), with a median rPFS of 9 months (95% CI: 4–13 months).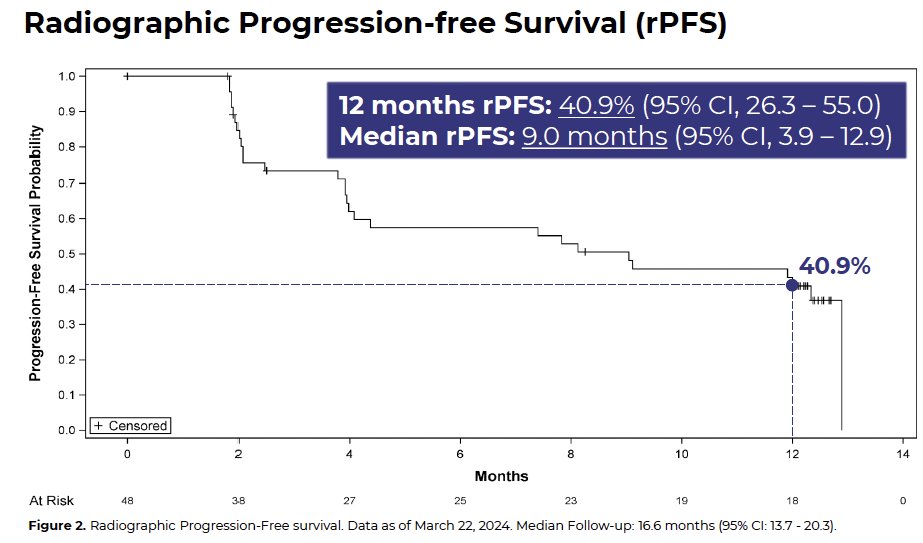
A PSA50 response was observed in 16.7% of patients (95% CI: 7.4–30.2%). The median overall survival was 23 months (95% CI: 17.7–not reached).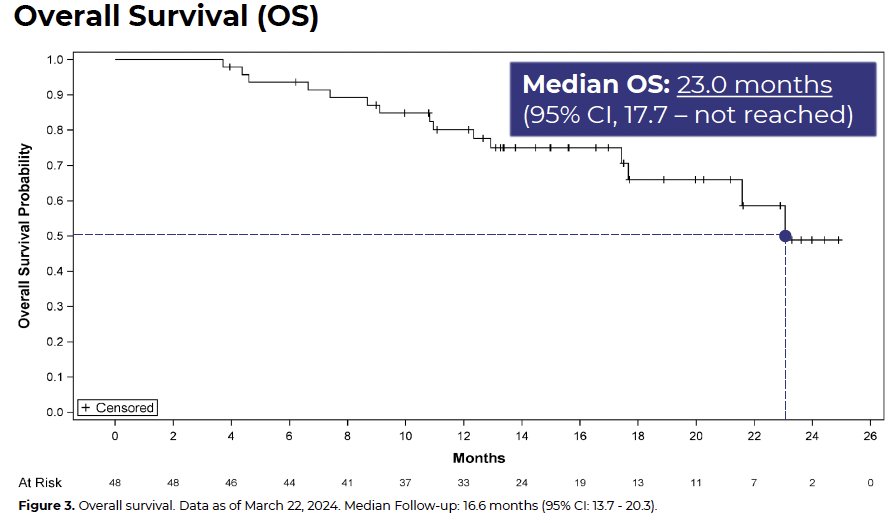
As of the study cut-off date of March 22, 2024, 10 patients remained on treatment. Quality-of-life, as assessed using the Functional Assessment of Cancer Therapy – Prostate (FACT-P) questionnaire, was maintained during treatment: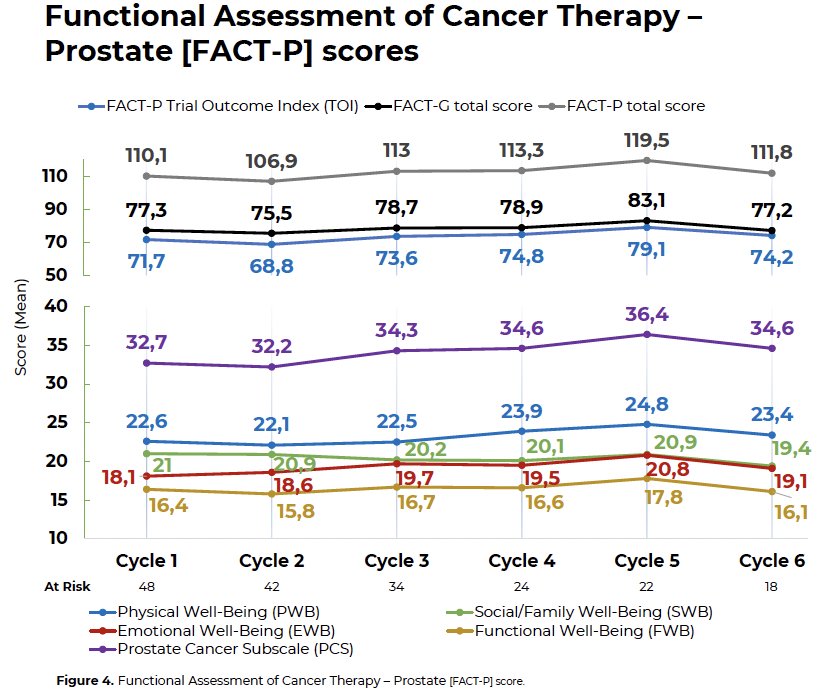
Treatment-related adverse events of any grade were observed in 65% of patients (Grade 3–4: 10%). No Grade 5 events were reported. The most common adverse events were bone and breast pain.
Dr. Isaacsson Velho concluded that the ExBAT study demonstrated durable (≥12 months) anti-tumor activity with alternating BAT and darolutamide in around 40% of abiraterone pre-treated mCRPC patients, with a manageable safety profile. Further studies evaluating ExBAT are needed to identify biomarkers of response and the impact of ARPI sequencing in subsequent lines of therapy.
Presented by: Pedro Isaacsson Velho, Hospital Moinhos de Vento (HMC), Porto Alegre, Brazil
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Linja MJ, Savinainen KJ, Saramaki OR, et al. Amplification and overexpression of AR gene in hormone-refractory PCa. Cancer Res. 2001;61:3550-3555.
- Attard G, Swennenhuis JF, Olmos D, et al. Characterization of ERG, AR, and PTEN gene status in circulating tumor cells from patients with castration-resistant PCa. Cancer Res. 2009;69:2912-2918.
- Brown RS, Edwards J, Dogan A, et al. Amplification of the AR gene in bone metastases from hormone-refractory PCa. J Pathol. 2002;198:237-244.
- Antonarakis ES, Lu C, Wang H, et al. AR-V7 and resistance to enzalutamide and abiraterone in PCa. N Engl J Med. 2014;371:1028-1038.
- Isaacs JT, D’Antonio JM, Chen S, et al. Adaptive auto-regulation of AR provides a paradigm shifting rationale for bipolar androgen therapy (BAT) for castrate resistant human PCa. Prostate. 2012;72:1491-1505.