(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to the Poster Session A: Prostate Cancer. Dr. Neeraj Agarwal presented Abstract 145: Cabozantinib ± atezolizumab in patients with metastatic castration-resistant prostate cancer (mCRPC): Expansion cohorts from the open-label phase 1b COSMIC-021 study.
Patients with metastatic castration-resistant prostate cancer (mCRPC) who progress on an androgen receptor pathway inhibitor (ARPI) have a poor prognosis, with a median overall survival (OS) of less than two years. Life expectancy is even shorter for those with liver metastases. Cabozantinib is a multi-tyrosine kinase inhibitor targeting VEGFR, MET, and TAM kinases, creating an immune-permissive tumor microenvironment, enhancing responses to immune checkpoint inhibitors (ICIs). Cabozantinib is approved in combination with the ICI nivolumab as first-line therapy for advanced renal cell carcinoma.1
The phase III CONTACT-02 trial evaluated cabozantinib + atezolizumab versus a second novel hormonal androgen receptor pathway inhibitor (ARPI) in patients with mCRPC and measurable extrapelvic soft tissue metastases (visceral or lymph nodes) after progression on a first ARPI. The combination significantly improved PFS and showed a trend toward OS benefit compared to a second ARPI. Moreover, an OS benefit of ~5 months was observed with cabozantinib + atezolizumab versus ARPI in patients with liver metastases (HR 0.68 [95% Cl 0.47-1.00]; median 12.2 vs 7.1 months).2
Dr. Agarwal presented outcomes from similar patients in the randomized mCRPC expansion cohorts of COSMIC-021. COSMIC-021 was a multicenter, open-label, phase 1b, dose-escalation/expansion study (NCT03170960) evaluating cabozantinib + atezolizumab in patients with advanced cancers.
For this expansion study, eligible patients were ≥18 years of age with confirmed mCRPC (adenocarcinoma histology without a small cell component) and measurable extrapelvic soft tissue metastasis per Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1; visceral or nodal) who progressed (radiographic soft tissue or prostate specific antigen [PSA]) following treatment with either enzalutamide or abiraterone, or both. Notably, prior taxane-based chemotherapy was allowed for hormone-sensitive but not for castration-resistant prostate cancer
Patients were randomized 1:1:1 to receive single-agent oral cabozantinib (60 mg once daily [QD]), single-agent intravenous (IV) atezolizumab (1200 mg every 3 weeks [Q3W]), or cabozantinib + atezolizumab (oral cabozantinib 40 mg QD plus IV atezolizumab 1200 mg Q3W)
The primary endpoint was investigator-assessed ORR per RECIST v1.1, with safety as a key secondary endpoint. Efficacy outcomes were also evaluated by a blinded independent radiology committee (BIRC), including overall response rate (ORR), duration of response (DOR), and PFS per BIRC according to RECIST V1.1, overall survival (OS), PSA response rate (defined as ≥50% reduction in PSA), and PSA progression rate (defined as an increase in PSA of 2 ng/mL and 25% from nadir confirmed by subsequent rising PSA ≥28 days later)
Additionally, flow cytometry and proteomic profiling were performed on baseline and on-treatment samples to explore potential biomarkers of response. This included assessing the impact of treatment on lymphoid and myeloid cells, CD8+ T cells, natural killer (NK) cells, protein angiogenic markers, and protein immune markers.
A total of 111 patients were randomized to receive either cabozantinib (n=51), single agent atezolizumab (n=10), or cabozantinib + atezolizumab (n=50). Notably, the single agent atezolizumab cohort did not meet the prespecified ORR threshold of at least one response to move beyond enrollment. The median age was 70 years in both groups. Notably, bone metastases were present in 75% and 72% of patients, respectively, while liver metastases were reported in 20% and 24%. Additionally, prior docetaxel treatment for mCSPC was received by 31% of patients in the cabozantinib group and 24% in the combination group. Baseline characteristics are shown below:

The ORR by BIRC and investigator assessment was 20% for cabozantinib (95% CI, 10–33) and 22% for cabozantinib + atezolizumab (95% CI, 12–36), with similar response rates observed between groups. Additionally, more patients in the combination group achieved a PSA response with a longer duration of response (NE vs. 6.93 and a prolonged time to PSA progression (5.6 vs. 3.5 months).
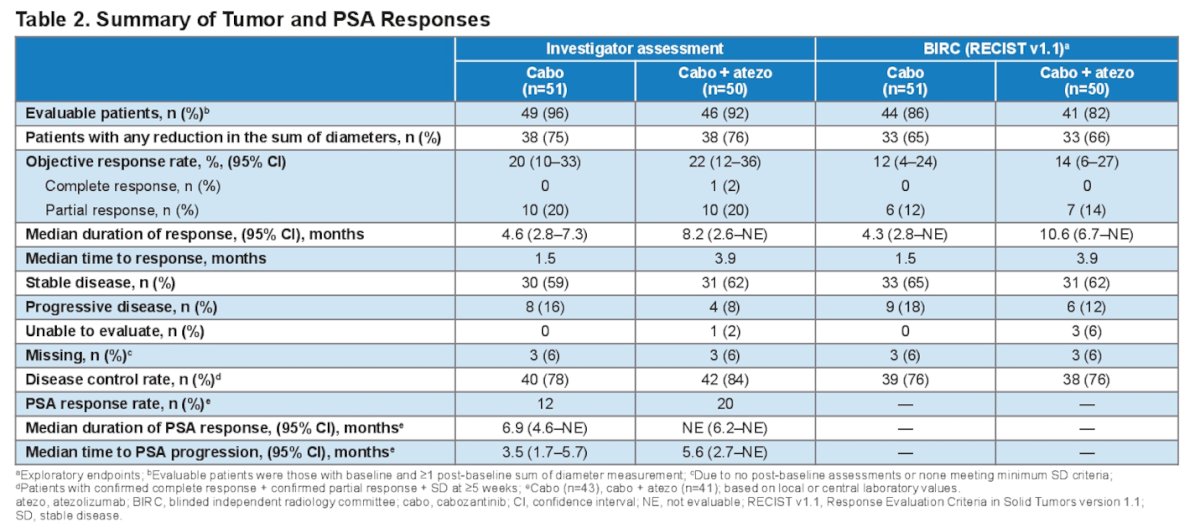
While progression-free survival (PFS) by BIRC was comparable between treatments (HR, 0.96; 95% CI, 0.59–1.58), the Kaplan-Meier estimate of patients without progression at 12 months was higher with cabozantinib + atezolizumab (26% vs 14%).

Compared with cabozantinib alone, the cabozantinib + atezolizumab group had approximately twice the duration of response, fewer patients with progressive disease as their best response, and a numerically longer median overall survival (HR, 0.91; 95% CI, 0.57–1.46).

In the liver metastases subgroup analysis, median PFS and OS were longer with cabozantinib + atezolizumab compared to cabozantinib alone (PFS: 5.7 vs. 2.5 months; OS: 14.7 vs. 5.0 months), with a statistically significant OS benefit (HR, 0.25; 95% CI, 0.08–0.77).

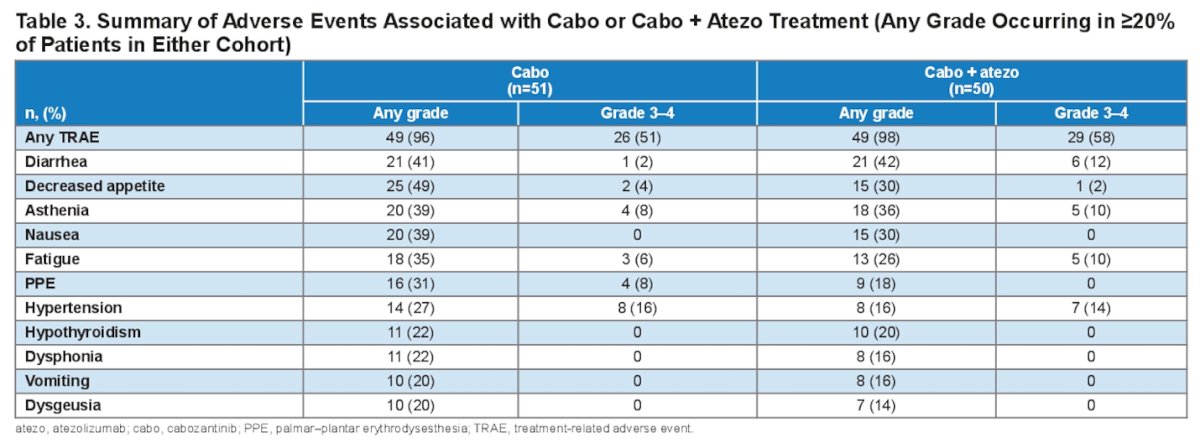
The median duration of treatment was 4.8 months in the cabozantinib cohort and 5.7 months in the combination cohort. The most common grade 3-4 treatment-related adverse events (AEs) in the cabozantinib group were hypertension (16%), asthenia (8%), and palmar-plantar erythrodysesthesia (8%). In the combination cohort, the most frequent grade 3-4 AEs were hypertension (14%), diarrhea (12%), asthenia (10%), and fatigue (10%). Notably, treatment-related AEs led to treatment discontinuation in 12% of patients receiving cabozantinib and 22% of those receiving cabozantinib + atezolizumab.
Programmed cell death-ligand 1 (PD-L1) expression by immunohistochemistry was available for 54 patients, while tumor mutational burden (TMB) determined by whole-exome sequencing was available for 17. No association was observed between PD-L1 combined positive score or TMB and clinical activity in any cohort.
Notably, in both cohorts, treatment was associated with a reduced number of plasma monocytes, neutrophils, and myeloid-derived suppressor cells, and an increased number of total CD8+ and NK cells as shown in the figure below.

Moreover, flow cytometry of CD8+ T cell subsets showed a significantly greater increase in activated CD8+ T cells (CD38+ and CD38+/HLA-DR+) with the combination compared with cabozantinib alone. Similarly, the combination was associated with a significantly higher increase in HLA-DR+ andCD38+/HLA-DR+ NK cells than cabozantinib treatment alone as illustrated below.

The investigators also analyzed pharmacodynamic protein biomarkers associated with the angiogenic pathway (VEGFR2/A, Angiopoietin-2, Tie2) and immune response. Differential regulation of these biomarkers was observed, as outlined below.
Dr. Agarwal concluded the presentation with the following key messages:
- Cabozantinib and cabozantinib + atezolizumab demonstrated clinical activity in patients with mCRPC and extrapelvic soft tissue metastases, with no new safety signals in the expansion cohorts of COSMIC-021.
- Notably, the combination showed additive clinical benefits in patients with liver metastases, with a significantly longer PFS and OS.
- Exploratory data from these randomized cohorts suggest an additive effect of atezolizumab to cabozantinib, with a prolonged duration of response (Double) in the combination group.
- Prolonged median PFS (5.7 vs 2.5 months) and OS (14.7 vs 5.0 months) with the combination vs. cabozantinib alone were observed in the subgroup of patients with liver metastases, indicating a clinically meaningful contribution of atezolizumab compared with single-agent cabozantinib in this subgroup with poor prognosis.
- Analysis of immune cell populations and protein biomarkers suggests that combination treatment promotes an immune-permissive tumor microenvironment.
Presented by: Neeraj Agarwal, MD, Medical Oncologist, Professor of medicine, and a Presidential Endowed Chair of Cancer Research at the Huntsman Cancer Institute (HCI), University of Utah, United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- CABOMETYX (cabozantinib) highlights of prescribing information. 2023.https://www.cabometyxhcp.com/sites/default/files/2021-03/prescribing-information.pdf (accessed Jan 20, 2025).
- Agarwal N, Azad A, Carles J, Chowdhury S, McGregor B, Merseburger AS, Oudard S, Saad F, Soares A, Benzaghou F, Kerloeguen Y, Kimura A, Mohamed N, Panneerselvam A, Wang F, Pal S. A phase III, randomized, open-label study (CONTACT-02) of cabozantinib plus atezolizumab versus second novel hormone therapy in patients with metastatic castration-resistant prostate cancer. Future Oncol. 2022 Mar;18(10):1185-1198. doi: 10.2217/fon-2021-1096. Epub 2022 Jan 17. PMID: 35034502.