(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA was host to a prostate cancer poster session. Dr. Neeraj Agarwal presented a sub-analysis of IMPLEMENT aimed at evaluating the barriers to and facilitators of first-line treatment intensification in metastatic castration-sensitive prostate cancer (mCSPC), by practice setting and intensification frequency.
First-line treatment intensification (i.e., androgen-deprivation therapy [ADT] + chemotherapy, androgen receptor pathway inhibitors [ARPIs], or both; also known as combination therapy) is a recommended treatment option in clinical guidelines for mCSPC patients,1,2 but remains underutilized. Currently, <50% of patients with mCSPC receive first-line treatment intensification.3
IMPLEMENT is a mixed-methods study that used a qualitative implementation science approach to identify barriers to and facilitators of mCSPC treatment intensification in phase 1 and identified priority issues and helpful resources using a discrete choice experiment (DCE) in phase 2.
The study objectives were as follows:
- Phase 1: To identify differences in the barriers to and facilitators of first-line treatment intensification for mCSPC among US-based physicians in academic and non-academic settings, as well as high and low intensifiers (physicians who use first-line treatment intensification in >50% vs ≤50% of patients, respectively).
- Phase 2: To validate, quantify, and prioritize these barriers and facilitators and identify potential resources that may increase treatment intensification across these subgroups
Phase 1 (qualitative implementation science study) results:
- Key barriers: knowledge gaps, costs, and anticipated regret over using up treatment options early
- Key facilitators: knowledge of clinical trial data, intensification habits, interdisciplinary collaboration, and clinical staff support
Phase 2 (DCE) results:
- Most helpful for physicians: decision support tools, clinical trial summaries, and databases of post-treatment options
- Less helpful for physicians: tools to reduce administrative burden and information comparing clinical outcomes of first-line versus later treatment intensification5
This sub-analysis explores potential differences by practice setting and intensification status.
The IMPLEMENT study design is summarized below:

The statistical methods for Phases 1 and 2 are as below:
- Phase 1
- Statistical analysis: frequency differences of ≥20% between academic and non-academic settings and between self-reported low and high intensifiers considered notable, in accordance with the upper bound of a 90% confidence interval for the subgroup size
- Phase 2
- Statistical analysis: mixed-effects logistic regression model adjusted for physician specialty used to calculate a coefficient of helpfulness for each resource and identify resources with the strongest impact on treatment intensification decisions
- Coefficients constrained to have a minimum value of 0 and average of 1 for each respondent (i.e., values > 1 indicate above-average utility; values <1 indicate below-average utility)
- Differences by setting and intensification status analyzed using bootstrapping of respondents' choices for each subgroup
- Statistical analysis: mixed-effects logistic regression model adjusted for physician specialty used to calculate a coefficient of helpfulness for each resource and identify resources with the strongest impact on treatment intensification decisions

In phase 1, there were notable differences in barriers and facilitators by setting (academic versus non-academic), summarized below:
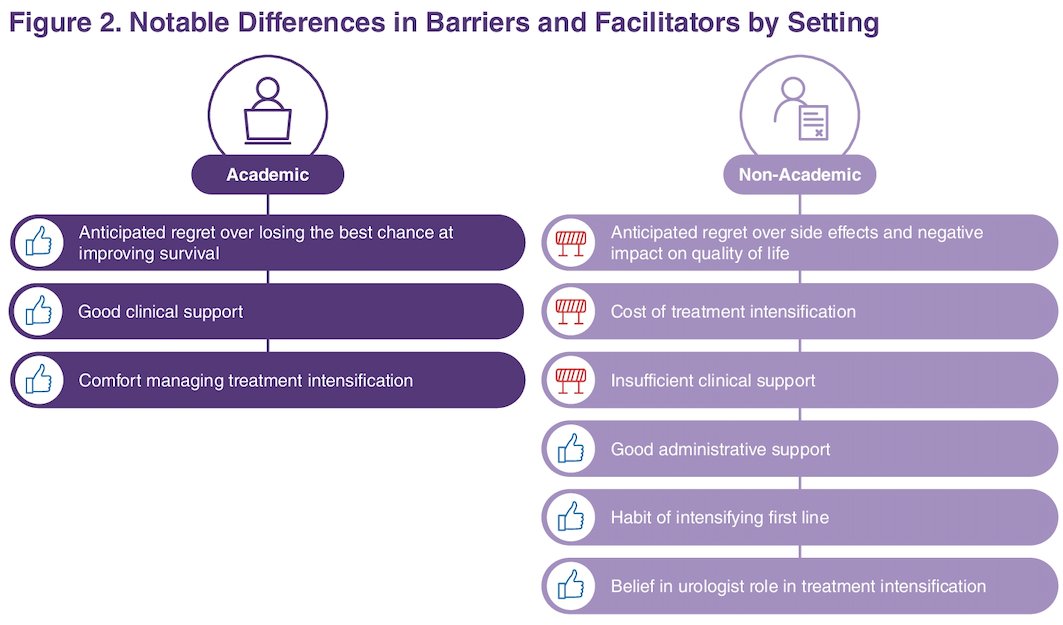
Both academic and non-academic physicians reported the following barriers and facilitators to treatment intensification:
Barriers:
- Knowledge gaps
- Tendency to intensify second line and reserve first-line treatment intensification for severe disease
- Urologists hanging onto their patients for too long
- Prioritizing preserving quality of life
- Anticipated regret over losing treatment options for later settings
- Patients' desire not to intensify
- A habit of starting patients on ADT or first-generation antiandrogens
- A low-intensifier peer environment
Facilitators:
- Confidence managing treatment intensification
- Good collaboration between urologists and oncologists
- Referring patients when unable to intensify
- A tendency not to limit intensification based solely on age and performance status
- Clinical pathways
Notable differences between high versus low intensifiers are illustrated below:
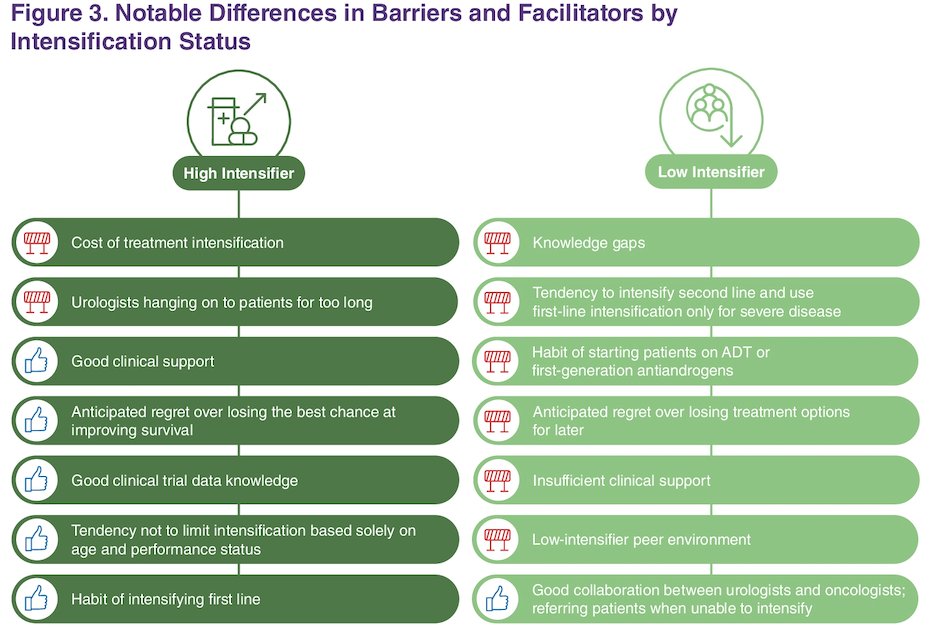
Both high and low intensifiers reported:
Barriers:
- Anticipated regret over side effects and negative impact on quality of life
- Patients' desire not to intensify
- Comfort and confidence in managing treatment intensification
- Good administrative support
- Clinical pathways
- A belief in the urologist's role in treatment intensification
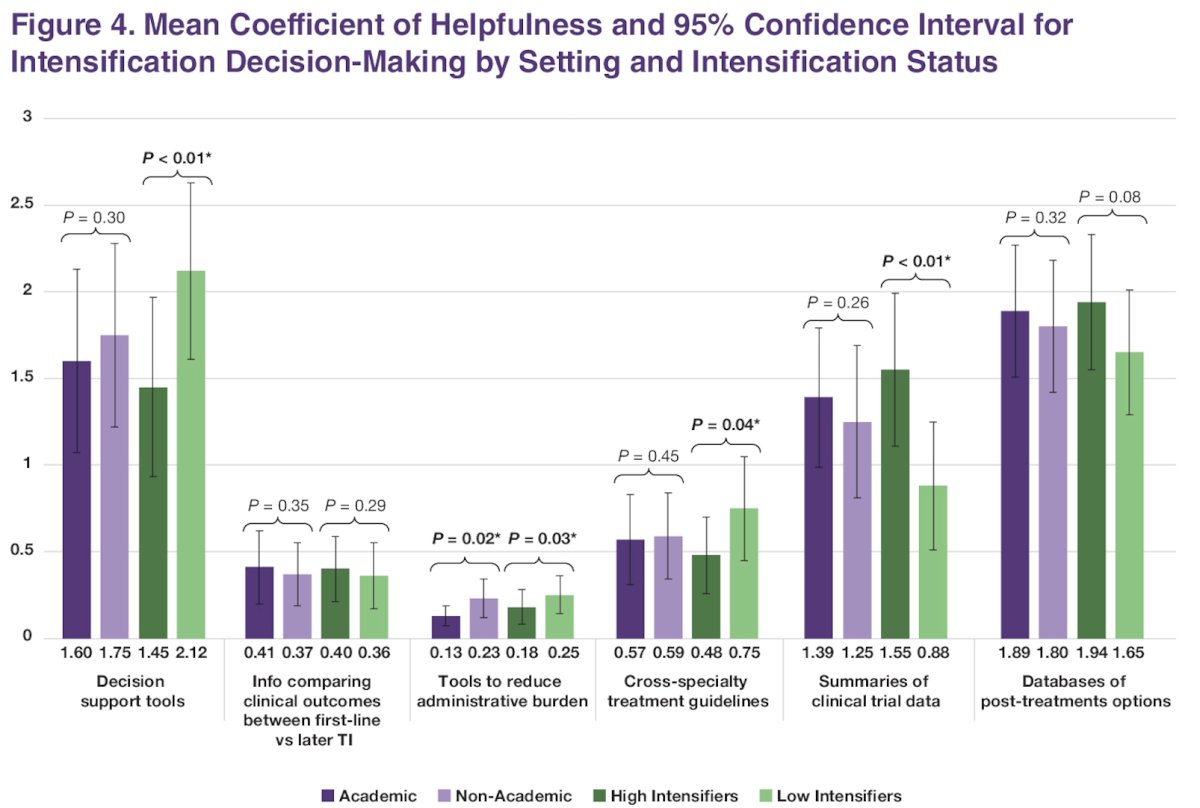
In phase 2, no significant differences were identified in the priority themes and the resources considered helpful by non-academic and academic healthcare providers. Decision support tools, clinical trial summaries, and databases of post-treatment options were considered helpful in both practice settings
With regards to high versus low intensifiers, clinical trial data summaries were considered very helpful by high intensifiers, whereas low intensifiers found them less helpful. Decision support tools and databases of post-treatment options were considered helpful by both high and low intensifiers. Decision support tools were considered significantly more helpful by low intensifiers. Information comparing clinical outcomes, tools to reduce administrative burden, and cross-specialty guidelines were considered less helpful for all subgroups.
Dr. Agarwal concludes as follows:
- Low intensifiers and non-academic physicians reported barriers to treatment intensification more frequently
- Low intensifiers had gaps in clinical trial knowledge, tended to reserve intensification for later, and had low-intensifier peers
- Non-academic physicians had concerns about side effects, cost, and impact on quality of life
- High intensifiers and academic physicians reported facilitators more frequently, such as good clinical support and anticipated regret about missing the best chance at improving survival
- Across all subgroups. decision support tools and databases of post-treatment options may help address barriers to treatment intensification and improve guideline-concordant care
Presented by: Neeraj Agarwal, MD, Professor, Department of Medicine, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Mottet N, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer. Eur Urol. 2021;79(2):243-62.
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Prostate Cancer. Version 1.2025. NCCN; 2025.
- Swami U, Agarwal N, Gupta S, et al. Phase I study of novel therapy in advanced prostate cancer. J Clin Oncol. 2022;40(6 Suppl):183.
- Loeb S, et al. J Clin Oncol. 2024;42(4 Suppl).
- Loeb S, et al. J Clin Oncol. 2024;42(16 Suppl).