(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Poster Session A: Prostate Cancer. Dr. Weinfeld presented Abstract 54, discussing real-world comparison of cost and adherence between patients receiving low-dose versus standard-dose abiraterone acetate (AA) in a safety-net hospital.
Dr. Weinfeld opened his presentation by noting that while the standard dose of Abiraterone (1,000 mg) is taken on an empty stomach, a lower dose (250 mg with a low-fat meal) is also a recognized option, with both approaches listed as standard of care in national guidelines for prostate cancer (PCa). The investigators aimed to evaluate in this real-world comparison, the cost and adherence of low-dose Abiraterone (LDAA) versus standard-dose Abiraterone (SDAA) in a diverse population treated at the University of Illinois Chicago (UIC), a public safety-net hospital.
Patients with PCa treated at the University of Illinois Chicago who filled at least one prescription for Abiraterone between April 2017 and September 2024 were retrospectively identified and included in this analysis. The study had two primary objectives and two secondary objectives:
- Primary objective #1: determine cost for patients receiving low-dose Abiraterone compared to those receiving standard-dose Abiraterone at UIH
- Primary objective #2: determine adherence for patients receiving low-dose Abiraterone compared to those receiving standard-dose Abiraterone at UH
- Secondary objective #1: determine progression-free survival (PFS) for patients receiving low-dose Abiraterone compared to those receiving standara-dose Abiraterone
- Secondary objective #2: determine rates of adverse drug events for patients receiving low-dose Abiraterone compared to those receiving standard-dose Abiraterone
Key variables of interest included age, race, ethnicity, insurance status, disease stage, monthly copays, medication fill history, dates of disease progression or death, and adverse events. The investigators used Chi-square analysis to compare cost, adherence, progression-free survival (PFS), and adverse events between the two groups.
Notably, adherence was calculated as the number of 30-day fills divided by the total number of months the patient was prescribed Abiraterone. Furthermore, Cost was assessed by monthly copays of 100 dollars or greater at any point during treatment.
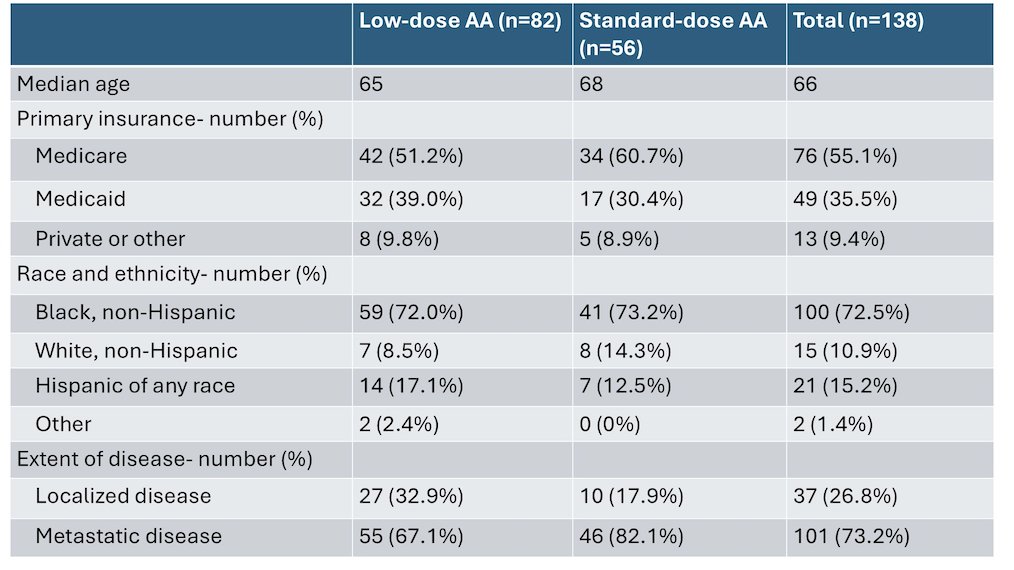
A total of 138 patients who filled a prescription for Abiraterone were identified during the study period. Of these, 72.5% were Black, 55.1% had Medicare as their primary insurance, and 35.5% had Medicaid. At the time of Abiraterone initiation, 26.8% had localized disease, while 73.2% had metastatic disease. Summarized baseline characteristics are shown below.
Patients receiving LDAA were less likely to have a monthly copay of $100 or more at any time point compared to those receiving SDAA (7.3% vs. 19.6%, p=0.04).

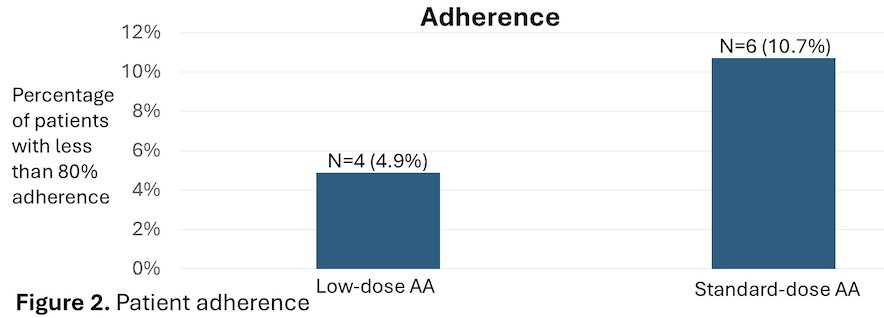
Adherence, defined as having less than 80% of expected fills, was lower in the SDAA group (10.7%) than in the LDAA group (4.9%), though this difference was not significant (p=0.20).
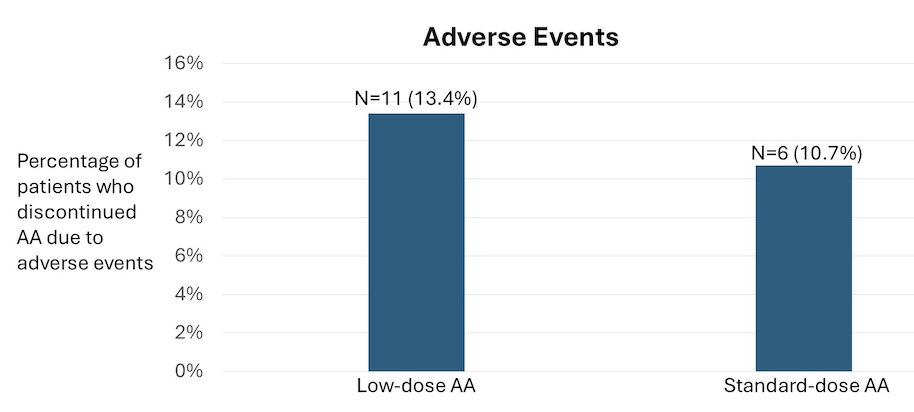
Adverse events were comparable between cohorts, with 13.4% of LDAA patients and 10.7% of SDAA patients discontinuing treatment due to toxicity (p=0.64).
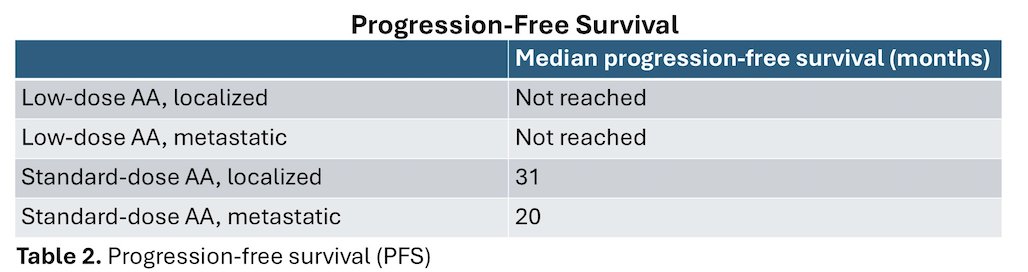
In terms of survival, the median PFS was 20 months in the SDAA group with metastatic disease, 31 months in the SDAA group with metastatic disease, but was not reached in the LDAA group due to data immaturity.
Dr. Weinfeld concluded his presentation with the following remarks:
- This retrospective analysis found that for a very diverse population of patients at a public safety-net hospital in Chicago. Patients receiving LDAA experienced a lower financial burden than those receiving SDAA, as reflected in the proportion of patients with copays of $100 or more.
- There was no statistically significant difference between the groups in adherence or the rate of adverse events leading to treatment discontinuation.
- Data on the impact of dose on oncological outcomes remains immature at this time, and results will be further discussed as more data becomes available
- Multicenter studies are needed to further compare cost savings, adherence/pill burden, and adverse events for the two dosing strategies reported.
Presented by: Michael Weinfeld, PhD, Professor in the Department of Oncology in the Faculty of Medicine & Dentistry of the University of Alberta, Edmonton, AB.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.