(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA, between February 13–15, 2025, was host to a prostate cancer poster session. Dr. Tobechukwu Okobi presented longer term follow-up results of a mature phase 1 trial of 225Ac-J591, an alpha emitter, in combination with 177Lu-PSMA-I&T, a beta emitter, in metastatic castration-resistant prostate cancer (mCRPC).
PSMA may be targeted by monoclonal antibodies or small molecules, which have different kinetics and biodistribution profiles and, therefore, different predicted toxicities. Differences between monoclonal antibodies and small-molecule ligands are summarized in the table below:
What is the difference between alpha and beta emitters? Alpha emitters are associated with higher linear energy transfers over a shorter range, compared to beta emitters, offering distinct therapeutic advantages with pre-clinical and dosimetric rationale for combining these two classes of emitters. Small molecules are not retained intracellularly, and the combination of an antibody with small-molecule ligands may enhance intracellular retention, as suggested by preclinical models.


This was a phase I trial of mCRPC patients with disease progression following ≥1 prior androgen receptor pathway inhibitor and chemotherapeutic agent (or unfit/refused) and ≥1 PSMA PET/CT-positive lesion (68Ga-PSMA-11 PET SUVmax >liver).
Eligible patients received 177Lu-PSMA-I&T (6.8 GBq) and 225Ac-J591 (30, 35, or 40 KBq/kg), with a 2nd dose administered at 8 weeks, The primary study outcomes were:
- Dose-limiting toxicity (DLT)
- Recommended phase II dose (RP2D)
Preliminary efficacy outcomes were:
- Overall survival (OS)
- Progression-free survival (PFS)
- PSA response (PSA50)
- Circulating tumor cell (CTC) changes
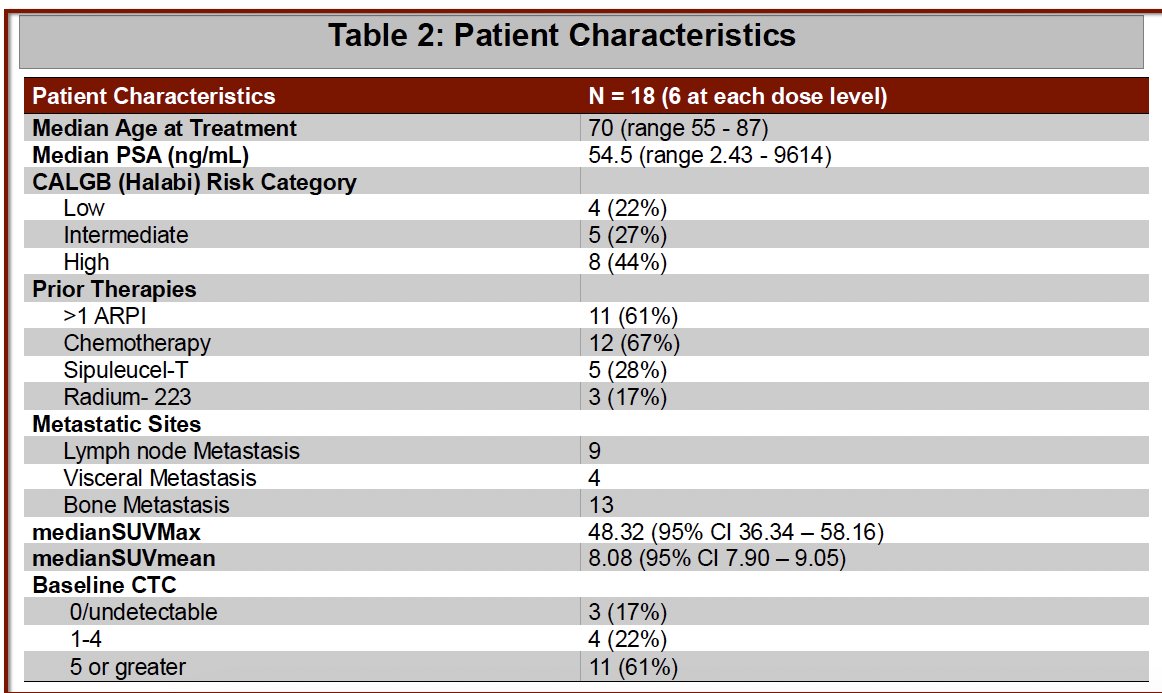
The baseline patient characteristics are summarized below (n=18). The median patient age was 70 years, with a median PSA level of 54.5 ng/mL. This was a heavily pre-treated population, with 61% having received ≥2 prior ARPIs, 67% chemotherapy, 28% sipuleucel-T, and 17% Ra-223. 13/8 patients had bone metastases, and 4/18 had visceral metastases.
With regards to the primary endpoint, two DLTs were observed at 40 Kbq/Kg (1 Grade 2 and 1 Grade 3 thrombocytopenia delaying cycle 2 for >3 weeks). The RP2D of 225Ac-J591 was 35 KBq/kg.

Overall, 94% of patients experienced a PSA declines (64% with >50% decline). Of those with available CTC counts (CellSearch) at baseline and follow up:
- 4/5 (80%) unfavorable-to-favorable
- 4/8 (50%) detectable-to-undetectable.
With extended follow up, the median OS to date is 29.8 months (95% CI: 7.4 – not reached). Currently, 6 patients are confirmed alive at 28 months median follow-up. With regards to progression-free survival, at the RP2D, 3 of 6 were progression-free at 13, 17 and 18 months. 1 of 6 treated at dose level 30 KBq/kg remains progression-free at 33 months follow up. The median PFS was 7.3 months.

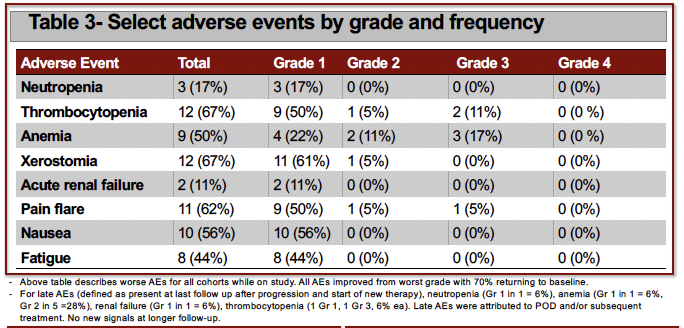
Select adverse events by grade and frequency are summarized below. The most common Grade 3 adverse events were thrombocytopenia, & anemia (17% for each). There were no grade 4 events reported.
Dr. Okobi concluded that the combination of a PSMA-targeted alpha emitter (via a monoclonal antibody) plus beta emitter (via small-molecule ligand) was feasible. High-grade adverse events were rare, and no new safety signals emerged with longer term follow-up. Nearly all patients had
PSA decline, and 6 had durable disease control off therapy.
Presented by: Tobechukwu Joseph Okobi, MD, MSc, Clinical Fellow, New York Presbyterian Brooklyn Methodist, Brooklyn, NY
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.