(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to the Poster Session A: Prostate Cancer. Dr. Cheng presented Abstract 77: Real world comparison of time-to-next-treatment (TTNT), time-to-castration-resistance (TTCR), and overall survival (OS) among patients with BRCA1/2 positive and homologous recombination repair (HRR) negative metastatic castration-sensitive prostate cancer (mCSPC).
Advanced metastatic disease prostate cancer is linked to poor outcomes, including a 5-year survival rate of 36.6%. Dr. Cheng highlighted that patients with metastatic hormone-sensitive prostate cancer (mHSPC) harboring genetic alterations in homologous recombination repair (HRR) genes, particularly BRCA1/2, may experience a more aggressive disease course and worse clinical outcomes. Targeted therapy, including poly ADP-ribose polymerase (PARP) inhibitors, is currently under investigation for treatment of patients with mHSPC harboring HRR mutations.1,2 However, there is limited real-world data on clinical outcomes among patients with mCSPC harboring BRCA+ mutations.1,2
This study aimed to compare time-to-next-treatment (TTNT), time-to-castration resistance (TTCR), and overall survival (OS) among patients with BRCA1/2-positive and HRR-negative mHSPC.
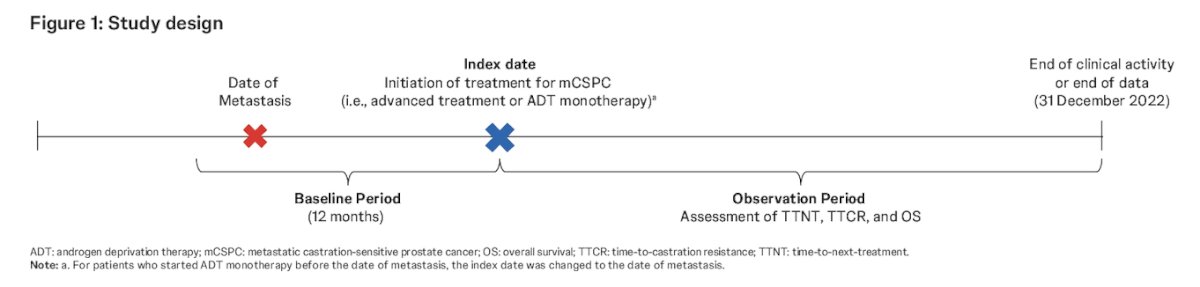
The investigators utilized data from oncology centers included in the US-based Flatiron Health-Foundation Medicine, Inc. Metastatic Prostate Cancer Clinico-Genomic Database (CGDB), covering the period from January 1, 2017, to December 31, 2022. Patients with mHSPC who underwent homologous recombination repair alteration testing and initiated first-line treatment for mHSPC after January 1, 2018 (index date), were included.
This was a retrospective longitudinal cohort study. Patients receiving their first treatment for mHSPC were included if they had results from ≥1 HRR mutation test and either:
- The start date of an advanced PC treatment (e.g., androgen receptor pathway inhibitors [ARPIs], chemotherapy) after the date of metastasis detection, with or without ADT, was on or after 1 January 2018 (index date)
- The start date of ADT monotherapy was on or after 1 January 2018, with the index date defined as the latter of ADT initiation or the date of metastasis detection
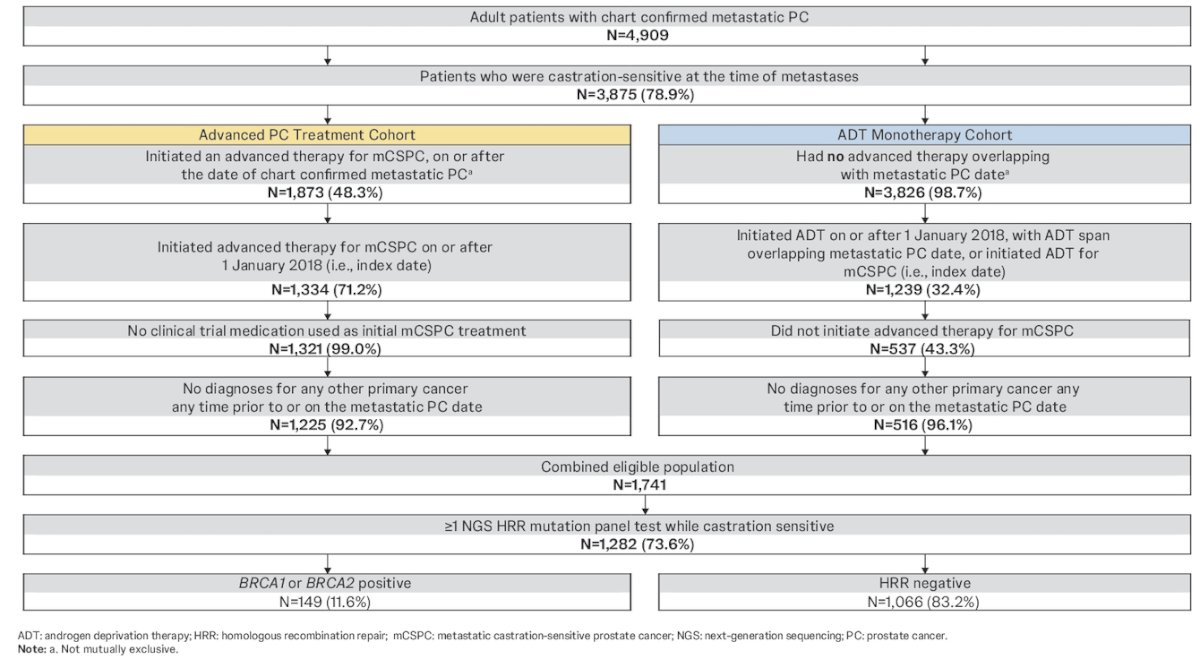
Patients were categorized as BRCA1/2-positive (BRCA1/2+) if they had at least one positive test for BRCA1/2 alterations, while those with no positive test for any of the eight assessed HRR alterations were classified as HRR-negative (HRR−). The following non-BRCA HRR mutations were also assessed: BRIP1, CHEK2, FANCA, PALB2, RAD51B, and RAD54L.
Patient inclusion and exclusion criteria as well as the sample selection process are summarized below:
The study evaluated time-to-next-treatment (TTNT), defined as the time from the index date to the start of subsequent treatment for prostate cancer, serving as an indicator of clinical and non-clinical performance. Additionally, time-to-castration resistance was measured as the time from the index date to prostate-specific antigen (PSA) increase on therapy or clinician documentation of castration resistance disease. Overall survival was assessed from the time of initial prostate cancer diagnosis to death.
The investigators used inverse probability of treatment weighting (IPTW) to balance baseline characteristics (12 months pre-index) between cohorts. Outcomes between BRCA1/2+ and HRR− patients were compared using weighted Kaplan-Meier curves. Hazard ratios 95% confidence intervals, and nominal p-values were generated using weighted Cox proportional hazards models.
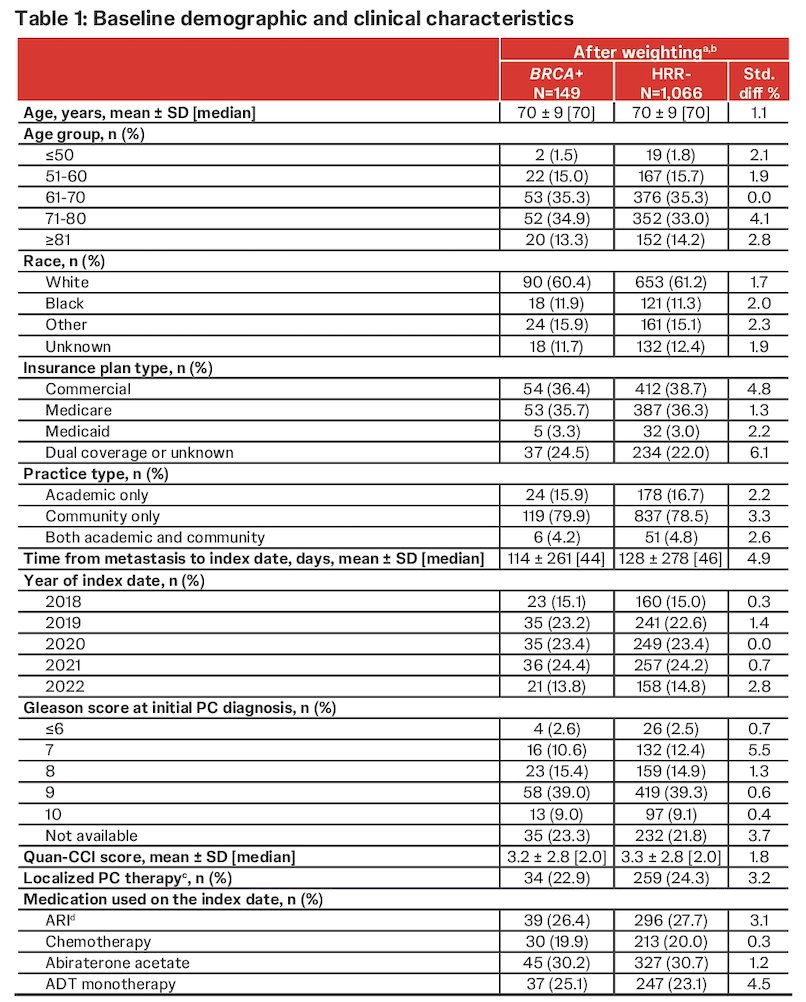
Dr. Cheng reported that a total of 149 BRCA1/2+ and 1,066 HRR− patients with mHSPC were included in this analysis. Weighted baseline characteristics were balanced as expected. Briefly, the median age was 70 years in both cohorts; 60.4% of BRCA1/2+ and 61.2% of HRR− patients were White. Abiraterone acetate was the most used first-line treatment (BRCA1/2+: 30.2%; HRR−: 30.7%). Baseline characteristics after weighting are summarized in the table below.
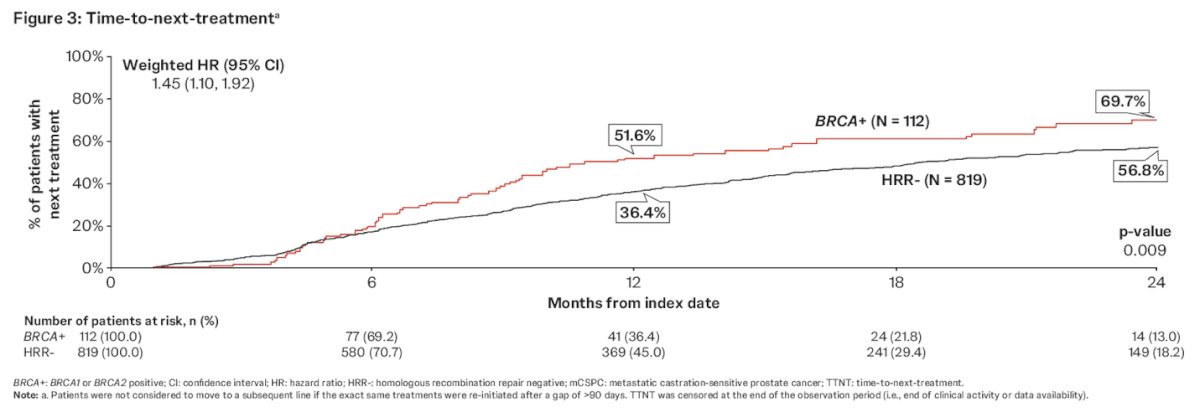
By 24 months after first-line treatment initiation, a significantly higher proportion of BRCA1/2+ patients progressed to next treatment than HRR− patients (59% vs. 46.7%; HR: 1.45 [95% CI: 1.10, 1.92], p=0.009). Median TTNT was shorter in the BRCA1/2+ cohort (10.9 months) than in the HRR− cohort (18.7 months).
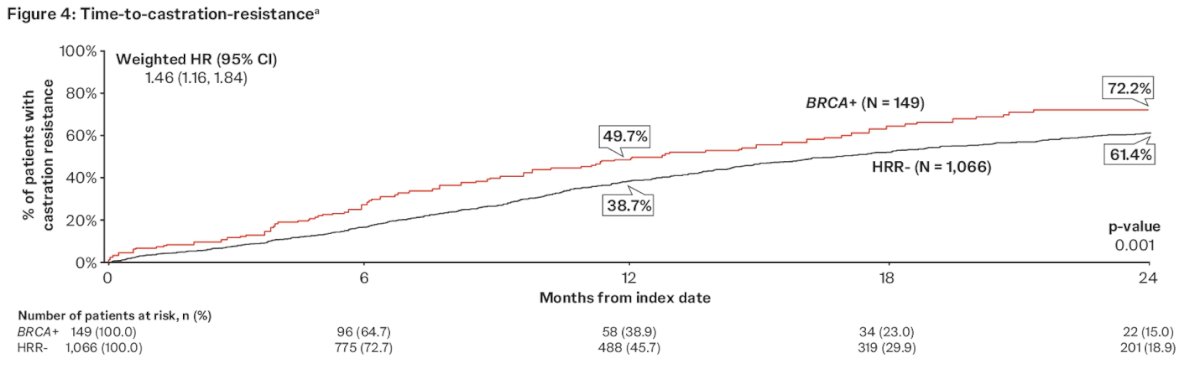
Moreover, at 24 months, a significantly higher proportion of BRCA1/2+ patients progressed to castration resistance than HRR− patients (66% vs. 53.3%; HR: 1.46 [95% CI: 1.16, 1.84], p=0.001). Median TTCR was shorter among BRCA1/2+ patients than HRR− patients (12.9 vs. 16.9 months).
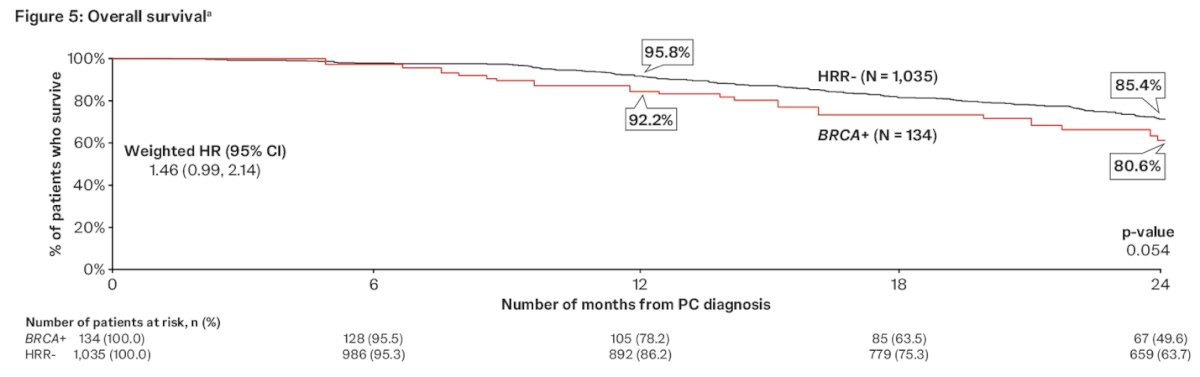
Fewer BRCA1/2+ patients survived 24 months after prostate cancer diagnosis (80.6%) compared to HRR− patients (85.4). This translated into a 46% higher risk of overall mortality in the BRCA1/2+ patients (HR: 1.46 [95% CI: 0.99, 2.14], p=0.054).
Dr. Cheng concluded her presentation with the following key messages:
- In this real-world study comparing BRCA+ and HRR- patients with mHSPC during the time of ARPI availability for the treatment of mHSPC, a significantly higher proportion of BRCA+ patients progressed to subsequent treatment and castration-resistance, relative to HRR-
- Overall survival data may signal more adverse survival outcomes for patients with BRCA+ and mHSPC.
- Given that BRCA1/2 alterations are the most prevalent HRR alterations observed in men with prostate cancer, these results support early identification of these alterations and a need for more effective tailored treatment for this specific population.
Presented by: Heather H. Cheng, MD, PhD, Medical Oncologist at Fred Hutchinson Cancer Center and Assistant Professor of Oncology at the University of Washington
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Dana E. Rathkopf et al., AMPLITUDE: A study of niraparib in combination with abiraterone acetate plus prednisone (AAP) versus AAP for the treatment of patients with deleterious germline or somatic homologous recombination repair (HRR) gene-altered metastatic castration-sensitive prostate cancer (mCSPC).. JCO 39, TPS176-TPS176(2021) DOI:10.1200/JCO.2021.39.6_suppl.TPS176
- Agarwal N, Saad F, Azad AA, Mateo J, Matsubara N, Shore ND, Chakrabarti J, Chen HC, Lanzalone S, Niyazov A, Fizazi K. TALAPRO-3 clinical trial protocol: phase III study of talazoparib plus enzalutamide in metastatic castration-sensitive prostate cancer. Future Oncol. 2024 Mar;20(9):493-505. doi: 10.2217/fon-2023-0526. Epub 2023 Oct 26. PMID: 37882449.