(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a renal cell, adrenal, penile, testicular, and urethral cancers poster session. Dr. David Maj presented an analysis of the International Metastatic Renal Cell Carcinoma Data Consortium (IMDC) evaluating real-world outcomes of first-line dual immunotherapy versus combination VEGF immunotherapy in intermediate-poor risk metastatic renal cell carcinoma (mRCC).
Current first-line therapy for mRCC is dual immunotherapy (IPI-NIVO) or a combination of immunotherapy with a VEGFR inhibitor (IOVE). Data from CheckMate-214 suggests that there may be durable disease control with Ipi-Nivo that has not been seen in IOVE trials.1 Real world data is lacking to compare the relative effectiveness of these regimens
Using the IMDC, Dr. Maj and colleagues performed a retrospective analysis of patients with intermediate or poor risk disease (≥1 IMDC risk factor), who received first-line therapy with
IPI-NIVO or an approved IOVE combination (avelumab + axitinib, nivolumab + cabozantinib, pembrolizumab + axitinib, or pembrolizumab + lenvatinib). The baseline characteristics, objective response rates (ORR), time to next therapy (TTNT), and overall survival (OS) were compared between IPI-NIVO and IOVE regimens using Cox regression analyses.
The baseline patient characteristics are summarized below. Compared to patients in the IPI-NIVO group, those in the IOVE group were more likely to be older than 65 years old (32% versus 26%, p=0.02) and have bone metastases (43% versus 34.3%, p=0.003). Baseline characteristics were otherwise well-balanced.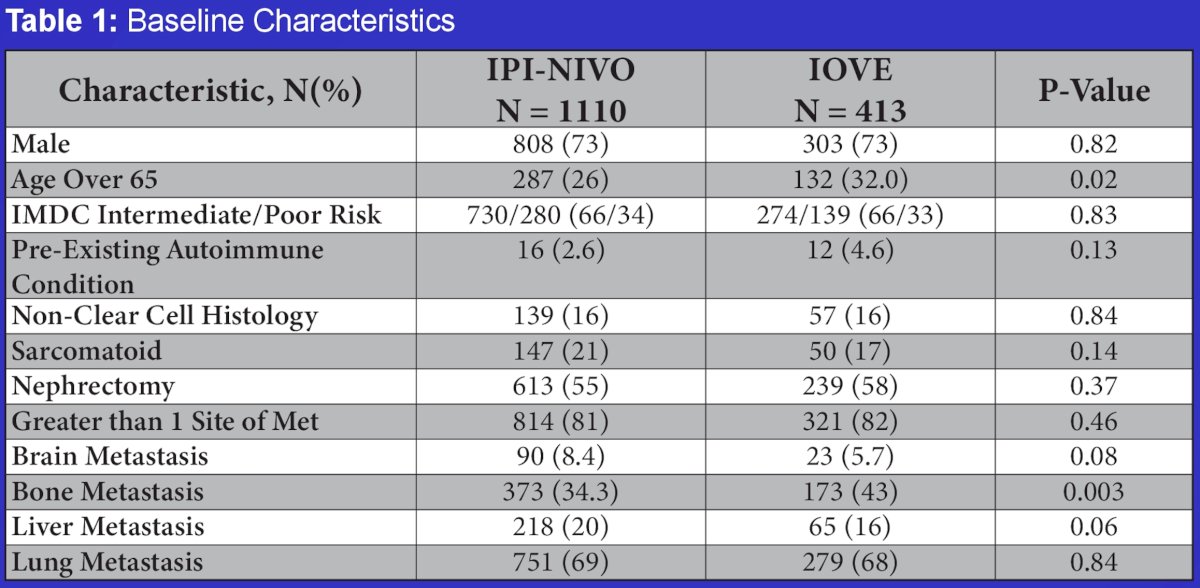
The ORR was superior in the IOVE group (48% versus 39%, p=0.004). This was mainly driven by higher partial response rates (45.6% versus 32.2%).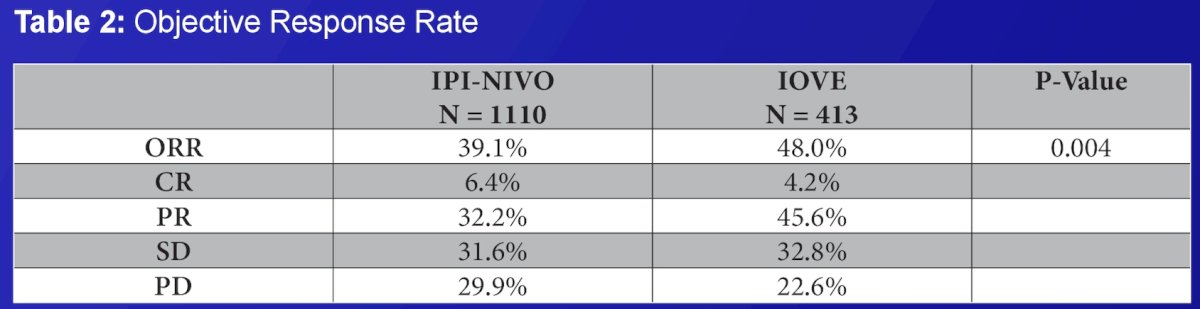
With regards to OS, on multivariable analysis adjusted for IMDC criteria, presence/absence of brain, bone, and liver metastasis, there were no significant differences in survival rates (HR: 0.87, 95% CI: 0.71–1.06, p=0.17).
Differences in survival remained non-significant in an exploratory analysis limited to patients with clear cell histology, ECOG 0-2, and no brain metastasis (p=0.73).
There were no subgroup differences in OS, when stratified by presence/absence of bone metastasis (p=0.98), liver metastasis (p=0.16), lung metastasis (p=0.34), or performance status (p=0.79).
The median time to next treatment in IMDC intermediate-poor risk patients was longer in the IOVE-treated patients (median: 18.6 versus 10.4 months; HR: 0.71, 95% CI: 0.60–0.83, p<0.0001).
Patients receiving IPI-NIVO were more likely to discontinue therapy (75% vs 62%, p<0.0001). There were no significant differences in immune-related adverse events (p=0.09) or reason for immunotherapy discontinuation (p=0.23).
Based on this data, Dr. Maj concluded that first-line ipilimumab + nivolumab and immunotherapy + VEGF regimens have similar real-world survival outcomes.
Presented by: David Maj, MBBS, MSc, Department of Oncology, Arthur JE Child Comprehensive Cancer Centre, University of Calgary, Calgary, AB, Canada
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Reference: