(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a urothelial carcinoma rapid oral abstract session. Dr. Gopa Iyer presented the initial results of FORAGER-1, a first-in-human phase I study of LY3866288 (LOXO-435) in advanced solid tumors with FGFR3 alterations.
LY3866288 is an oral, potent, highly isoform-selective, small molecule FGFR3 inhibitor designed to limit off-target toxicities. In this report, the study investigators presented the initial phase Ia dose escalation results from FORAGER-1, a phase Ia/b study of LY3866288 in FGFR3-altered advanced solid tumors (NCT05614739).
In patients treated at 200 mg twice daily and higher, LY3866288 demonstrates a favorable safety profile and promising preliminary antitumor activity in patients with FGFR3-altered metastatic urothelial carcinoma. 41% (16/39) of patients with an activating FGFR3 mutation or fusion had a confirmed response with a 90% disease control rate. 50% (6/12) of patients who previously received an FGFR inhibitor had a confirmed response. LY3866288 was well-tolerated. Grade 1–2 diarrhea was the most common treatment-emergent adverse event, and high-grade FGFR-1, 2, and 4 mediated adverse events, typical of erdafitinib and other pan-FGFR inhibitors, were very rare.
Activating FGFR3 genetic alterations (most commonly S249C) occur in 15-20% of metastatic urothelial cancers (mUC) and <5% of other solid tumors. Erdafitinib, a pan FGFR1-4 inhibitor, improves survival in FGFR3-altered mUC treated in the 2nd and 3rd line settings (median overall survival: 12.1 months; confirmed objective response rate: 35%), but has clinical toxicities driven by off-target FGFR-1, 2, and 4 inhibition.1
LY3866288 is an oral, highly potent and isoform-selective small molecule FGFR3i designed to limit off-target toxicities.2
The study design with the eligibility criteria and objectives is illustrated below. The phase 1a dose escalation portion included 107 patients with solid tumors and an eligible FGFR3 alteration on local testing. Cohort A1 evaluated 10 dose levels (6 mg QD to 400 mg twice daily).
Cohort A2 is evaluating 200 mg, 300 mg and 400 mg twice daily dosages in patients with metastatic urothelial carcinoma and activating FGFR3 mutations/fusions.
Phase 1b will include two cohorts:
- Cohort B: Metastatic urothelial carcinoma
- Cohort C: Non-urothelial carcinoma solid tumors
The key objectives of the phase 1a/b trial are as follows:
- Safety and tolerability
- Determine optimal dose
- Pharmacokinetics
- Preliminary efficacy per RECIST v1.1

The baseline patient characteristics of Cohort A1 are summarized below. Urothelial carcinoma patients accounted for 65% of the cohort. The median number of prior regimens received in the advanced/metastatic setting was 3. 21% had received prior FGFR3 inhibitor therapy. The FGFR3 alterations were:
- Mutations (56%)
- Fusions (34%)
- Ligand amplifications (10%)
- FGFR3 amplifications (7%)

The baseline characteristics of the metastatic urothelial carcinoma cohort (Cohort A2 of the phase 1a dose escalation) are summarized below. 44% of the 39 patients had upper tract disease. The median number of prior regimens received in the advanced/metastatic setting was 3. 79% had received prior PD-1/L-1 inhibitor therapy and 79% had received prior platinum-based chemotherapy. The most common FGFR3 alteration was a mutation (82%).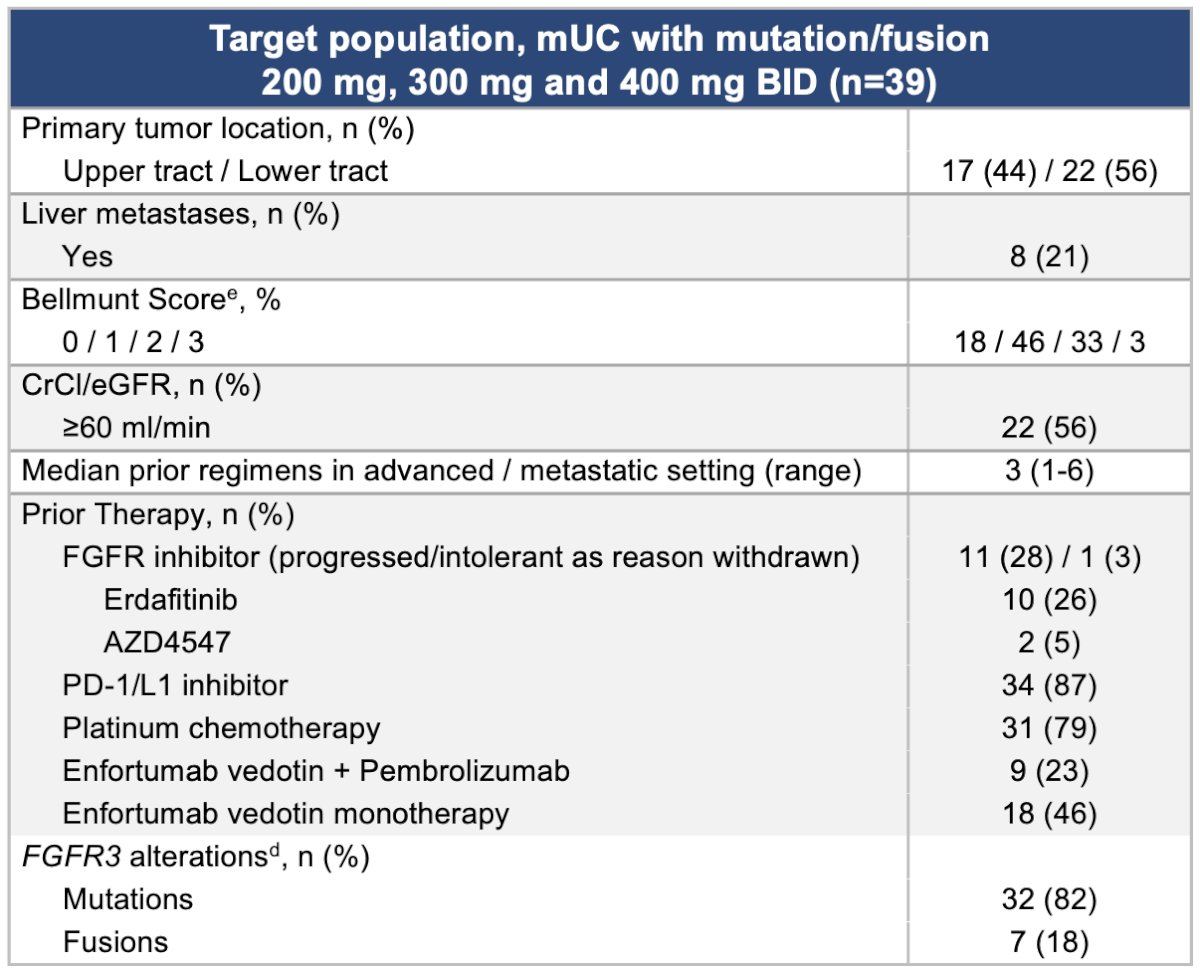
Exposures at doses ≥200 mg twice daily achieved FGFR3-S249C IC90 for the entire dosing interval. Exposures increased with escalating doses, and at highest dose levels remained below FGFR-1, 2, or 4 IC50. No significant differences in exposures were observed in subjects with moderate renal insufficiency (eGFR 30-49 cc/min).
The median follow-up was 5 months. Ten dose levels were evaluated (6 mg once daily – 400 mg twice daily). No dose-limiting toxicities were observed during dose escalation. At the higher dose levels (200, 300, 400 mg BID):
- 25 (36%) remained on treatment at data cutoff
- Most treatment emergent adverse events were grade 1–2 in nature
- High-grade FGFR-1, 2, and 4 related adverse events typical for erdafitinib were very rare
- Dose reductions/discontinuations were uncommon

Among the 39 evaluable metastatic urothelial carcinoma patients in Cohort A2, the confirmed objective response rate was 41%, including 50% in those who had received a prior FGFRi. Overall, the disease control rate was 90%.
Changes (i.e., decreases) in FGFR3 variant allele frequency at Cycle 2, Day 1 correlated with the best observed response.
The median time to response was 1.4 (1.2-2.6) months. 12/16 (75%) confirmed responders remain on treatment; the median duration of response is immature.

Dr. Iyar concluded as follows:
- LY3866288 demonstrates
- Promising preliminary efficacy in patients with FGFR3-altered metastatic urothelial carcinoma treated with ≥200 mg BID
- 41% (16/39) of patients with an activating FGFR3 mutation or fusion had a confirmed response with a 90% disease control rate
- 50% (6/12) of patients who previously received an FGFR inhibitor had a confirmed response
- Favorable safety profile
- Diarrhea was the most common treatment-emergent adverse event and was predominantly low grade and manageable
- High-grade FGFR-1, 2, and 4 mediated adverse events (e.g. nail/skin disorders and ocular toxicity) typical of pan-FGFR inhibitors were very rare
- Randomized dose finding is currently enrolling patients to 200 mg, 300 mg, and 400 mg twice daily doses to select an optimal dose for further development
- Select expansion cohorts, including enfortumab vedotin + pembrolizumab + LY3866288 in the 1st line metastatic urothelial carcinoma setting will open in Q1 2025
Presented by: Gopa Iyer, MD, Associate Attending, Medical Oncologist, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Loriot Y, et al. Erdafitinib or Chemotherapy in Advanced or Metastatic Urothelial Carcinoma. N Engl J Med. 2023; 389(21):1961-71.
- Ballard JA,. et. al. 2021 Mol Cancer Ther 20 (12_Suppl) P141.