(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a urothelial carcinoma rapid oral abstract session. Dr. Noah Hahn presented the results of HCRN GU16-243: ADAPT-BLADDER Cohort 4, a phase I/II trial of durvalumab plus intravesical gemcitabine and docetaxel in BCG-unresponsive non-muscle invasive bladder cancer (NMIBC) patients.
Despite recent FDA approvals of new therapeutic options for patients with high-risk NIMBC, a need persists to investigate novel regimens that safely yield high complete response (CR) rates. Both the intravesical gemcitabine plus docetaxel (Gem/Doc) doublet and intravenous agents targeting the PD-(L)1 immune checkpoint have demonstrated CRs in BCG-unresponsive.
NMIBC trials.1-3 With this in mind, Dr. Hahn and colleagues aimed to assess the clinical efficacy and safety of durvalumab in combination with intravesical Gem/Doc in BCG-unresponsive NMIBC patients
The multi-arm, multi-stage ADAPT-BLADDER trial design has been previously described.4 Herein, Dr. Hahn reported the outcomes from the durvalumab + Gem/Doce (cohort 4) phase 1 and phase 2 expansion arms.
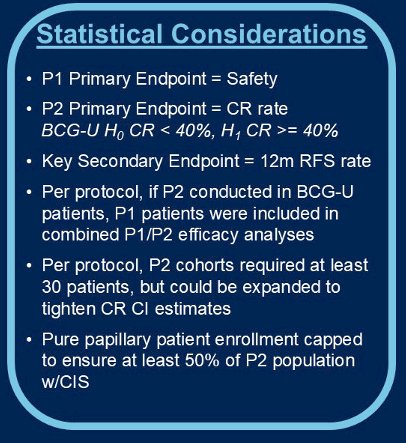
In phase 1, BCG-unresponsive NMIBC patients were enrolled in a 6 + 3 + 3 fashion to establish safety. In phase 2, additional patients were enrolled to evaluate the primary endpoint of CR rate in the total study population and to provide a CR rate estimate within the subset of patients with CIS. Per protocol, phase 1 and 2 efficacy analyses were combined. Enrollment of pure papillary patients was capped to ensure at least 20 patients with CIS.
Patients received durvalumab 1,500 mg intravenously on day 1 of each 4-week cycle for up to 6 cycles. In addition, they received intravesical Gem 1000 mg + Doce 37.5 mg weekly for the first 6 weeks. Patients achieving a CR were encouraged, but not required, to receive Gem/Doce monthly maintenance therapy. Cystoscopic and urine cytology assessments were performed every three months in year one, with a mandatory biopsy at 12-months in responding patients. Toxicity rates were reported per CTCAE v5.0.
The detailed disease evaluation protocols, complete response definition, and statistical methods are summarized below:

Between January 2022 and October 2024, 40 patients enrolled (phase 1, n=12; phase 2, n=28) from 6 sites. The study completed its full planned accrual. The baseline patient demographics are summarized in the table below. The median age was 69 years, and 83% of patients were male. The median number of prior BCG regimens received was 2.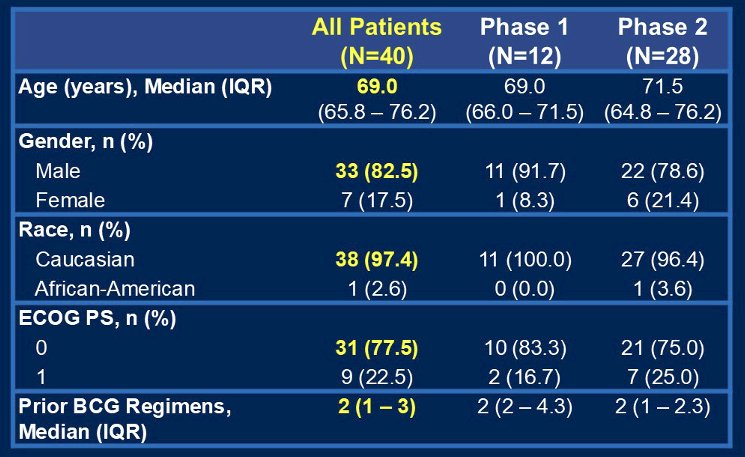
48% of patients had pure papillary disease (HG Ta or T1), and 53% had CIS disease (CIS +/- HG Ta or T1).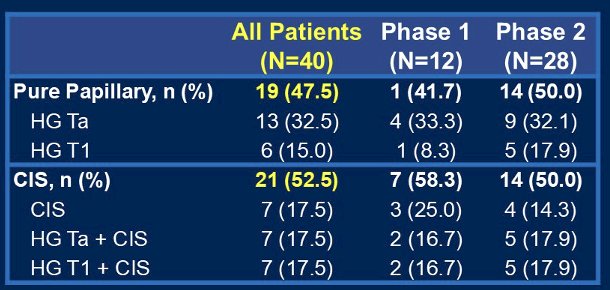
No dose limiting toxicities were observed in the phase 1 portion. Low rates of Grade 3 events were observed (5%; pulmonary in nature), and there were no Grade 4 treatment-related adverse events. No new durvalumab or Gem/Doce treatment-related AEs were observed. One on-study death due to spontaneous retroperitoneal bleed occurred in a patient on anti-coagulation. This was deemed unrelated to study therapy by both the treating investigators and the study DSMB.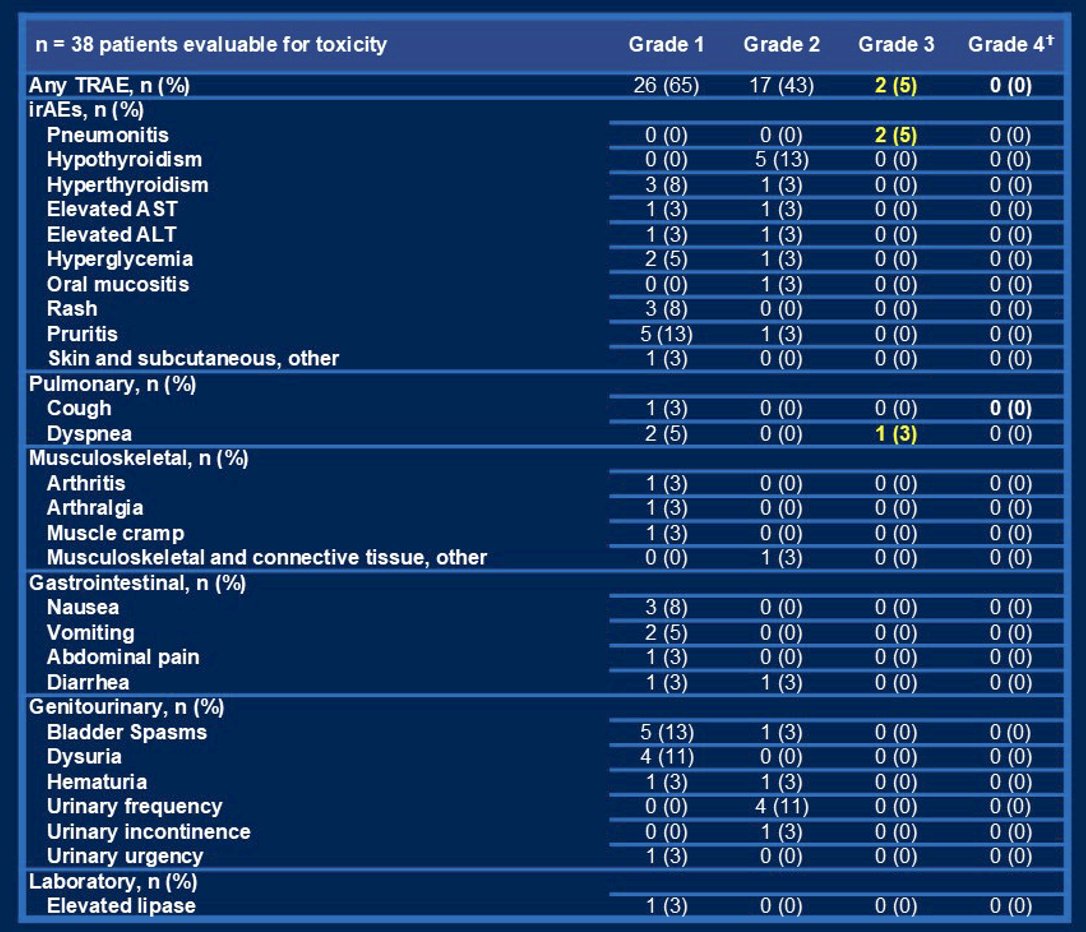
Among 37 evaluable patients for response, 33/37 (89%) had a complete response. The proportions of CRs were similar among CIS (90%) and pure papillary disease (88%) patients.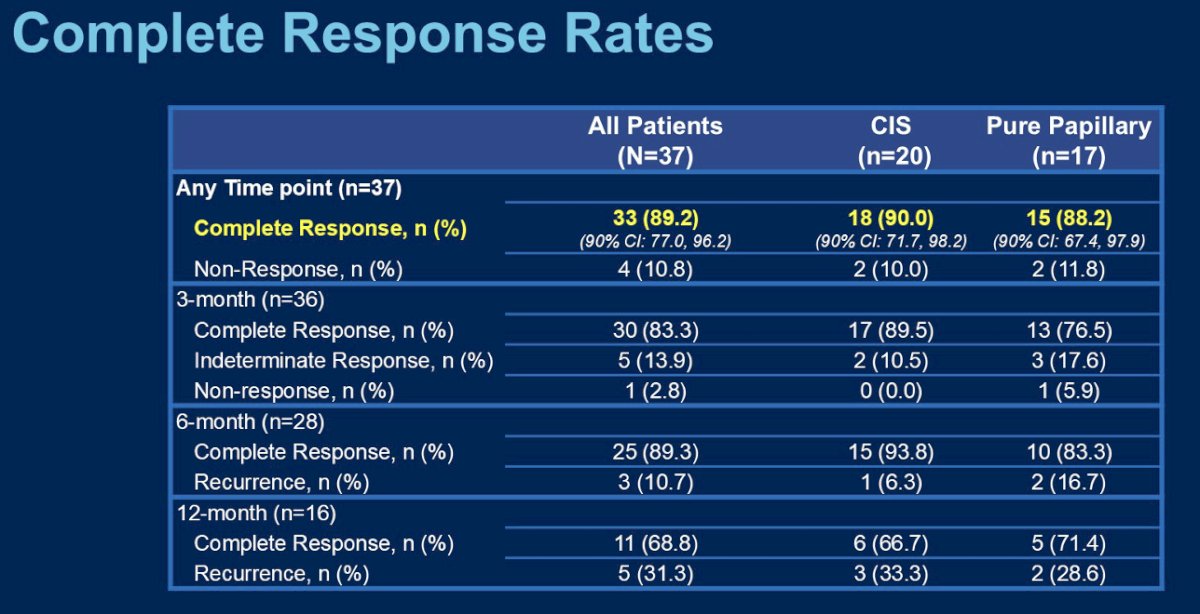
23/33 (70%) CRs are ongoing. 10 (27%) NMIBC recurrences and 3 (8%) MIBC recurrences were observed. Of the 4 recurrences detected at the 12-month time point, 1 had a normal cystoscopy and (-) cytology.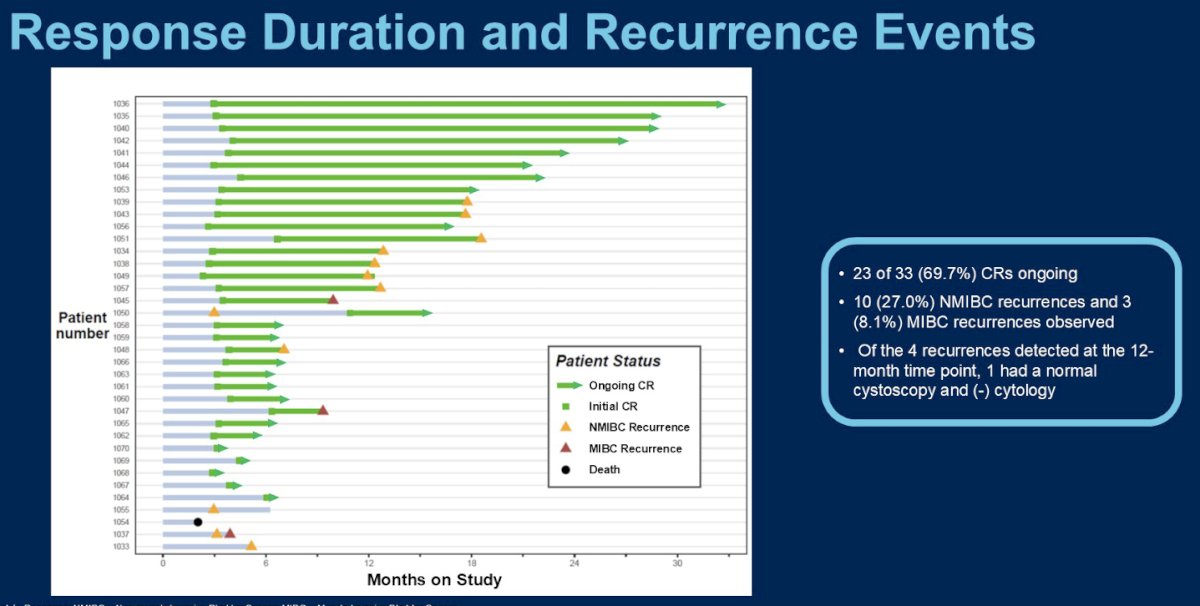
Dr. Hahn concluded as follows:
- Combination therapy with durvalumab plus the intravesical combination of gemcitabine and docetaxel demonstrated a complete response rate of 89% in BCG-unresponsive NMIBC patients
- The study achieved its pre-specified efficacy threshold to qualify as a positive trial
- The toxicity profile is consistent with prior durvalumab studies in advanced urothelial carcinoma patients
- Durable complete responses have been observed, and further results are still maturing
- The multi-arm, multi-stage infrastructure of the ADAPT-BLADDER trial presents an efficient approach to evaluate safety and initial efficacy readouts of novel NMIBC regimens
Presented by: Noah Hahn, MD, Associate Professor of Oncology and Urology at the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins in Baltimore, MD.
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Steinberg RL, Thomas LJ, Brooks N, et al. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. 2020; 203(5):902-9.
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021; 22(7):919-30.
- Black PC, Tangen CM, Singh P, et al. Phase 2 Trial of Atezolizumab in Bacillus Calmette-Guérin-unresponsive High-risk Non-muscle-invasive Bladder Cancer: SWOG S1605. Eur Urol. 2023; 84(6):536-44.
- Hahn NM, O’Donnell MA, Efstathiou JA, et al. A Phase 1 Trial of Durvalumab in Combination with Bacillus Calmette-Guerin or External Beam Radiation Therapy in Patients with Bacillus Calmette-Guerin–unresponsive Non–muscle-Invasive Bladder Cancer: The Hoosier Cancer Research Network GU16–243 ADAPT-BLADDER Study. Eur Urol. 2023; 83(6):486-94.