(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a urothelial carcinoma rapid oral abstract session. Dr. Pooja Ghatalia presented the results of RETAIN-2, a phase II trial of risk enabled therapy after neoadjuvant chemo-immunotherapy for muscle-invasive bladder cancer (MIBC).
Cisplatin-based neoadjuvant chemotherapy (NAC) followed by radical cystectomy (RC) or chemoradiotherapy (CRT) is the standard of care for patients with muscle invasive bladder cancer (MIBC). Mutations in DNA damage repair genes enrich for pathologic downstaging after NAC.
In RETAIN-1, a risk-adapted approach was employed to identify patients for cystectomy-sparing active surveillance (AS) following NAC, reporting a 73% 2-year metastasis-free survival (MFS) rate.1 RETAIN-2 employs a similar approach but incorporates neoadjuvant chemoimmunotherapy.
This is a phase II, multi-institutional trial in which patients with cT2-T3N0M0 MIBC, ECOG PS 0-1, and CrCl ≥50 mL/min received the combination of neoadjuvant dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin (ddMVAC) plus nivolumab. Pre-NAC transurethral bladder resection (TURBT) specimens were sequenced for mutations (pathogenic or variant of unknown significance [VUS]) in ATM, ERCC2 or RB1. Patients with >1 mutation and clinical complete response (cCR) post-NAC (based on restaging TUR, urine cytology and CT imaging) initiated active surveillance (AS). The remaining patients (i.e., those without a mutation and/or no clinical complete response) underwent bladder-directed therapy: intravesical therapy (< cT2 post-NAC), chemoradiotherapy, or radical cystectomy. The primary endpoint of this study is 2-year MFS for ITT patient (data not mature yet). This interim analysis reports clinically meaningful secondary endpoint outcomes.
A total of 80 patients were treated over 40 months at four academic centers and 71 were evaluable per protocol. The median age was 69 years (range: 66-86), 77% were male, 80% had ECOG PS 0 and 87% were cT2.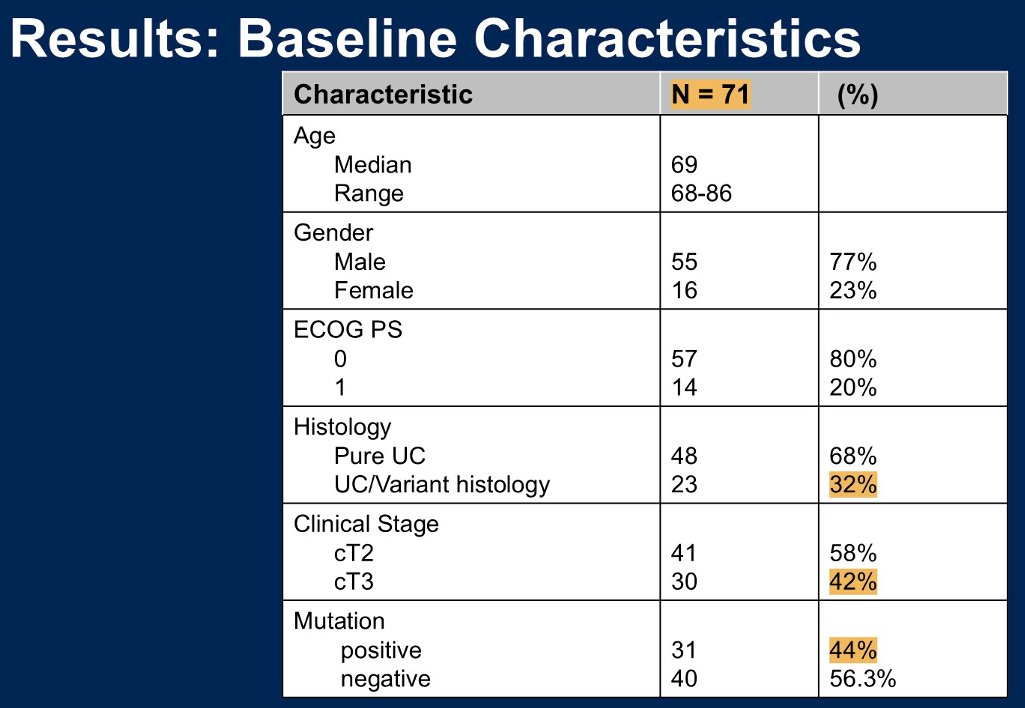
Of 80 treated patients, 60 (75%) completed three cycles of ddMVAC with nivolumab; seven tolerated only one cycle, and two died shortly after completing three cycles from treatment-related adverse events and were not evaluable for the primary endpoint.
Grade 3-4 treatment-related adverse events (TRAEs) occurred in 19% of all treated patients. Two deaths occurred with ddMVAC/nivolumab after completing 3 cycles, secondary to multi-organ failure and an AKI. One death was observed in a chemoradiotherapy-treated patient likely related to pneumonitis.
Of 71 evaluable ITT patients, 31 (44%) had a mutation of interest and the cCR rate in those patients was 71%. Thirty-five patients proceeded directly to radical cystectomy, 10 received chemoradiotherapy, three received intravesical therapy, and 23 patients started AS, per protocol. Among cystectomy patients, 40% were found to have no residual disease (i.e., ypT0) and 63% were ≤ypT1. Among patients who opted for intervention, 85% remained free of metastases.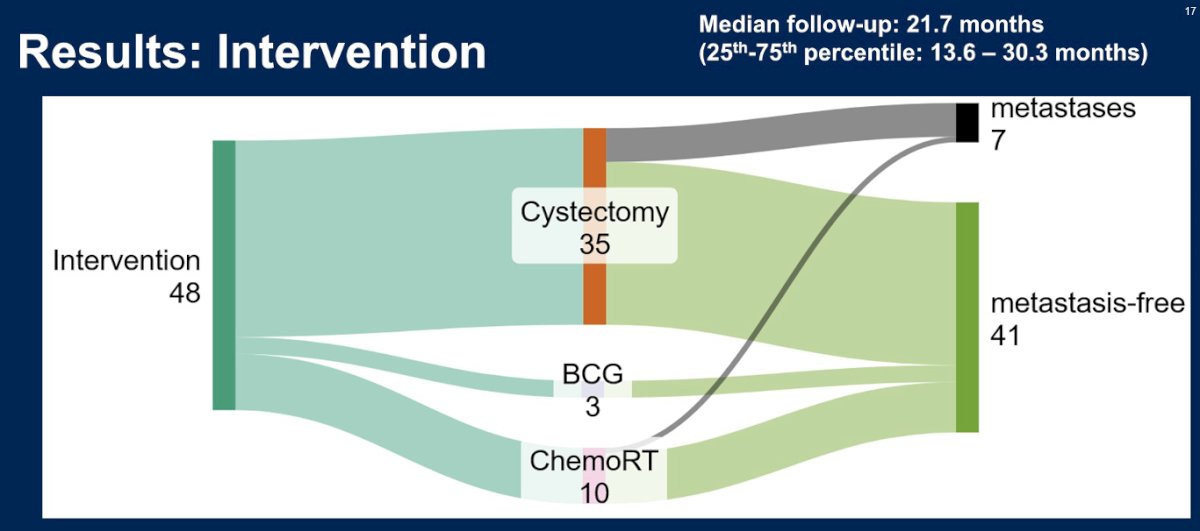
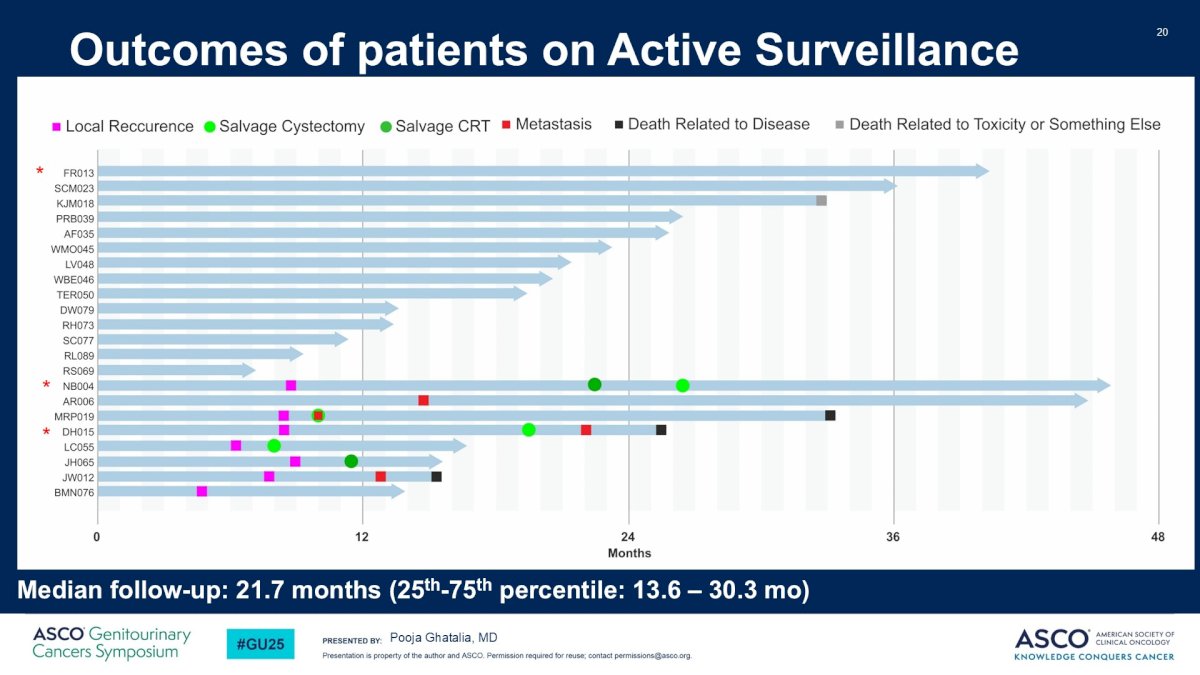
Of the 19 patients who were assigned to and accepted AS, 16 (84%) remained intervention-free after 21.7 months median follow-up (2 underwent cystectomy, 1 chemoradiotherapy). Two patients who remained intervention-free developed metastases, and 1/2 who underwent a delayed cystectomy developed metastases. Among AS patients, 82% remained metastases-free, and 60% remained metastases-free and with an intact/un-radiated bladder.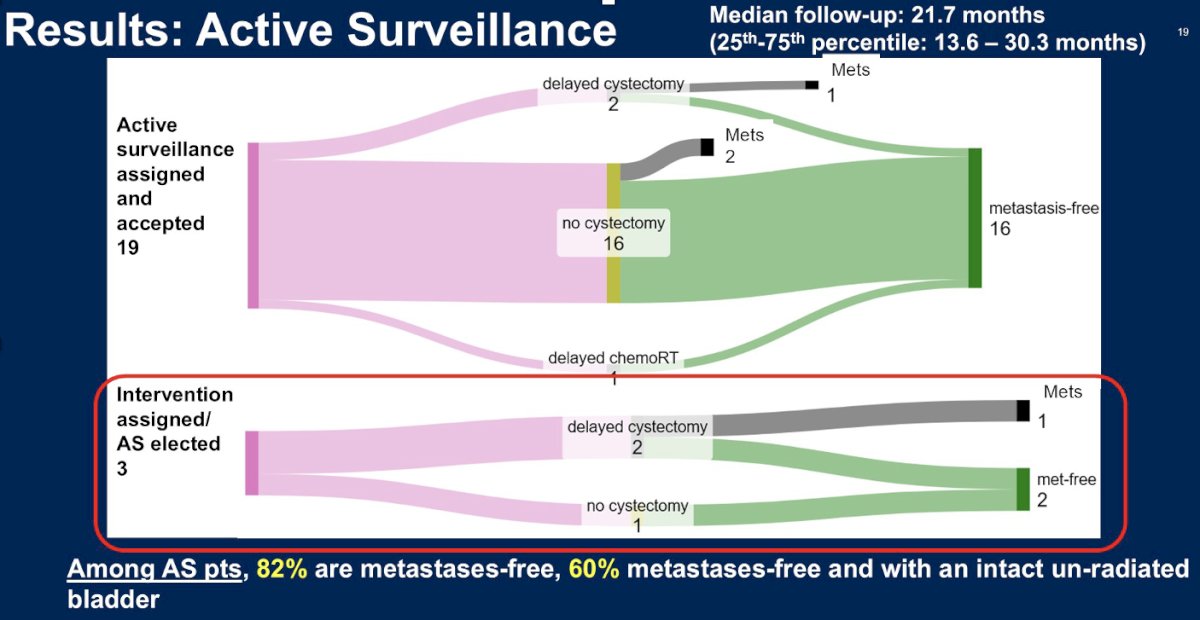
In the ITT population, the 2-year MFS and OS rates are 77.4% and 93%, respectively.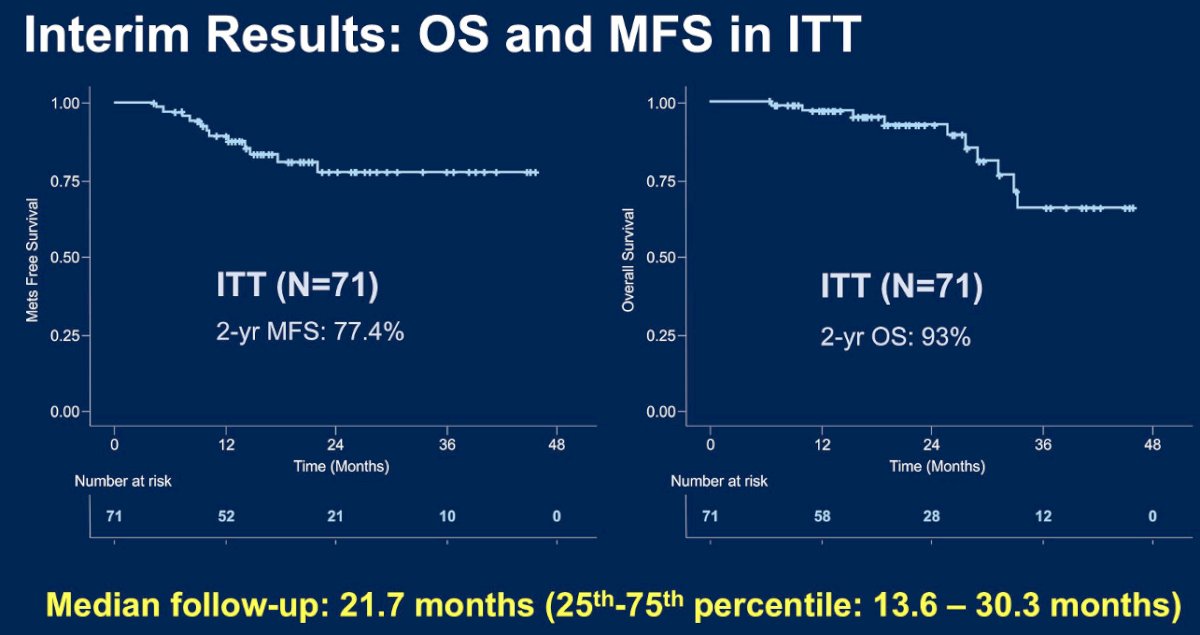
A quick comparison of the results of RETAIN-1 versus RETAIN-2 demonstrates that for RETAIN-2 patients:
- Metastasis-free survival in active surveillance patients is superior to date (82% versus 64), albeit with a short median duration of follow-up (22 versus 40 months)
- Higher ypT0 rates in cystectomy patients (40% versus 15%)
- Local recurrence rates in AS patients are lower (32% versus 62%)
- The metastasis-free and intact unirradiated bladder proportion is higher (60% versus 48%)

Dr. Ghatalia concluded as follows:
- At the time of interim analysis, combination chemoimmunotherapy with ddMVAC + nivolumab was associated with a metastases-free survival rate of 84.2% in ITT and 82% in the active surveillance arm
- 60% of active surveillance patients are metastases-free and with an intact un-irradiated bladder
- Compared to RETAIN-1, the ypT0 rate was higher at 40% and rate of pT0 + cCR of 54% in RETAIN-2 suggests an additive benefit of adding nivolumab to ddMVAC
Presented by: Pooja Ghatalia, MD, Assistant Professor, Medical Oncologist, Department of Hematology/Oncology, Fox Chase Cancer Center, Philadelphia, PA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: RETAIN-2 Study Shows Promise for Bladder Cancer Preservation - Pooja Ghatalia