(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Panning for Gold: The Role of ctDNA as a Biomarker for Bladder Cancer Session. Dr. Gillian Vandekerkhove discussed how we could unleash the potential of ctDNA across the spectrum of urothelial carcinoma.
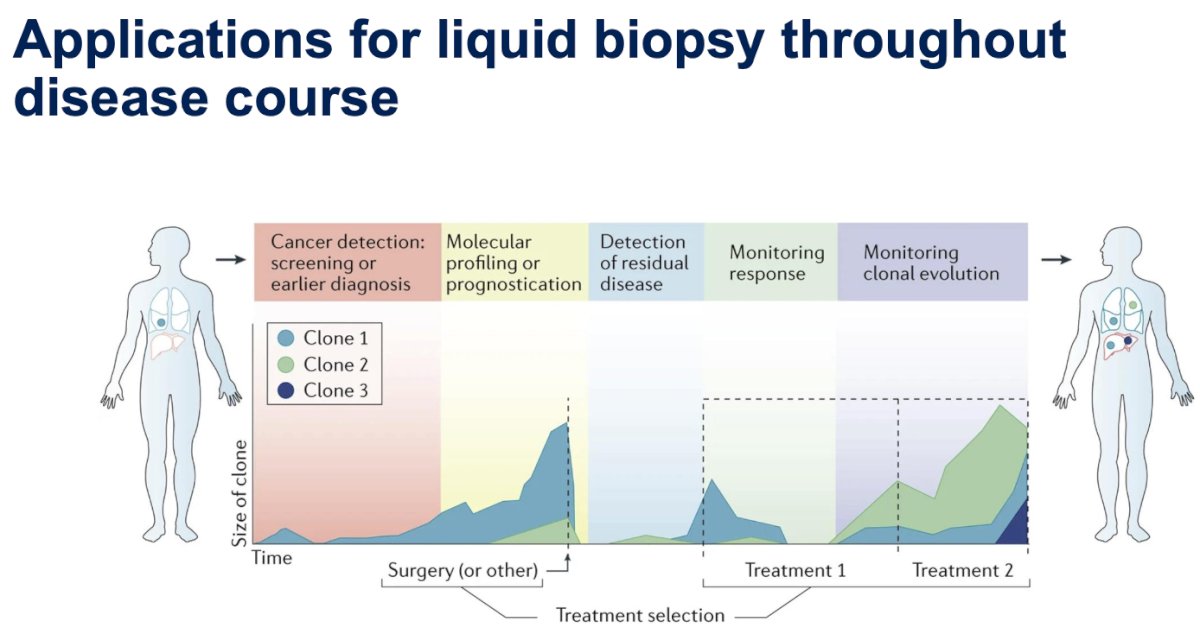
Dr. Vandekerkhove began her presentation by discussing how advancements in genomic and molecular methods are expanding the potential applications of liquid biopsy throughout the disease course. These applications range from cancer detection, screening, and early diagnosis to monitoring clonal evolution after systemic or local treatment. 1
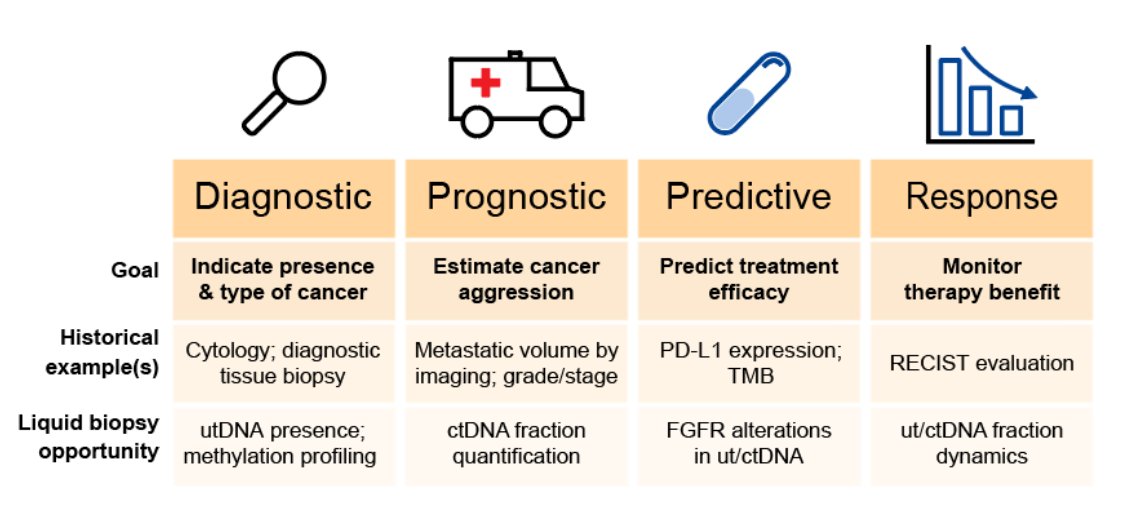
Historically, different biomarker classes have been used across the spectrum of urothelial carcinoma. In the diagnostic process, cytology has been utilized, while metastatic volume by imaging and grade/stage of the disease have been used to estimate cancer aggressiveness. To predict treatment efficacy, biomarkers such as PD-L1 expression status or TMB have been employed. Liquid biopsy presents new opportunities, including utDNA presence in the diagnostic setting, ctDNA fraction for prognostic assessment, and the presence of FGFR alterations or ctDNA as predictors of treatment response as illustrated below.
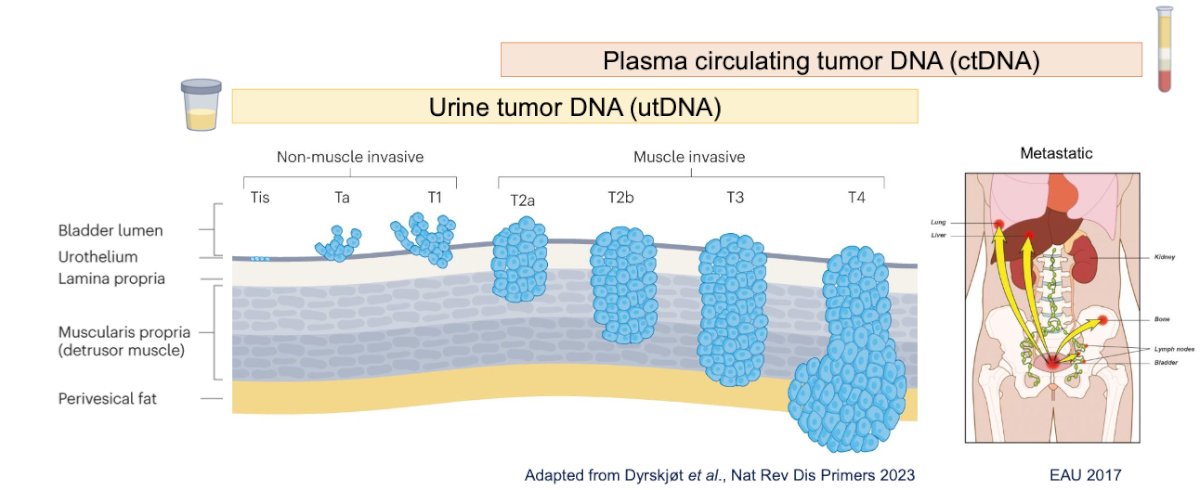
Dr. Vandekerkhove noted that “one size does not fit all” disease stage and the specific clinical question drive the selection of analytes and assays. He proposed using urine liquid biopsy to assess urine tumor DNA (utDNA) for insights into local disease and plasma liquid biopsy (ctDNA) to inform on (micro)metastatic disease.
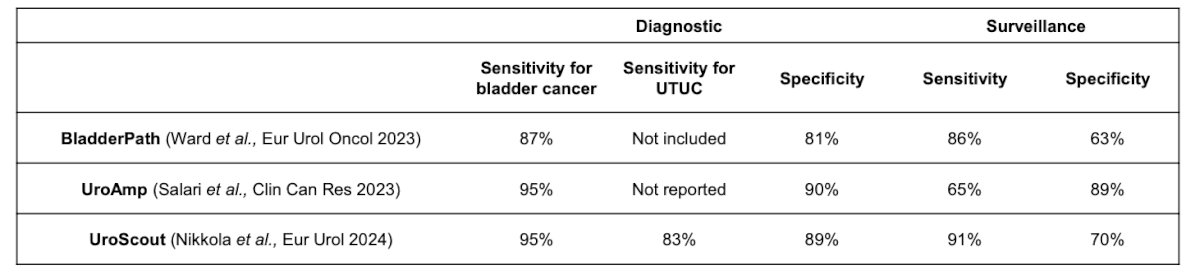
The diagnosis and surveillance of urothelial cancer are shifting from urine assays focused solely on detecting tumor markers (e.g., DNA, mRNA, methylation) to assays that enable both detection and characterization. Multiple liquid biopsy platforms are emerging, including UroScout, a high-volume (up to 100 mL) urine tumor DNA assay detecting mutations in 25 urothelial cancer-associated genes; BladderPath, which utilizes capture-based ultra-deep sequencing for 443 somatic mutations in 23 genes from 591 urine cell-pellet DNAs; and UroAmp, which applies urinary comprehensive genomic profiling (uCGP) to predict the presence and pathological grade of urothelial carcinoma. (2-4) Additional alternatives include CxBladder, UroMark, UroSeek, Xpert Bladder, UroCad, and BladderCARE.
Recent multi-gene urine DNA sequencing assays with high sensitivity and specificity have the potential to augment cytology and cystoscopy for hematuria evaluation. Notably, the sensitivity for detecting bladder cancer in the diagnostic setting is 95% for UroScout and UroAmp and 87% for BladderPath, with comparable sensitivity in the surveillance setting, as shown below. (2-4) Moreover, prospective assessments of urine biomarker clinical utility are ongoing (e.g., NCT03988309, NCT06310759).
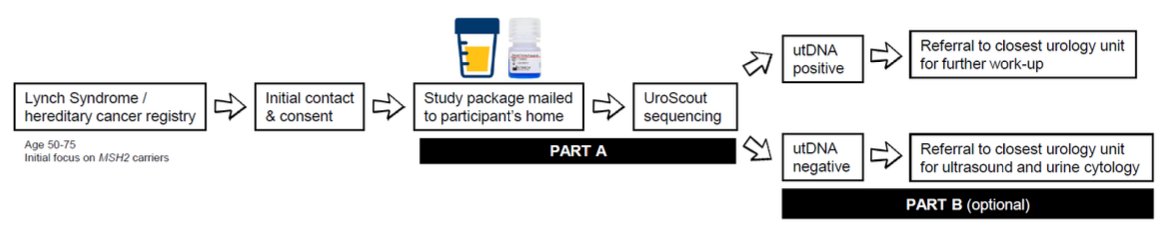
Dr. Vandekerkhove discussed the challenges of detecting urothelial carcinoma (UC) in asymptomatic, high-risk populations such as those with Lynch syndrome (LS), an inherited cancer predisposition caused by germline MMR gene variants. Individuals with LS have a ~25% lifetime risk of UC, with a higher prevalence of upper tract UC and earlier onset.
The LS-URO study (NCT06218433) seeks to improve early detection through a collaboration between uro-oncology and hereditary cancer specialists. Participants enroll via the Finnish LS Registry and BC Cancer Hereditary Cancer Program, receiving a home-based study package that includes UroScout sequencing and a urine collection kit with DNA preservative. Samples are analyzed for tumor-derived DNA, with positive cases referred to urology clinics and negative cases offered optional follow-up. This innovative, non-invasive strategy aims to facilitate early UC detection and personalized risk-based management.
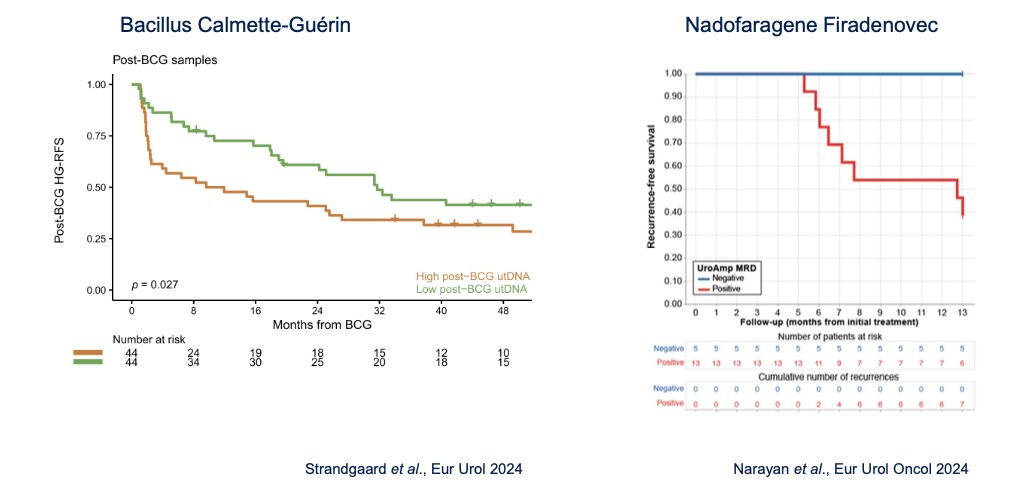
Urine tumor DNA (utDNA) is emerging as a valuable biomarker for monitoring response to intravesical therapy in NMIBC. Post-treatment detection of utDNA serves as an indicator of minimal residual disease (MRD) and predicts recurrence. Two exploratory studies showed that patients treated either with BCG or Nadofaragene Firadenovec who had high post-treatment uTDNA were associated with significantly higher risk of HG recurrence. (5)
In Canada, the EVER trial (NCT05037279), led by Drs. Zlotta and Kulkarni, is investigating this approach. This multicenter, phase III noninferiority trial compares OncoTICE versus Verity-BCG for intermediate- and high-risk NMIBC, integrating urine collection into a comprehensive biomarker strategy alongside blood and tissue analysis.
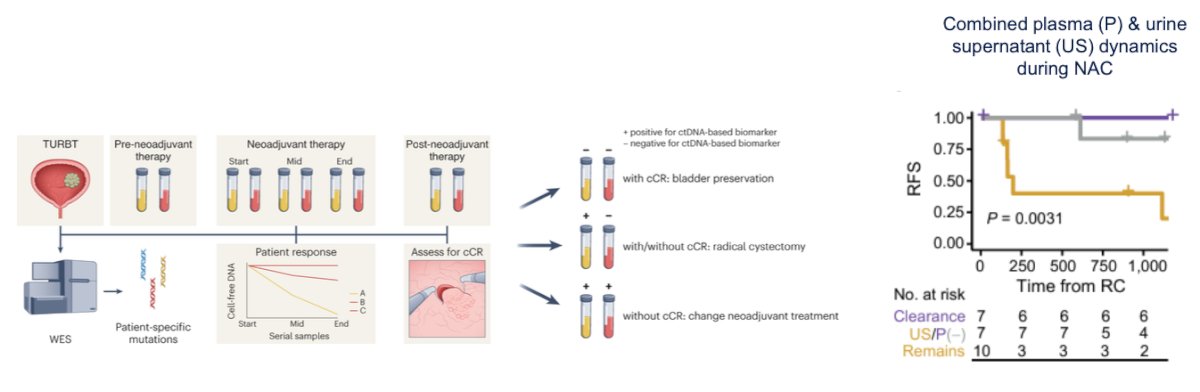
Urine and plasma offer complementary insights into treatment response during neoadjuvant therapy for MIBC. Proof-of-principle data suggest that analyzing the dynamics of these biomarkers can help assess patient response to neoadjuvant chemotherapy and predict recurrence-free survival. 6
In the adjuvant setting, plasma ctDNA is emerging as a transformative tool in clinical practice. Prospective trials are evaluating ctDNA positivity (i.e., MRD) post-cystectomy to guide adjuvant therapy. Personalized, tumor-informed assays are expected to enhance ctDNA detection, refine treatment decisions, and predict therapeutic response. Notable ongoing trials include TOMBOLA (NCT04138628), IMvigor011 (NCT04660344), and MODERN (NCT05987241).
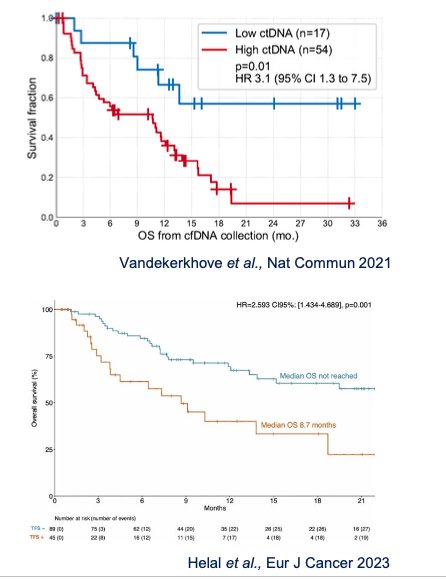
In the advanced disease setting, plasma ctDNA levels correlate with overall survival in advanced urothelial carcinoma/ Quantification of circulating tumor DNA—assessing tumor fraction and purity—before initiating therapy provides a strong prognostic signal, consistently observed across various clinical scenarios and treatment regimens. (7) Notably, this association extends beyond UC and has been demonstrated in pan-cancer studies. The figures below show how low vs high ctDNA status significantly predicts survival in advanced UC.
Clinically relevant alterations can be detected in both ctDNA and utDNA, providing valuable insights for tumor characterization, such as identifying FGFR3 mutations and fusions. Detecting actionable alterations in plasma or urine enables precision-guided targeted therapy. Additionally, serial sampling offers a unique opportunity to track clonal evolution in UC patients, revealing emerging resistance mechanisms in response to treatment (Kinase domain resistance mutations in plasma ctDNA)
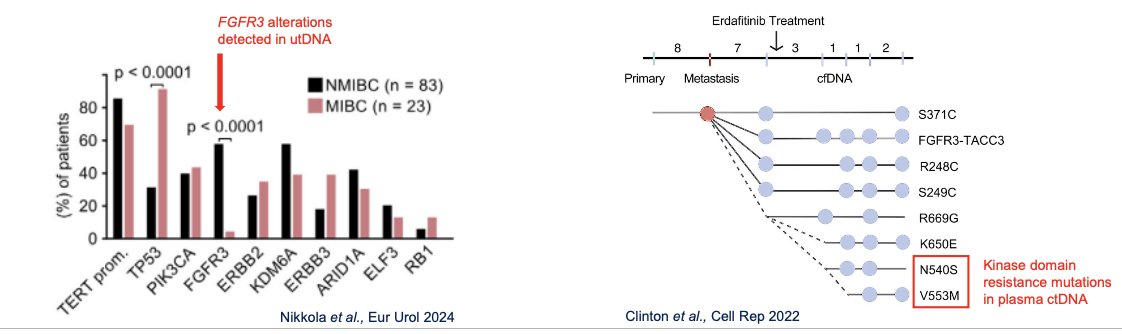
Benchmarking ctDNA and utDNA assays involves comparing them against established tissue-based patient stratification strategies. A prospective pan-Canadian trial (NCT06129084) is evaluating the added value of plasma ctDNA testing alongside standard tumor tissue FGFR biomarker assessment. This study has met its enrollment target of 260 metastatic UC patients, assessing FGFR genotype in both tumor tissue and ctDNA to identify candidates for erdafitinib. Additionally, ongoing ctDNA collection at disease progression aims to investigate acquired resistance mechanisms.
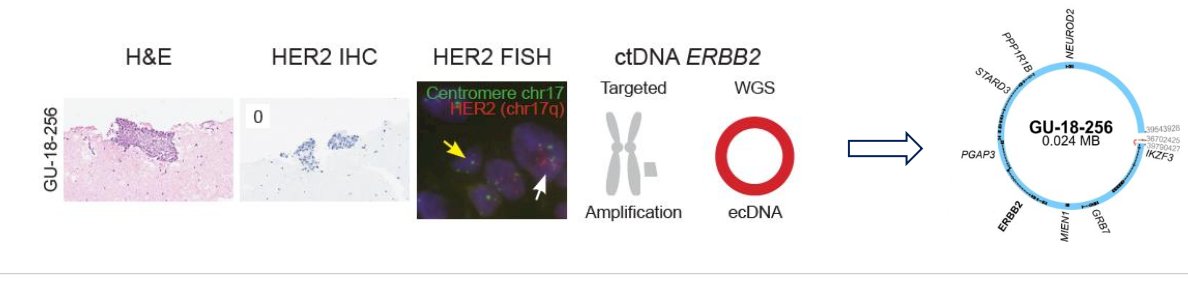
In addition to FGFR3, tumor characterization using ctDNA and utDNA can also identify ERBB2/HER2 alterations. Benchmarking these assays against established tissue-based stratification strategies is essential. ctDNA analysis detects ERBB2 oncogenic mutations and amplifications, as well as evidence of ERBB2 extrachromosomal DNA (ecDNA). Furthermore, serial sampling reveals spatiotemporal heterogeneity, highlighting the dynamic evolution of ERBB2/HER2 alterations in metachronous tissue and plasma from patients with metastatic UC.
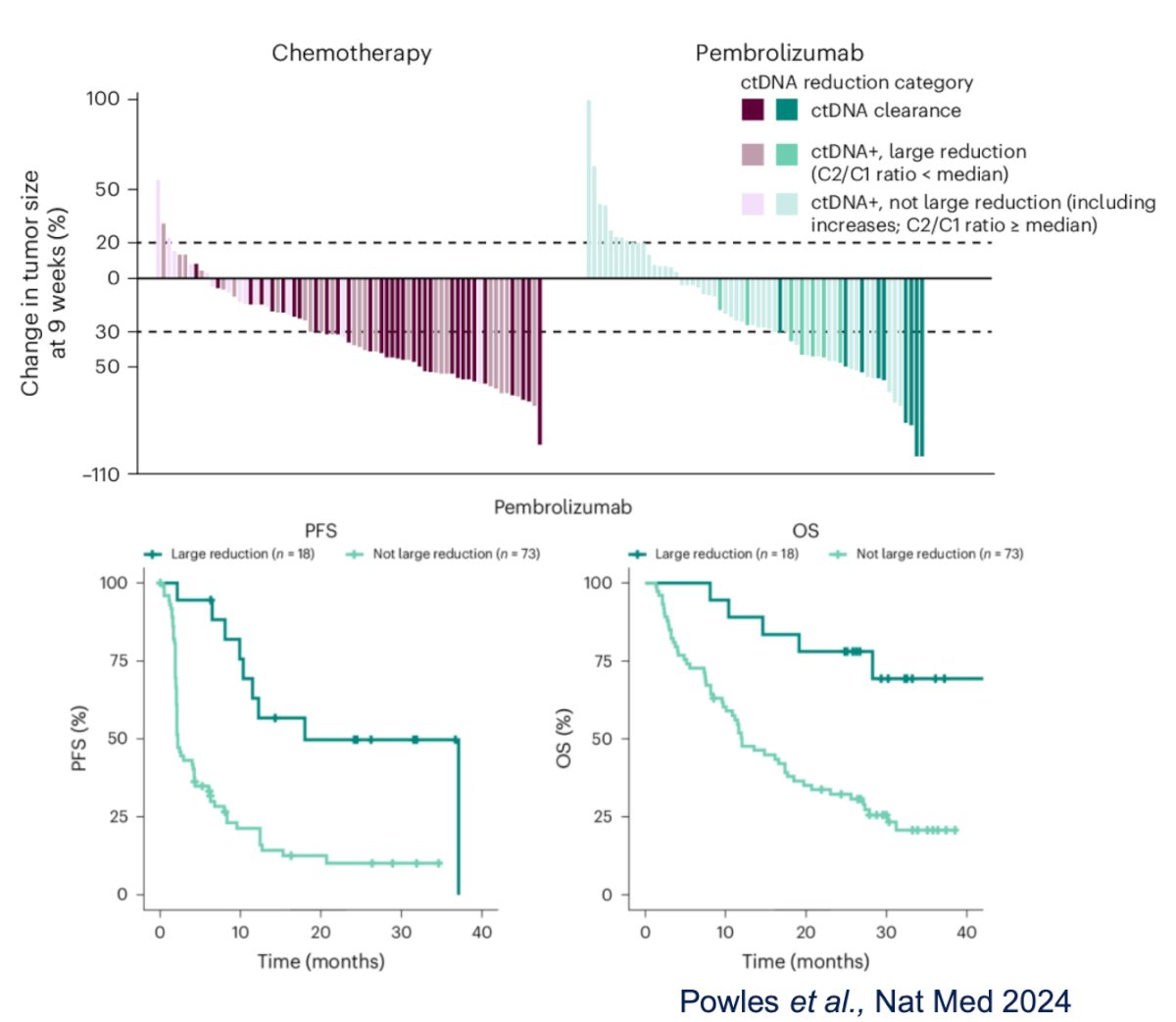
Dr. Vandekerkhove highlighted that plasma ctDNA dynamics correlate with treatment response in advanced UC. On-treatment changes in ctDNA levels can distinguish responders from non-responders, providing an early signal of efficacy before imaging at 3 or 6 weeks, including in patients with non-measurable disease. In the Tolmeijer study, a ctDNA decline at 3 weeks on immune checkpoint inhibitors (ICI) was associated with improved progression-free survival (PFS) and overall survival (OS). Similarly, in the pembrolizumab arm of KEYNOTE-361, radiographic response and survival outcomes were linked to the extent of ctDNA reduction. 8
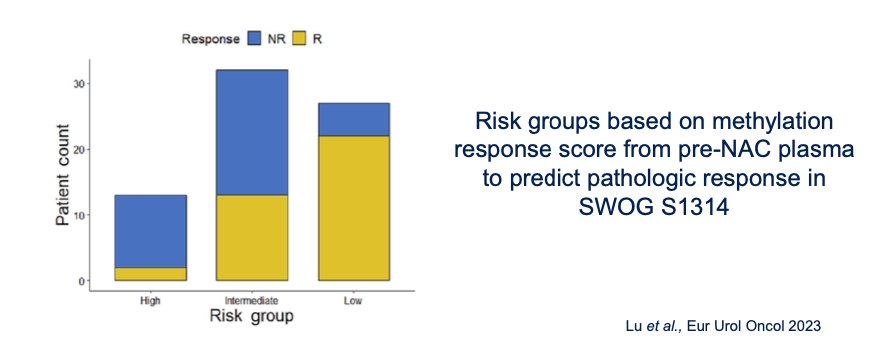
Liquid biopsy is evolving beyond genetic alterations to incorporate multi-omic and multi-analyte models, enabling the development of comprehensive composite biomarkers for cancer detection and treatment personalization. Epigenomics, particularly DNA methylation profiling, plays a key role in tumor stratification, with urine tumor DNA methylation showing potential for improved diagnosis and plasma ctDNA methylation offering insights into tumor phenotype.
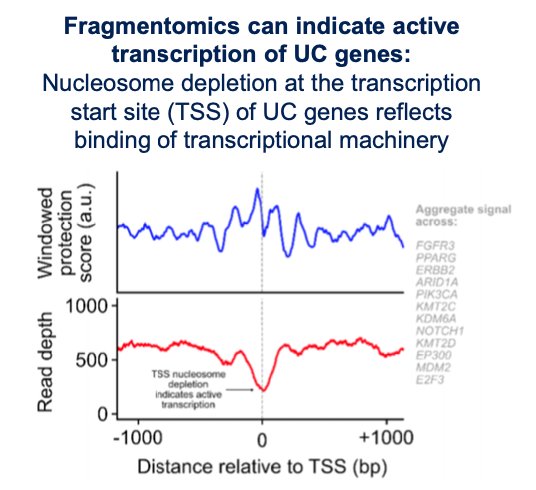
Moreover, fragmentomic analysis of cell-free DNA offers a novel approach to infer chromatin architecture using existing sequencing data rather than requiring a new assay. This technique can provide insights into the expression of therapeutic target genes (e.g., FGFR3, TROP2, NECTIN4, HER2), identify histologic subtypes, and monitor treatment-induced changes in transcription factor activity across serial samples.
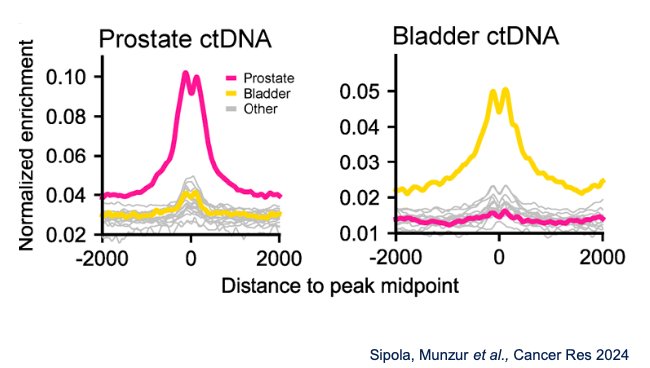
Additionally, plasma cell-free chromatin immunoprecipitation sequencing (cfChIP-seq) enables non-invasive exploration of histone modifications to infer tumor subtypes and metastatic behavior. This approach can distinguish luminal versus basal subgroups, predict predominant sites of metastasis, and identify histologic subtypes such as neuroendocrine differentiation. In urothelial carcinoma (UC), cfChIP-seq captures tumor-specific chromatin features, including H3K4me2 signal enrichment at open chromatin sites, which can differentiate UC from prostate cancer and provide deeper insights into tumor phenotype and evolution as shown below.
Dr. Vandekerkhove emphasized the shift from single-feature analyses to comprehensive multi-parameter models that integrate multiple analytes, omics data, immunological markers, and clinicopathological features. This approach aims to enhance prognostication and prediction of treatment response, providing a more holistic understanding of disease biology. However, translating these complex models into clinical practice remains a significant challenge, requiring standardization, validation, and integration into existing workflow

Dr. Vandekerkhove concluded her presentation with the following key takeaways:
- Plasma ctDNA is poised to impact the clinical management of MIBC and metastatic UC.
- utDNA is emerging as a biomarker across applications in NMIBC and MIBC; however, optimal (pre)analytic approaches are needed, and it is not yet ready for clinical translation.
- The application of next-generation liquid biopsy in UC should incorporate emerging techniques that enable epigenomic and transcriptomic analysis.
- Every trial should collect plasma and serum samples for analysis. Studies do not necessarily need to be biomarker-driven to continue informing on ctDNA clinical performance.
Presented by: Gillian Vandekerkhove, PhD, MSc, Vancouver Prostate Centre, Department of Urologic Sciences, University of British Columbia. Vancouver, BC, Canada.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Wan JCM, Massie C, Garcia-Corbacho J, Mouliere F, Brenton JD, Caldas C, Pacey S, Baird R, Rosenfeld N. Liquid biopsies come of age: towards implementation of circulating tumour DNA. Nat Rev Cancer. 2017 Apr;17(4):223-238. doi: 10.1038/nrc.2017.7. Epub 2017 Feb 24. PMID: 28233803.
- Ward DG, Baxter L, Ott S, Gordon NS, Wang J, Patel P, Piechocki K, Silcock L, Sale C, Zeegers MP, Cheng KK, James ND, Bryan RT; BladderPath Trial Management Group. Highly Sensitive and Specific Detection of Bladder Cancer via Targeted Ultra-deep Sequencing of Urinary DNA. Eur Urol Oncol. 2023 Feb;6(1):67-75. doi: 10.1016/j.euo.2022.03.005. Epub 2022 Apr 8. PMID: 35410825.
- Nikkola J, Ryyppö L, Vuorinen J, Kallio H, Selin H, Jämsä P, Åkerla J, Virtanen T, Pekkarinen T, Kaipia A, Pulkkinen J, Vandekerkhove G, Müller DC, Wyatt AW, Black PC, Nykter M, Veitonmäki T, Annala M. Sensitive Detection of Urothelial Cancer via High-volume Urine DNA Analysis. Eur Urol. 2025 Jan;87(1):86-88. doi: 10.1016/j.eururo.2024.10.014. Epub 2024 Oct 22. PMID: 39443274.
- Salari K, Sundi D, Lee JJ, Wu S, Wu CL, DiFiore G, Yan QR, Pienkny A, Lee CK, Oberlin D, Barme G, Piser J, Kahn R, Collins E, Phillips KG, Caruso VM, Goudarzi M, Garcia-Ransom M, Lentz PS, Evans-Holm ME, MacBride AR, Fischer DS, Haddadzadeh IJ, Mazzarella BC, Gray JW, Koppie TM, Bicocca VT, Levin TG, Lotan Y, Feldman AS. Development and Multicenter Case-Control Validation of Urinary Comprehensive Genomic Profiling for Urothelial Carcinoma Diagnosis, Surveillance, and Risk-Prediction. Clin Cancer Res. 2023 Sep 15;29(18):3668-3680. doi: 10.1158/1078-0432.CCR-23-0570. PMID: 37439796; PMCID: PMC10502470.
- Strandgaard T, Nordentoft I, Birkenkamp-Demtröder K, Salminen L, Prip F, Rasmussen J, Andreasen TG, Lindskrog SV, Christensen E, Lamy P, Knudsen M, Steiniche T, Jensen JB, Dyrskjøt L. Field Cancerization Is Associated with Tumor Development, T-cell Exhaustion, and Clinical Outcomes in Bladder Cancer. Eur Urol. 2024 Jan;85(1):82-92. doi: 10.1016/j.eururo.2023.07.014. Epub 2023 Sep 16. PMID: 37718188.
- Christensen E, Nordentoft I, Birkenkamp-Demtröder K, Elbæk SK, Lindskrog SV, Taber A, Andreasen TG, Strandgaard T, Knudsen M, Lamy P, Agerbæk M, Jensen JB, Dyrskjøt L. Cell-Free Urine and Plasma DNA Mutational Analysis Predicts Neoadjuvant Chemotherapy Response and Outcome in Patients with Muscle-Invasive Bladder Cancer. Clin Cancer Res. 2023 Apr 14;29(8):1582-1591. doi: 10.1158/1078-0432.CCR-22-3250. PMID: 36780195; PMCID: PMC10102843.
- Vandekerkhove G, Lavoie JM, Annala M, Murtha AJ, Sundahl N, Walz S, Sano T, Taavitsainen S, Ritch E, Fazli L, Hurtado-Coll A, Wang G, Nykter M, Black PC, Todenhöfer T, Ost P, Gibb EA, Chi KN, Eigl BJ, Wyatt AW. Plasma ctDNA is a tumor tissue surrogate and enables clinical-genomic stratification of metastatic bladder cancer. Nat Commun. 2021 Jan 8;12(1):184. doi: 10.1038/s41467-020-20493-6. PMID: 33420073; PMCID: PMC7794518.
- Powles T, Csőszi T, Özgüroğlu M, Matsubara N, Géczi L, Cheng SY, Fradet Y, Oudard S, Vulsteke C, Morales Barrera R, Fléchon A, Gunduz S, Loriot Y, Rodriguez-Vida A, Mamtani R, Yu EY, Nam K, Imai K, Homet Moreno B, Alva A; KEYNOTE-361 Investigators. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021 Jul;22(7):931-945. doi: 10.1016/S1470-2045(21)00152-2. Epub 2021 May 26. PMID: 34051178.