(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA was host to a urothelial carcinoma rapid oral abstract session. Dr. Alina Basnet presented the results of a genomic landscape study in young onset cancer patients with clinically advanced urothelial bladder cancer.
Clinically advanced urothelial carcinoma of the bladder is defined by the following features:
- Surgically unresectable bladder cancer (i.e., cT4b)
- Pelvic lymph node positive disease (i.e., cN+)
- Non-regional lymph node disease
- Distant metastatic disease (i.e., cM1)
In this study, young onset bladder cancer was defined by an age at diagnosis of <50 years. Further understanding of the underlying biology of these patients’ disease process is needed to improve upon these patients’ poor oncologic outcomes.1
From a methodology standpoint, ≥50 ng of DNA was extracted from 40 µm of FFPE sections of 9,411 cases of clinically advanced urothelial carcinoma of the bladder. Sequencing was performed on 324 cancer-related genes and introns from 28 genes commonly rearranged in cancer. FDA-approved (F1CDx) hybrid capture-based sequencing using adaptor ligation-based libraries was performed. The mean coverage depth was >600-fold. Base substitutions, insertions and deletions (short variants; SV), rearrangements, and copy number changes were assessed. The tumor mutational burden (TMB) was calculated from 0.80 Mb sequenced DNA.
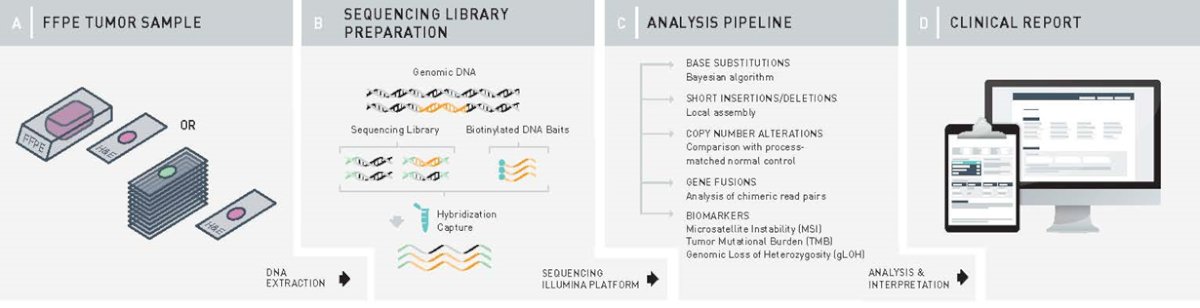
9,411 cases of clinically advanced urothelial carcinoma of the bladder underwent comprehensive genomic profiling (CGP) to examine all classes of genomic alterations (GA). MSI high status, tumor mutational burden (TMB), genomic ancestry, and trinucleotide mutational signatures were determined from the sequencing data. HRDsig status was calculated using a broad set of genome-wide copy number features.2
PD-L1 status was determined by immunohistochemistry using the Dako 22C3 tumor proportional score (TPS) system. Results were compared using Fisher’s exact test with Benjamini-Hochberg adjustment to correct for false discoveries.
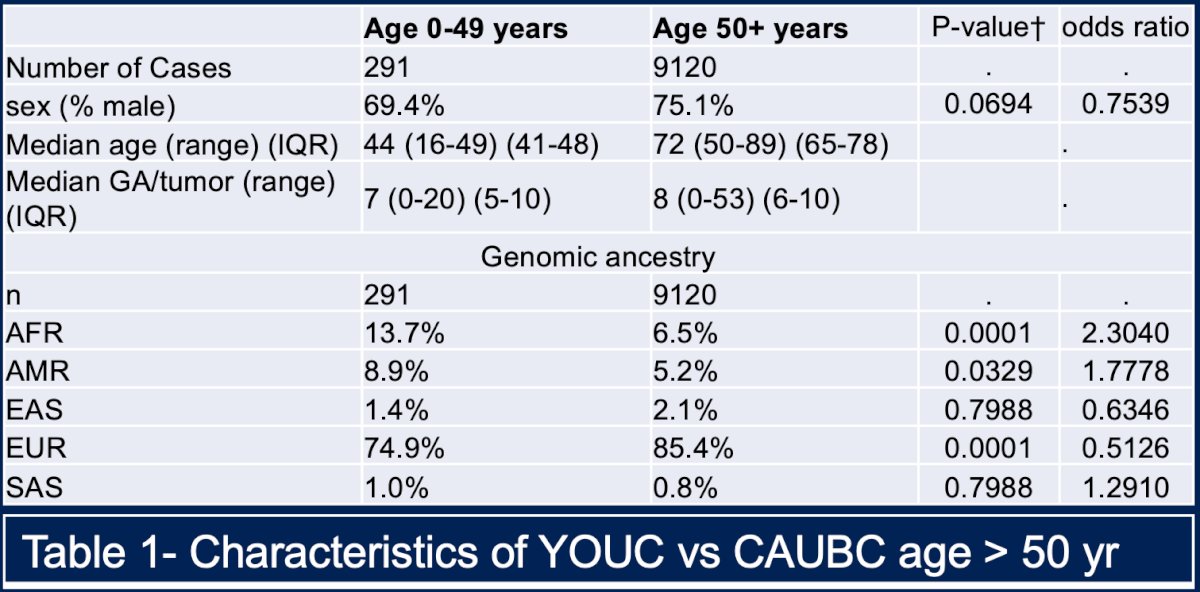
Among all identified young onset bladder cancer patients, 291 (3.1%) had clinically advanced urothelial bladder cancer. The genomic alterations and biomarkers were compared with 9,120 clinically advanced urothelial bladder cancers that developed in patients 50 years of age and older (CAUBC>50).
The proportion of male patients in the CAUBC >50 group was greater than that in the CAUBC <50 cases (75% versus 69%; p=0.07). The number of genomic alterations per tumor was higher in the CAUBC>50 group (8 versus 7; p<0.0001).
Genomic ancestry distribution revealed significantly more African (13.7% vs 6.5%; p=0.0001) and Admixed American (9% vs 5%;p=0.033) cases in the CAUBC <50 versus more European (85% vs 75%; p<.0001) cases in the CAUBC >50 population.
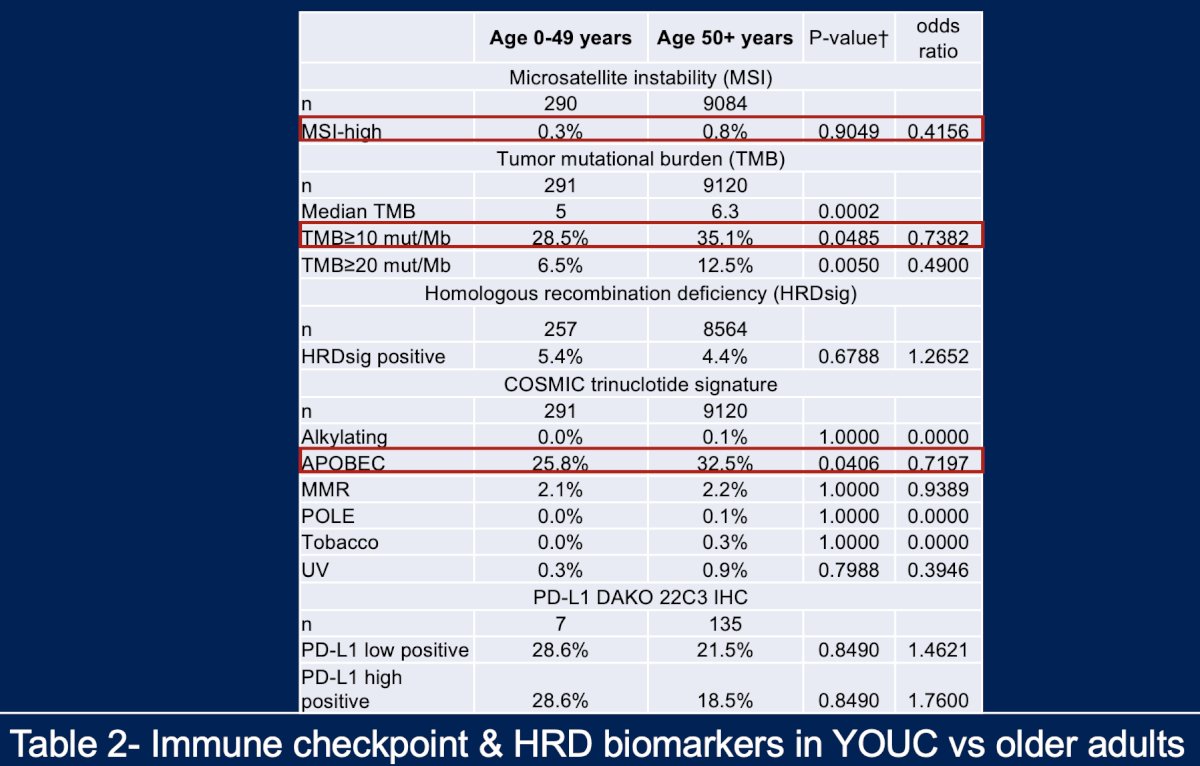
With regards to immune checkpoint and HRD biomarker status, microsatellite instability (MSI) high status was extremely uncommon (0.3–0.8%) in young onset bladder cancer patients. TMB > 10 mutations/Mb was more frequently present in the CAUBC>50 patients (35% vs 28.5%; p=0.048). An APOBEC trinucleotide signature was more frequently observed in the CAUBC>50 patients (32.5% vs 26%; p=0.041).
PD-L1 low expression (1-49% TPS) was available in small subsets of cases and was similar in both groups (21.5% vs 28.6%; p=0.84). APOBEC signatures are associated with higher TMB levels and neoantigen loads, thus potentially impacting immunotherapy drug response.
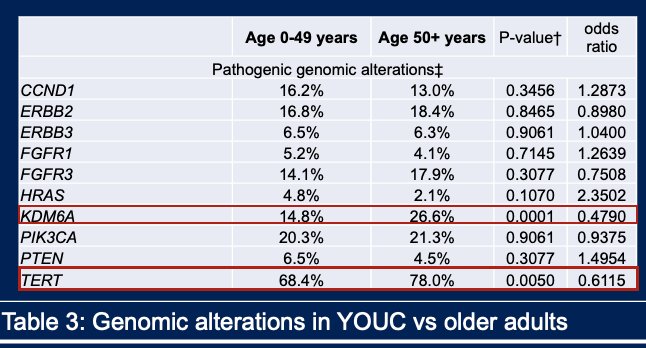
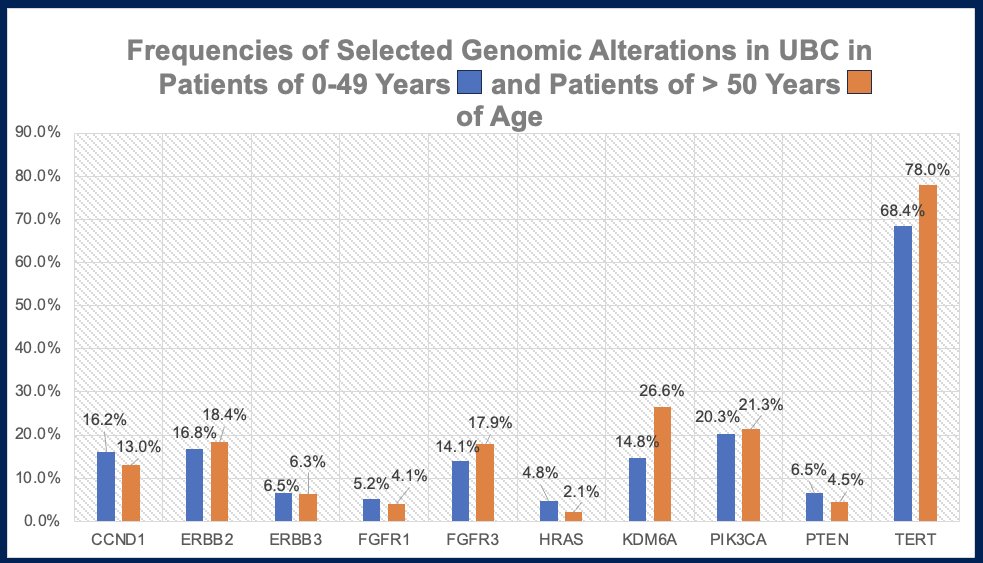
Genomic alterations were more frequently present in clinically advanced urothelial bladder cancer patients <50 years of age:
- HRAS (5% vs 2%; p=0.11),
- CCND1 (16.2% vs 13%; p=0.35)
- pTEN (6.5% vs 4.5%; p=0.30)
However, the frequency of targetable/potentially targetable genomic alterations was not significantly different between groups:
- ERBB2 (18.4% vs 17%; p=0.85)
- ERBB3 (6.3% vs 6.5%; p=0.91)
- MTAP (25% vs 20.3%; p=0.27)
- FGFR3 (14% vs 18%; p=0.31)
Dr. Basnet concluded her presentation as follows:
- 6.5% of clinically advanced urothelial carcinoma of the bladder occurs before age 55 years
- Young onset urothelial carcinoma of the bladder is challenging since survival is shorter, with significant morbidity and loss of productivity (work hours) for the society (42% of young onset urothelial carcinoma of the bladder patients die <55 years of age)
- Biomarkers associated with immune checkpoint inhibitor response, e.g. higher median TMB & TMB ≥10, PDL1 expression are present less frequently in young onset urothelial carcinoma of the bladder patients
- Comprehensive Genomic Profiling data in these young patients demonstrated:
- Differences in the pattern of genomic alterations distributions & putative biomarkers
- The genomic alteration profile is similar for young onset bladder cancer patients and those with clinically advanced urothelial carcinoma of the bladder
- Germline testing & genetic counseling is critical for these patients
- The plan is to expand this effort via the large BCAN-IBCG initiative on young onset bladder cancer patients
Presented by: Alina Basnet, MD, Guthrie Cortland Medical Center, Syracuse, NY
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: Genomic Characterization of Young-Onset Bladder Cancer - Alina Basnet
References:
- Stenzl A, Cowan NC, De Santis M, et al. Treatment of muscle-invasive and metastatic bladder cancer: update of the EAU guidelines. Eur Urol. 2011; 59(6):1009-18.
- Moore JA, Chen KT, Madison R, et al. Pan-Cancer Analysis of Copy-Number Features Identifies Recurrent Signatures and a Homologous Recombination Deficiency Biomarker to Predict Poly (ADP-Ribose) Polymerase Inhibitor Response. JCO Precis Oncol. 2023; e2300093.